
Abstract

Cardiovascular disease (CVD) remains the main cause of death worldwide, accounting for 44% of all non-communicable disease deaths, of which most are attributable to coronary heart disease (CHD). 1 Coronary artery calcification (CAC) has a strong association with major cardiovascular events and mortality, and has a high risk-predictive value of CHD in asymptomatic individuals.2,3 It has been argued that the amount of CAC, expressed in the CAC score, can be used in population-based screening.
The Dutch Risk Or Benefit IN Screening for CArdiovascular disease (ROBINSCA) trial is the first large-scale population-based randomised controlled trial (RCT) to investigate whether CAC screening followed by preventive treatment is effective in reducing CHD-related morbidity and mortality in asymptomatic individuals.4,5 The aim of this study was to investigate the CAC prevalence and predictors in the ROBINSCA trial, which included an asymptomatic high-risk potential target population from the general population.
The rationale and design of the ROBINSCA trial have been described before.
5
Briefly, 43,447 potentially high-risk women (55–74 years) and men (45–74 years) from the national population registry who completed a baseline questionnaire to assess sociodemographic and health characteristics and gave informed consent were randomly allocated (1:1:1) to either the control arm, intervention arm A (screening according to traditional risk factors) or intervention arm B (CAC screening). The current study focuses on the CAC screening arm (Figure 1
Flowchart of the ROBINSCA trial study design in which CAC scoring is performed in intervention arm B. BMI: body mass index; CAC: coronary artery calcium; CHD: coronary heart disease; CT: computed tomography; CVD: cardiovascular disease; CVRM: cardiovascular risk management; SCORE: systematic coronary risk evaluation.
CAC screening was performed using computed tomography scanning to identify CVD risk according to the CAC score, which represents the total amount of any CAC. 6 CAC scores were categorised into low (Agatston 0–99), high (Agatston 100–399) and very high (Agatston ≥ 400) risk. 2
The effects of baseline characteristics on CAC score were analysed using a two-step approach regression analyses for modelling presence, both any CAC and CAC score of 400 or higher (multivariable backward logistic regression), and extent (multivariable backward linear regression of the log-transformed CAC score) of CAC in women and men separately. Variables included in the models were age, educational level, waist circumference cut-off (88 cm for women and 102 cm for men), body mass index (BMI) cut-off (30 kg/m2), family history of CHD, smoking, diabetes mellitus, hypertension and/or hypercholesterolemia in the past year, and baseline use of either antihypertensive or lipid-lowering medication (according to self-reported data from the baseline questionnaire). A P value of less than 0.05 was considered statistically significant. All analyses were performed using IBM SPSS Statistics version 24.0.
Of the 12,950 screened participants, 48.1% were women and 94.2% were born in The Netherlands. The median age was 64 years in women and 62 years in men. Regarding CVD risk factors, 20.0% were current smokers at baseline, 3.4% reported diabetes mellitus, 16.4% and 15.3% reported being diagnosed with hypertension and hypercholesterolemia, respectively, in the year before baseline, and 44.9% reported a family history of CHD.
CAC was absent in 39.2% of the total study population. Overall, 48% of women had a zero CAC score compared to 20.7% of men in the same age category and 31.2% of all men. Furthermore, 16.8% of women had a CAC score of 100 or higher compared to 40.0% of men in the same age category and 30.7% of all men. The CAC distribution in the ROBINSCA trial is compared to the German Heinz Nixdorf Recall Study and the American Multi Ethnic Study of Atherosclerosis in the Supplementary material.
Baseline predictors for the presence and extent of coronary artery calcium and for a coronary artery calcium score of 400 or higher.
