
Abstract
Gallbladder injuries are extremely rare in blunt trauma, with a reported incidence of <2%. We report an autopsy case of fatal hemorrhagic shock due to intra-abdominal bleeding resulting from complete avulsion of the gallbladder associated with liver cirrhosis. Multiplanar images derived from multislice computed tomography (MSCT) performed as part of pre-autopsy screening showed complete avulsion of the gallbladder without any other associated intra-abdominal injuries, facilitating forensic autopsy planning. In this report, we discuss the role of MSCT in cases of fatal intra-abdominal bleeding caused by avulsion of the gallbladder and discuss the mechanism of this injury.
Keywords
Since the gallbladder is afforded substantial anatomic protection from external blunt forces, complete detachment of the gallbladder from its hepatic bed is a very rare occurrence. However, its position does not afford complete protection from blunt injuries, particularly from a forceful localized blow. Soderstorm et al. reported a 2.1% incidence of gallbladder trauma in 1449 patients with blunt abdominal trauma (1). In this case report, we describe an autopsy case of fatal intra-abdominal bleeding caused by avulsion of the gallbladder as suggested by findings from a multislice computed tomography (MSCT) examination that were corroborated at forensic autopsy. We also discuss the mechanism of injury.
Case report
Scene of death
A man in his 40s with a history of chronic alcohol abuse and mental illness was found dead at home. His brother alleged that he hit the deceased's head and face while under the influence of alcohol, but in a deposition he denied hitting the deceased in the abdomen. During the police investigation, the veracity of the brother's account could not be determined because he was intoxicated at the time of the incident. He also had a mental illness. Therefore, the body was transported to our institution for a forensic autopsy in order to clarify whether the death was the result of a crime or an accident.
MSCT data acquisition and findings
Postmortem CT for pre-autopsy screening was performed with an eight-channel multislice scanner (Aquilion; Toshiba Medical Systems, Tokyo, Japan). Images were reconstructed with soft tissue, lung, and bone kernels to provide 2.0 mm slices each. MSCT data were sent to a digital imaging and communication in medicine (DICOM) server (POP-Net Server; ImageONE, Tokyo, Japan) and a three-dimensional workstation (ziostation ver. 2.1.0.3; Ziosoft, Tokyo, Japan). All CT images were evaluated by an experienced radiologist.
On postmortem CT, a moderate amount of blood was identified in the right perihepatic and perisplenic spaces, respectively (Fig. 1a). The gallbladder could not be visualized in situ (Fig. 1b). It was lying in a high-attenuation material (suspected to be blood) in the inferior abdomen, detached from its liver bed and filled with a large amount of bile, some gallstones, and biliary sludge (Fig. 1c, d, e). Its fundus was at the lower pole of the right kidney (Fig. 1d). Clotted blood was evident in the liver bed (Fig. 1b). No other hepatic parenchymal injuries were visible on CT. Other CT findings included fatty liver, fractures of the fourth to ninth left ribs, and cerebral edema. Pneumothorax and hemothorax were not found.

Postmortem CT images of the abdomen showing gallbladder avulsion and associated abdominal bleeding. (a) A moderate amount of blood can be identified in the perisplenic and right perihepatic spaces (white arrows). (b) The gallbladder is missing from the liver bed. Clotted blood is confirmed in the gallbladder fossa (white arrow heads). (c) Gallstones and biliary sludge were found in the fundus of gallbladder; the fundus is located near the lower pole of the right kidney in a high-attenuation material (asterisk). (d) A sagittal image reveals complete avulsion of the gallbladder containing gallstones, with displacement of the gallbladder from its fossa so that it lies in a high-attenuation material in the inferior abdomen. (e) A coronal image also shows complete avulsion of the distended gallbladder
Autopsy findings
Following MSCT scanning, forensic autopsy was performed with the guidance of radiologic findings. The cadaver was 170 cm long and weighed 92 kg. The subcutaneous tissue of the head was edematous. The brain weighed 1200 g, with slight swelling of the surface. No intracranial bleeding was identified. Slight amounts of subcutaneous hemorrhage were widespread in the upper abdomen. Massive subcutaneous hemorrhage was seen around the left thoracic and left hip region. The eighth right costal cartilage and the fifth and sixth left costal cartilages were fractured. The multiple bilateral rib fractures were found without pleural injury. There were no lacerations and hemorrhage in both lungs. The distended gallbladder was completely stripped from its liver bed (Fig. 2) and hanging from an intact cystic duct with adherent coagulated material. The gallbladder was filled with dark green bile (110 mL) and three gallstones, and associated with massive intra-abdominal bleeding (900 mL). There was no extrahepatic bile duct injury or evidence of bile leak. The presence of clotted blood was confirmed on the liver bed. The liver weighed 1580 g; the appearance of its external surface was irregular, nodular, and yellow. The cut surface also had a yellow granular appearance suggestive of cirrhosis. No other pathological abnormalities were found in the abdomen.
