
Abstract

Most people with hypertension or diabetes will develop structural heart disease, which might cause renal water and salt retention and, eventually, symptoms and signs of congestion: simply, heart failure. 1 Most modern definitions of heart failure couple the notions of symptoms (e.g. breathlessness or ankle swelling), an abnormality on imaging (such as a reduced left ventricular ejection fraction (LVEF)) and raised plasma concentrations of natriuretic peptides. 2 For many individuals, there must be a long, preclinical phase of cardiac dysfunction. 3 , 4 Intervening before the onset of symptoms may offer the best opportunity to delay their onset, change the disease trajectory and prolong active life. This requires screening of asymptomatic people, usually those at greater risk of developing heart failure, to identify preclinical cardiac dysfunction. This is an enormous undertaking. The population to be screened should be well defined, the screening tools should be simple and robust and the definitions of what is abnormal must be clear. For those who test ‘positive’, the risk of morbidity, disability and death should be sufficiently high to warrant intervening and there should be an actionable intervention that reduces these risks.
There is some evidence that asymptomatic individuals with a substantially reduced LVEF (i.e. <40%) might benefit from treatment with angiotensin-converting enzyme inhibitors, beta-blockers, mineralocorticoid receptor antagonists and probably statins, especially those with a history of myocardial infarction. 5 However, screening of asymptomatic patients with hypertension or diabetes identifies rather few people with LVEF less than 40%, 6 even though many may have had an undiagnosed myocardial infarction. 7 Measurement of global longitudinal strain (GLS) might be more sensitive than LVEF in identifying more subtle left ventricular systolic dysfunction, but it requires more sophisticated technology and equipment, personnel and skills, and additional time for obtaining good quality images and for their analysis. 8 Of note, there is no evidence that treating a patient with an impaired GLS is beneficial when LVEF is normal. There are many other sophisticated methods of imaging cardiac function that are associated with a greater risk of events, but none has been shown to be useful in selecting patients for treatment. 9 On the other hand, there is some evidence that selecting patients for treatment based on plasma concentrations of natriuretic peptides may be useful.10–12
In the current issue of this journal, Morbach and colleagues used the characteristics and course of heart failure stages A–B and determinants of progression (STAAB) cohort study to assess the prevalence of heart failure precursor stages in the general population. 13 They enrolled a representative sample (n = ∼5000) of residents of Wuerzburg (n = 124,297), Germany, aged 30–79 years. In the derivation cohort (n = 2473), 42% of participants were in stage A (that is, risk factors for heart failure but without evidence of cardiac dysfunction on imaging) and 17% were in stage B (evidence of structural heart disease, including a reduced LVEF, diastolic dysfunction or valve disease) but without symptoms such as exertional breathlessness or ankle swelling. Surprisingly, only seven patients had structural heart disease with symptoms (i.e. undiagnosed heart failure; stage C). Interestingly, they also identified a substantial proportion of participants (n = 131, 5%) with structural heart disease who had no risk factors (called stage B-not-A). These findings were confirmed in an internal validation cohort (n = 2492), in which 9% were found to be in stage B-not-A.
A large proportion of stage B-not-A individuals were young women (78%; mean age 47 years) who were reported to have impaired systolic function (32%) or a dilated left ventricle (72%) by echocardiography, but they often had a normal plasma N-terminal pro brain natriuretic peptide (NT-proBNP) (median 54 (28–94) ng/l, which is the expected median value for healthy women aged 40–50 years) 14 and most (95%) had normal left atrial volumes. Their plasma NT-proBNP and left atrial volumes were similar to those in stage A (NT-proBNP 56 (27–106) ng/l, and 7% left atrial dilation, respectively), and also similar to those without risk factors (NT-proBNP 42 (21–78) ng/l) and 2% left atrial dilation).
Compared to patients in stage B-not-A, those in stage B were about 15 years older and were more likely to have valve disease or left atrial dilatation (22%) and had a lower mean LVEF (56 (7)% vs. 59 (6)%) and higher NT-proBNP (median 95 (54–179) ng/l). This suggests that participants in stage B-not-A had less or milder structural heart disease compared to stage B (Figure 1).