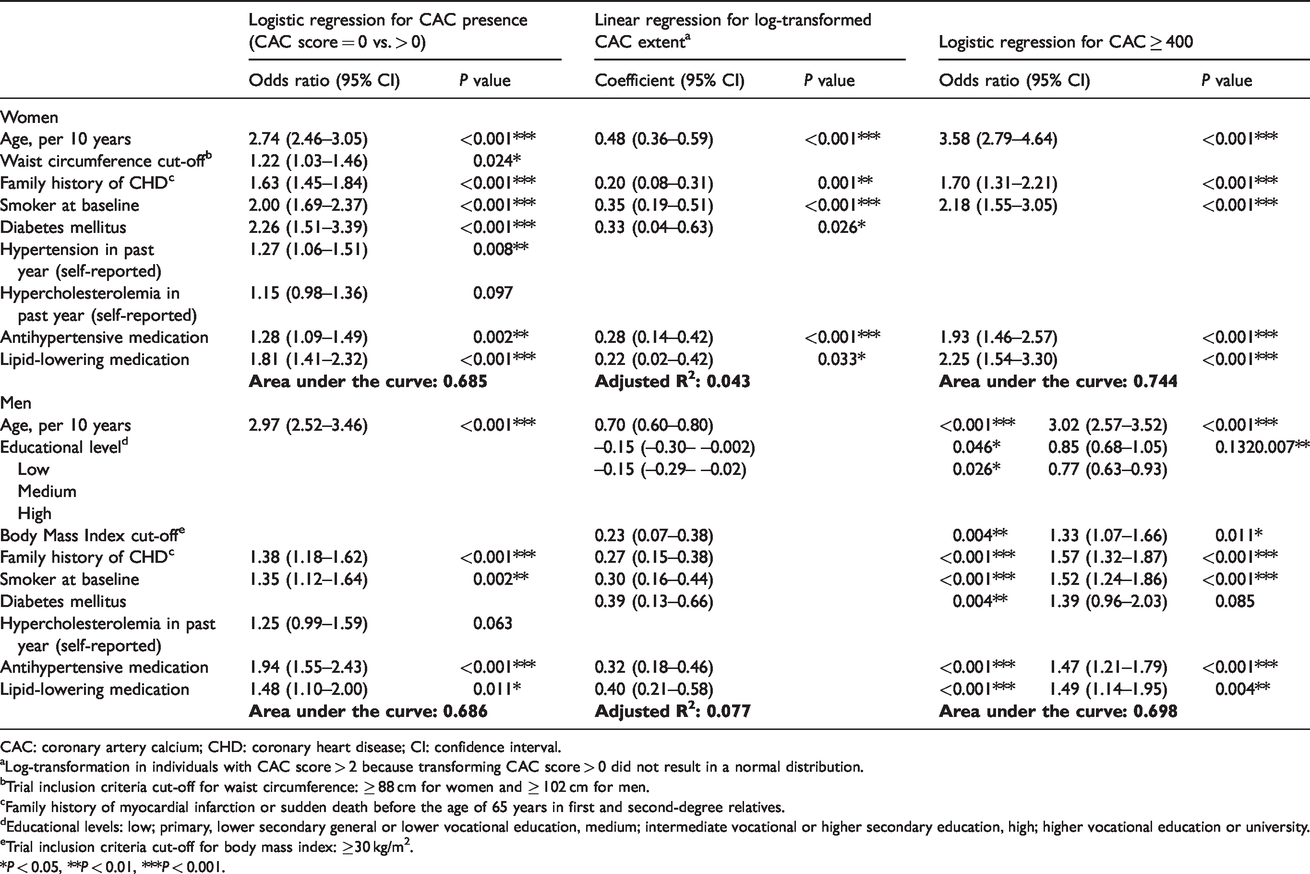
CAC: coronary artery calcium; CHD: coronary heart disease; CI: confidence interval.
aLog-transformation in individuals with CAC score > 2 because transforming CAC score > 0 did not result in a normal distribution.
bTrial inclusion criteria cut-off for waist circumference: ≥ 88 cm for women and ≥ 102 cm for men.
cFamily history of myocardial infarction or sudden death before the age of 65 years in first and second-degree relatives.
dEducational levels: low; primary, lower secondary general or lower vocational education, medium; intermediate vocational or higher secondary education, high; higher vocational education or university.
eTrial inclusion criteria cut-off for body mass index: ≥30 kg/m2.