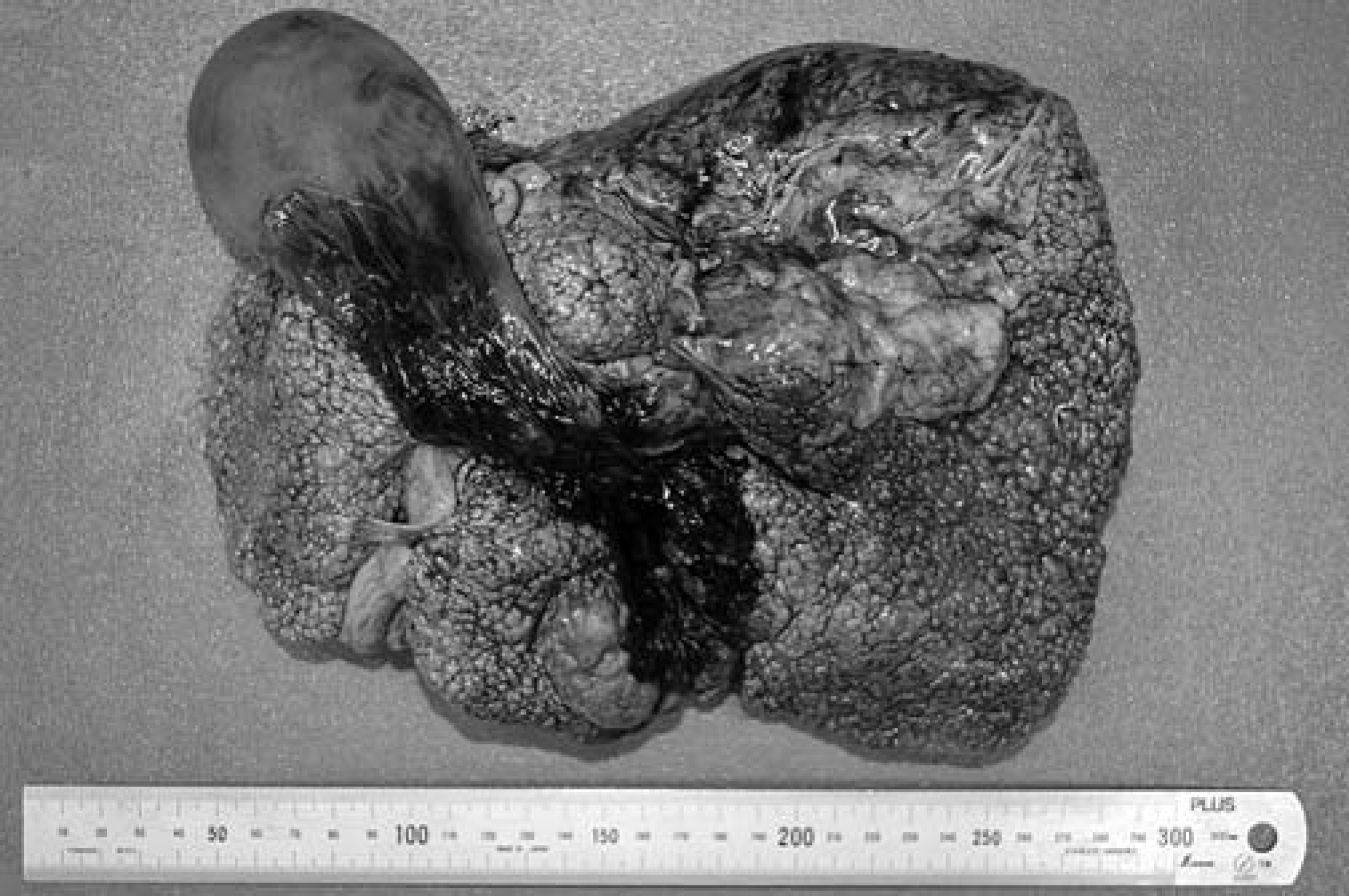
Gross appearance of the liver. The gallbladder is detached from the liver bed. The liver shows signs of cirrhosis
The blood alcohol concentration was 0.8 mg/mL. As mentioned above, we confirmed that the brain and lungs showed no significant pathological alteration, and therefore concluded that the cause of death was hemorrhagic shock due to intra-abdominal bleeding from avulsion of the gallbladder.
Discussion
This report is a rare case of death due to gallbladder injury; MSCT and autopsy revealed bleeding from an avulsion injury of the entire gallbladder without any other associated intra-abdominal injuries. In such cases, since the exact relationship between the gallbladder and the gallbladder fossa can be difficult to appreciate on axial CT images alone, reconstructed coronal and sagittal images can be very useful (2), especially in assisting the planning for a forensic autopsy to establish the cause of death. Recently, it was reported that new acquisition techniques such as dual-energy CT could provide additional information (3).
The gallbladder is a well-protected organ, being partially embedded in the relatively large liver, cushioned by the surrounding omentum and intestines, and covered by the bony and cartilaginous rib cage (1, 4, 5). However, it has been reported that the spectrum of gallbladder injuries includes contusion, laceration, and avulsion (6). Avulsion results in partial or complete tearing of the gallbladder from the liver bed, and may also involve the cystic duct and artery. Consequently, the gallbladder lies free in the abdomen (1). Based on Losanoff and Kjossev's (7) more detailed classification of blunt gallbladder injuries, the current case is type 3B; namely, isolated complete avulsion of the gallbladder, or near cholecystectomy.
