
Abstract

There is a small but significant increase in the risk of sudden cardiac death (SCD) during and shortly following strenuous exercise. Can these tragic events be prevented? In the current issue of the journal, D’Ascenzi et al. present a survey to map the use of imaging in the pre-participation evaluation and to explore physician beliefs and potential barriers that may influence individual practices. 1 The authors found that echocardiography was frequently used as a first-line evaluation tool in athletes. Routine evaluation by echocardiography in asymptomatic athletes has been debated for years. What does echocardiography add, and can echocardiography as a first-line tool be justified?
Athletes are, in general, healthy and have a life expectancy that exceeds that of the normal population. 2 The estimated incidence of sports-related SCD is one to two per 100,000 athletes per year in 12–35-year-old individuals. 3 The same incidence was found in a Danish cohort, in which no systematic pre-participation evaluation was mandated. 4 Interestingly, the comparative incidence of SCD among individuals in the same age group from the general population was 3.76 per 100,000 individuals per year. 4 As such, is a systematic evaluation of these healthy athletes needed?
The European Heart Rhythm Association and the European Association of Preventive Cardiology recommend a cardiovascular evaluation, including medical history, physical examination and a 12-lead electrocardiogram (ECG) for all athletes. 1 ECG has a low cost and high availability, and many cardiomyopathies and channelopathies present with early ECG changes. 3 With new and improved guidelines for interpreting athletes’ ECGs, the false positive and false negative rates have been significantly reduced. However, adding ECG to the cardiovascular evaluation of athletes has been widely debated, and we are missing randomised studies on the usefulness of ECG in the pre-participation examination. Notably, the documentation of the preventive benefits of ECG assessment is primarily based on the findings of one observational study, 5 that have not been reproduced in other cohort. 6 , 7
The use of transthoracic echocardiography as a first-line evaluation tool lacks evidence of incremental diagnostic value to ECG alone. 3 Despite the limited documentation, echocardiography in pre-participation evaluation guidelines has been implemented by large and influential sports societies, such as the Union of European Football Associations.
The challenges of echocardiography as a first-line evaluation tool are addressed by several studies. Malhotra and colleagues studied the use of echocardiography in the evaluation of 11,168 young athletes, reporting SCD in eight athletes (0.07%) during a mean follow-up of 10.6 years. 8 In total, six of these had normal cardiac screening results at baseline. 8 Another screening study that used ECG and echocardiography in the pre-participation evaluation of 595 professional soccer players reported six serious cardiovascular events during a follow-up of 8 years. All six subjects had normal baseline echocardiographic examinations assessed by experienced cardiologists. 9
Considering the increasing use of echocardiography in the primary evaluation of low-risk athletes, the study of D’Ascenzi and colleagues adds important information. 1 The study presents data on how more than 600 physicians involved in the cardiovascular evaluations of athletes view the role of echocardiography as part of pre-participation evaluation. The survey shows that 65% of the physicians used echocardiography routinely as part of the pre-participation evaluation of asymptomatic athletes. Interestingly, only 28% of the physicians suggested that repeated echocardiography should be limited to individuals with an abnormal finding. The authors concluded that their findings indicate that the clinical community has moved beyond the debate of whether or not to include an ECG as part of the cardiovascular evaluation, and that further work should focus on the optimal use of cardiovascular imaging in evaluating cardiovascular risk in athletes.
This survey is highly interesting. Why do we clinicians feel that echocardiography has incremental value in the pre-participation evaluation, despite the current lack of documentation? Is it because we believe it to be the best clinical practice? Is it because the sports societies are increasingly mandating echocardiography in pre-participation evaluation? Are there other reasons? These questions unfortunately remain unanswered.
Adding echocardiography to all pre-participation evaluations comes with a cost, both to society and the individuals assessed. Malhotra and colleagues estimated an additional cost of £73 per evaluation when echocardiography was added on top of the current pre-participation screening programme. This implies an additional cost of £7,300,000 per 100,000 individuals, in addition to an unknown number of repeated or additional examinations due to uncertain findings. 8 The estimated incidence of sports-related SCD is one to two per 100,000 athletes per year in 12–35-year-old individuals. In addition, about 2% of the screened athletes (n=2000) are likely to be advised to stop sports participation due to false positive findings. 5 In the survey by D’Ascenzi et al., 1 most respondents (54%) advocated repeated echocardiography every 1–2 years during an athlete’s career, suggesting extensive costs for implementing a screening programme, including echocardiography.