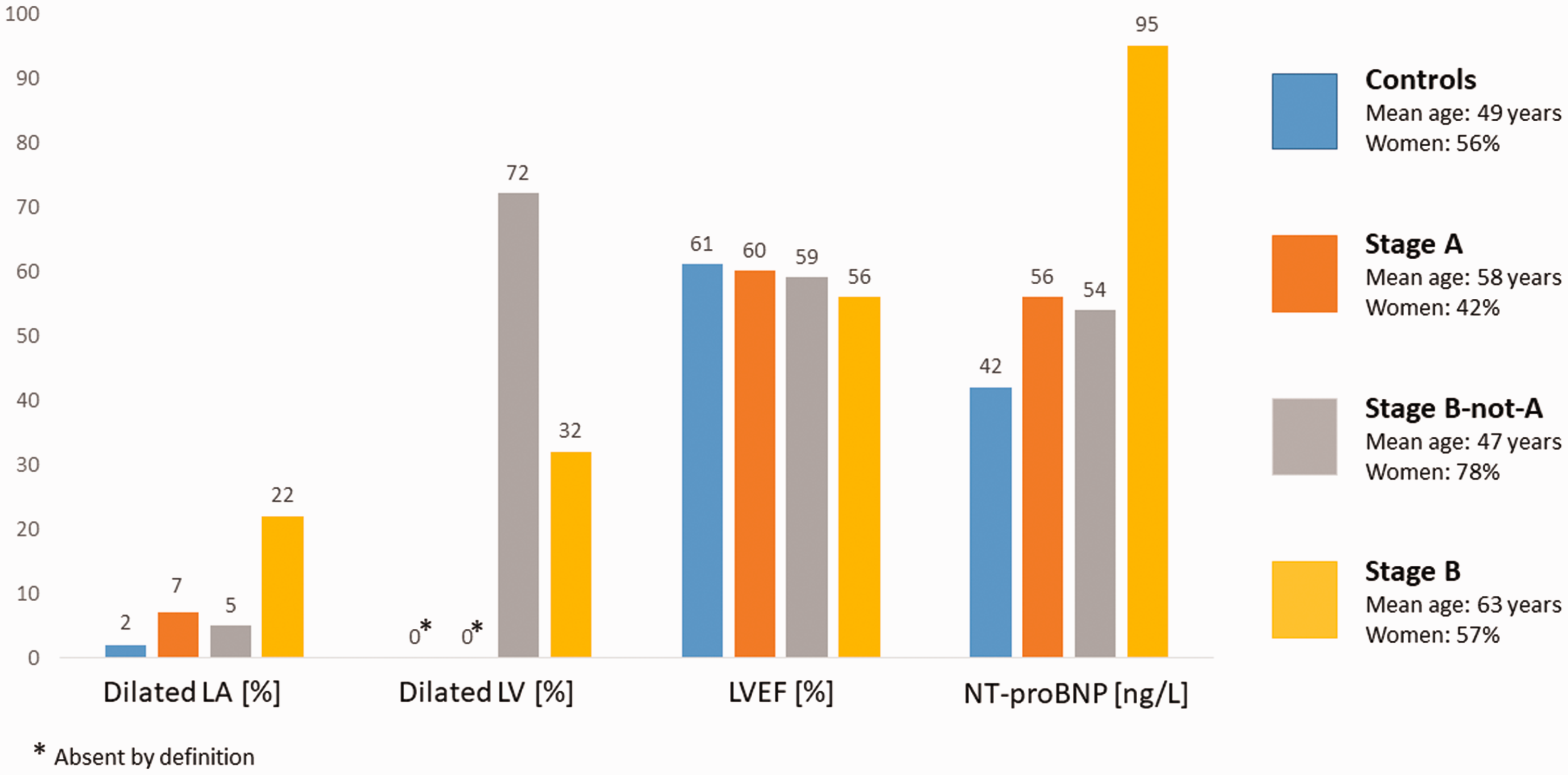
Key baseline characteristics in the STAAB cohort (derivation sample).
Omissions and errors will have accounted for some people in stage B having no record of risk factors. Definitions of structural heart disease are arbitrary. Values for some people with disease will remain in the ‘normal’ range and some people without disease will be beyond the 95% confidence limits of the normal range; these will often be people who go to the gym or engage in sports, 15 which was not uncommon for these individuals. The high prevalence of left ventricular dilation as a criterion for structural heart disease for those identified as ‘B-not-A’ might also be because measurements were overestimated when adjusted for body size: by definition, those B-not-A could not be obese. Finally, measurement precision and reproducibility may account for some patients being classified inaccurately.
The left atrium is a thin-walled cardiac chamber that is exposed to the same internal pressure as the much thicker-walled left ventricle during diastole. A chronic increase in left ventricular filling pressure, regardless of cause, should lead to atrial remodelling, increasing the risk of atrial fibrillation and reduce atrial performance 16 thereby contributing to the development of heart failure. A rise in atrial and ventricular diastolic pressures and wall stress should also cause plasma concentrations of NT-proBNP to increase. NT-proBNP is one of the most powerful prognostic markers in patients with cardiovascular disease but is fairly agnostic as to the cause of cardiac dysfunction. Up to 50% of patients with hypertension, coronary artery disease or diabetes have elevated plasma concentrations of NT-proBNP, which indicates an adverse cardiovascular outcome. 17 Therefore, a dilated and dysfunctional left atrium and elevated plasma NT-proBNP might be the most appropriate markers to quantify cardiac dysfunction rather than measurements of left ventricular structure and function that are complex and prone to measurement error. NT-proBNP might be the preferred screening test for population studies and in primary care because it can be measured at the same time as other routine blood tests, with little additional costs. Low plasma concentrations do not require further investigation of cardiac function and provide reassurance to patients and their doctors. Emerging evidence suggests that the identification and treatment of individuals at risk of heart failure who have modest increases in plasma NT-proBNP improves adverse cardiac remodelling, and perhaps outcome.10–12 The reasons for any increase in NT-proBNP should be considered. Atrial fibrillation may be identified by physical examination and confirmed by electrocardiography. Renal dysfunction can be identified by measuring serum creatinine in the same blood test as NT-proBNP. Patients with a history of hypertension who do not have a murmur or history of myocardial infarction and who have only modest increases in plasma NT-proBNP (perhaps 125–500 ng/l) are likely to have left ventricular hypertrophy and developing diastolic left ventricular dysfunction. Those with more marked increases in plasma NT-proBNP or with a murmur or history of myocardial infarction should have an echocardiogram.
In summary, if cardiac imaging suggests that there is structural heart disease but this is not associated with a dilated left atrium and elevated plasma concentrations of NT-proBNP, then either the imaging measurements are wrong or the structural disease has no important effect on cardiac performance. It is likely that stage B-not-A includes many people with an excellent prognosis. Long-term follow-up is required to prove that this is the case.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the British Heart Foundation Centre of Research Excellence grant number RE/18/6/34217 and the Heart Research UK (Scotland grant).