Shearing forces are major contributors to avulsion injuries of the gallbladder (1). Considering the difference in mass between the gallbladder and liver, it would seem reasonable to postulate that exposure to acceleration and deceleration forces could result in shearing forces between these two organs (2). A fully distended gallbladder, as seen in our case, has increased mass compared to a small, contracted gallbladder. Additionally, the victim had firm, cirrhotic hepatic parenchyma. The increased mass of the fluid-filled gallbladder and the more solid consistency of the liver parenchyma may have amplified these shearing forces. The presence of multiple bilateral rib fractures and subcutaneous soft tissue bleeding around the left hip indicated that external blunt forces, such as a number of forceful kicks or blows to the body, occurred several times during a fight. We suspect that these forces, amplified by the fluid-filled gallbladder and firm liver, led to avulsion of the gallbladder. The firmness of the cirrhotic liver parenchyma may be thought of as a dysfunctional shock absorber in the face of external blunt force (8).
Cholecystic venous branches communicate directly with intrahepatic portal venous branches around the gallbladder fossa (9). In our case, the gallbladder was completely avulsed and it was natural to suppose that bleeding was due to damage to these vessels. The formation of blood clots suggested a survival time of several minutes. Steady hemorrhage from the damaged vessels of the gallbladder and liver bed is likely to have resulted in a fatal volume of blood loss. Clinically, there is a higher incidence of death due to blunt trauma than penetrating trauma, as the symptoms and signs of blunt trauma can be more insidious, thereby causing delays in diagnosis (10).