As identified by the survey, echocardiography has benefits, particularly in identifying cardiomyopathies and structural abnormalities. The authors discuss different strategies of making echocardiography more accessible as a first-line tool, suggesting short protocols of only 2–5 minutes’ duration. However, separating physiological adaptations from early stages of cardiomyopathy is difficult (Figure 1), requiring comprehensive and often additional assessments.10–12 Furthermore, neither echocardiography nor ECG can predict premature coronary artery disease and myocarditis, two major contributors to SCD in athletes. Finally, a significant percentage of sports-related SCD remain unexplained. 13
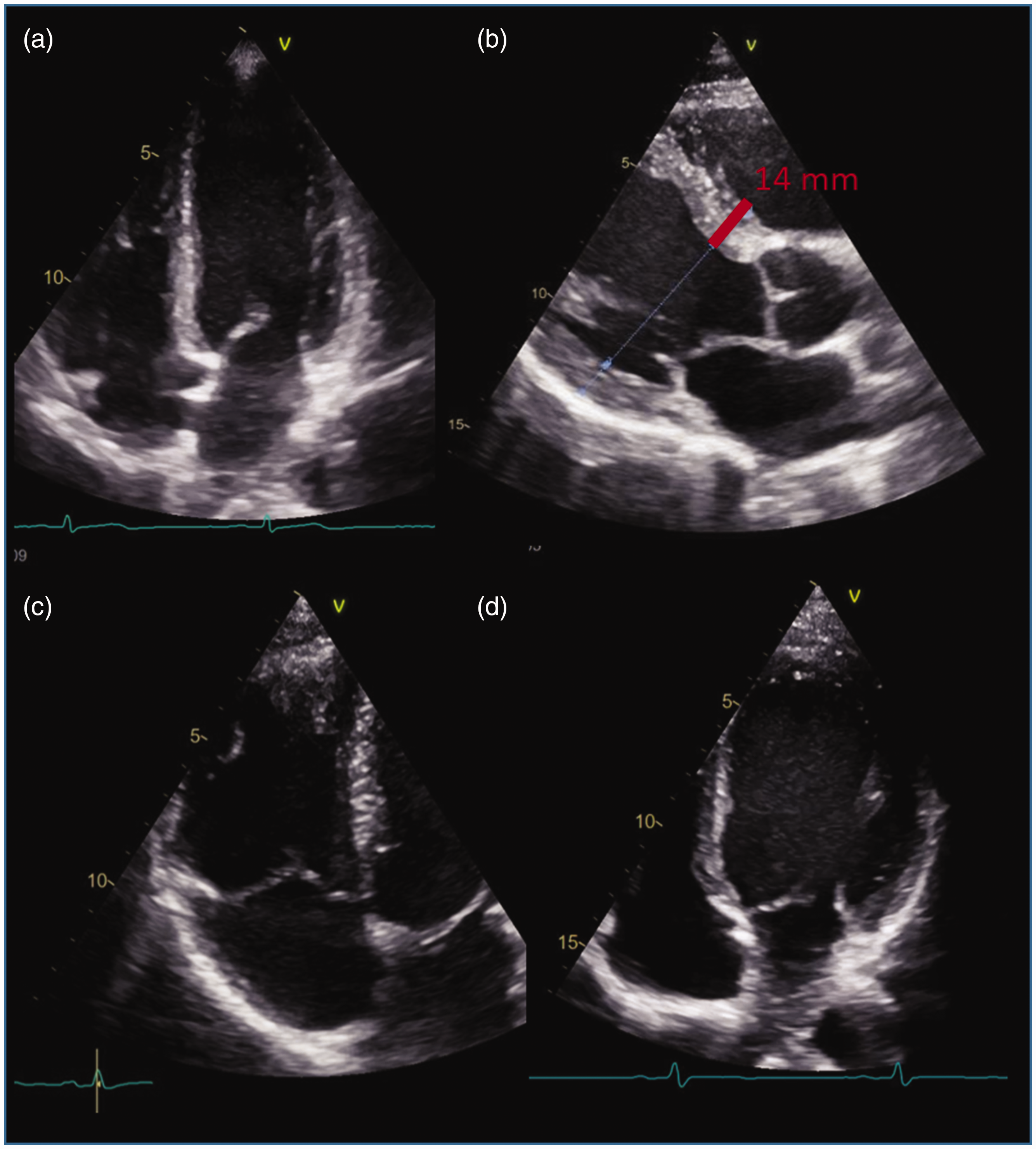
Echocardiography of athletes might show only slight adaptations to exercise (a), but findings of left ventricular hypertrophy (b) and dilatation of the right (c) and left (d) ventricle might be challenging to differentiate from pathological conditions. These images were obtained from studies on healthy recreational athletes.
Choosing to do fewer tests requires education and courage, but sometimes less is more. A careful medical history, including specific questions about family history of arrhythmias/palpitations/unclear cardiac history and deaths at young ages, is pivotal. Echocardiography remains essential in the assessment of athletes with signs or symptoms indicating underlying cardiac pathology. However, in our opinion, the cost-benefit of echocardiography needs better elucidation before it can reach a general recommendation in the pre-participation evaluation of low-risk asymptomatic individuals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.