*P < 0.05, **P < 0.01, ***P < 0.001.
The associations of age, male sex, diabetes mellitus and smoking with higher CAC scores are well known. 7 A lower socioeconomic status, indicated by educational level, significantly predicted a higher extent of CAC in men. This association is possibly a result of a less favourable lifestyle in terms of smoking, diet and physical activity. 8 Diabetes mellitus was one of the strongest predictors of CAC presence in women. This is in line with previous research in which diabetes mellitus was identified to have a greater impact in women compared to men. 9 Moreover, diabetes mellitus was a strong predictor for CAC extent in both sexes, suggesting that it is the most important risk factor for CAC development after sex and age. Regarding BMI and waist circumference, our results confirm earlier findings that BMI is not a strong predictor for the presence of CAC, while waist circumference is more predictive of CAC presence. 10 The predictive value of the baseline use of either antihypertensive or lipid-lowering medication in CAC development was also seen in previous research. However, statins have been associated with increased CAC scores, but not with more CVD events. It is suggested that statins induce CAC progression and, at the same time, plaque repair. 11
This study contributes to evidence on identifying the optimal target population for screening from the general population that will gain most healthy life-years from screening and subsequent treatment. All inclusion criteria for the ROBINSCA trial (smoking, waist circumference, BMI and a family history of CHD) were statistically significant predictors of CAC. Future analyses should provide evidence on whether the study population includes individuals who benefit most.
A main limitation is that the ROBINSCA population is not representative of all ethnic groups as a result of a homogeneous distribution, although ethnicity is known to affect CAC prevalence and severity. Another possible limitation is that study participants tend to be generally healthier than similar individuals not responding to the participation invitation (healthy volunteer effect). However, the inclusion and exclusion criteria should have minimised this effect. Furthermore, participants using both cholesterol-lowering and antihypertensive medication were excluded from the trial, which might have affected the found associations of CAC with CVD medication. Finally, baseline data were obtained using a self-reported questionnaire, rather than diagnostic test measures, and might entail some inaccuracies.
In conclusion, this currently largest population-based RCT for CAC screening in asymptomatic middle-aged Caucasian individuals showed that 30.7% of men and 16.8% of women with a CAC score of 100 or greater urgently require preventive treatment. To a large extent, male sex and increasing age, followed by diabetes mellitus and smoking, influence CAC distribution. These results can therefore help determine the best risk prediction and prevention strategy should screening for a high risk of developing CVD be (cost)-effective.
Supplemental Material
sj-pdf-1-cpr-10.1177_2047487320932263 - Supplemental material for Screening for coronary artery calcium in a high-risk population: the ROBINSCA trial
Supplemental material, sj-pdf-1-cpr-10.1177_2047487320932263 for Screening for coronary artery calcium in a high-risk population: the ROBINSCA trial by Sabine JAM Denissen, Carlijn M van der Aalst, Marleen Vonder, Jan Willem C Gratama, Henk J Adriaansen, Dirkjan Kuijpers, Jeanine E Roeters van Lennep, Rozemarijn Vliegenthart, Pim van der Harst, Richard L Braam, Paul RM van Dijkman, Matthijs Oudkerk and Harry J de Koning in European Journal of Preventive Cardiology
Footnotes
Acknowledgements
The author(s) would like to thank the European Union for funding the ROBINSCA trial and the Ministry of Health, Welfare and Sports for the ethical approval to perform the trial. Naturally, The author(s) thank all participants for their participation. Furthermore, they would like to thank M Quak for the extensive research assistance, RADventure for developing the data management system and the IVA group for handling all questionnaires and letters. Finally, they thank all employees of the radiology departments of the screening centres (Gelre Hospital Apeldoorn, Bronovo Hospital The Hague and University Medical Centre Groningen) for scanning participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ROBINSCA trial was funded by an advanced grant (agreement no. 294604) of the European Research Council.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.