
Abstract
Aims
The purpose of this study was to analyse the association of leisure-time physical activity of different intensities at baseline, and cardiovascular disease incidence, cardiovascular disease mortality and all-cause mortality in a population-based sample of 60-year-old men and women with and without established metabolic syndrome, for more than 20 years of follow-up. A secondary aim was to study which cardiometabolic factors may mediate the association between physical activity and long-term outcomes.
Methods
A total of 3693 participants (53% women) underwent physical examination and laboratory tests, completed an extensive questionnaire at baseline 1997–1999 and were followed until their death or until 31 December 2017. First-time cardiovascular disease events and death from any cause were ascertained through regular examinations of national registers.
Results
Metabolic syndrome prevalence was 23.0%. In metabolic syndrome participants, light physical activity attenuated cardiovascular disease incidence (hazard ratio = 0.71; 95% confidence interval 0.50–1.00) compared to sedentary (reference) after multi-adjustment. Moderate/high physical activity was inversely associated with both cardiovascular disease and all-cause mortality, but became non-significant after multi-adjustment. Sedentary non-metabolic syndrome participants had lower cardiovascular disease incidence (0.47; 0.31–0.72) but not significantly different cardiovascular disease (0.61; 0.31–1.19) and all-cause mortality (0.92; 0.64–1.34) compared to sedentary metabolic syndrome participants. Both light and moderate/high physical activity were inversely associated with cardiovascular disease and all-cause mortality in non-metabolic syndrome participants (p<0.05). There were significant variations in several central cardiometabolic risk factors with physical activity level in non-metabolic syndrome participants. Fibrinogen mediated the protective effects of physical activity in non-metabolic syndrome participants.
Conclusion
Physical activity of different intensities attenuated cardiovascular risk and mortality in 60-year old men and women with metabolic syndrome during a 20-year follow-up.
Introduction
The metabolic syndrome (MetS) is a cluster of metabolic and clinical features, 1 with complex underlying mechanisms including lifestyle factors such as physical inactivity, unhealthy eating habits and stress interacting with genetic factors.2,3 The MetS is associated with increased risk for several non-communicable diseases including type 2 diabetes and cardiovascular diseases (CVDs). 4 Recent reports present an alarming increase in MetS prevalence all over the world5,6 and preventive strategies are urgently needed.
Increased physical activity (PA) reduces the cardiometabolic risk factors present in the MetS.7,8 A recent systematic review showed a negative linear relationship between leisure-time PA and MetS incidence, concluding that any amount of leisure-time PA was more beneficial than none and that individuals exceeding current PA guidelines had substantially lower MetS incidence. 9 Moreover, data from a few large population-based samples indicate that active participants with clustered CVD risk factors have similar risks of CVD and all-cause mortality to active participants without risk factors.10–13 In individuals with impaired glucose tolerance, a combined intervention of increased PA and improved eating habits reduced the risk of type 2 diabetes, CVD and total mortality after 30 years. 14 However, the aforementioned studies are mainly targeting exercise i.e. the middle-to-upper intensity level of PA, with less data available for the potential effect of light intensity PA or to what extent sedentary time increases CVD risk in MetS individuals. 15 With low fulfilment rates of recommended moderate-high intensity PA, a majority of waking hours spent sedentary16,17 and an aging population, it is relevant from both a clinical and a public health perspective to gain a deeper understanding of the roles and benefits of different intensities of PA from long-term follow-ups in robust population based samples. Moreover, the clinical definition of the MetS as an all-or-none condition may not adequately reflect individual differences in cardiometabolic risk, hence, comparative analyses in MetS and non-MetS individuals of how cardiometabolic risk factors varies with PA level would give a deeper understanding of possible mediating effects on long-term clinical outcomes.
The aim of this study was to analyse the association of leisure-time PA of different intensities at baseline, CVD incidence, CVD mortality and all-cause mortality in a large population-based sample of 60-year-old men and women both with and without established MetS, for more than 20 years of follow-up. A secondary aim was to study which cardio-metabolic factors may mediate the association between PA and long-term outcomes.
Methods
Study population
From August 1997–March 1999, every third person (n = 5460) living in Stockholm County, Sweden, born between 1 July 1937–30 June 1938, was invited to participate in a health screening survey. A total of 4232 individuals (2039 men and 2193 women, 78% response rate) agreed to participate and underwent physical examinations and laboratory tests and completed a self-administrated questionnaire. A total of 491 individuals with previously reported CVD (myocardial infarction, angina pectoris, heart failure, intermittent claudication and/or stroke) at baseline and/or missing data for the PA variable (n = 48) at baseline were excluded, leaving 3693 individuals (1727 men and 1966 women) for the present analyses. The study was approved by the ethical committee at the Karolinska Institutet, and all clinical investigations were conducted according to the Declaration of Helsinki. All study participants gave their informed oral consent to be enrolled in the study. Written consent was not collected as, at the time the study was initiated, forms for written consent were not in current use. The ethical committee has in several recent matters approved continued research on the current material, 18 referring to the fact that eligible men and women were already informed (in written form) about the study and that participation was voluntary.
Assessment of PA and other lifestyle factors
Leisure-time PA during the past year was self-reported through the question; Please report your leisure-time physical activity level during the past year. If the activity has varied between summer and winter, please tick an average during the past year, with the given alternatives: (a) Sedentary (mainly sedentary activities such as reading, television viewing, and going to the movies or walking, riding a bike or performing other light intensity activities less than 2 hours a week), (b) Light-intensity PA (walking, riding a bike or performing other activities without sweating at least 2 hours a week), (c) Regular moderate-intensity PA (exercising regularly for at least 30 min, 1–2 times a week, such as running, swimming, playing tennis, badminton or performing other activities that make you sweat), or (d) Regular high-intensity PA (running, swimming, playing tennis, badminton, doing gymnastics or performing other activities for at least 30 min, three or more times a week, at such intensity level that you sweat excessively). The question has been validated against objectively assessed accelerometer data (hip-worn Actigraph GT3X for 7 days) in 57 men and women, with a significant correlation to total PA (rs = 0.32) (data not shown).
Lifestyle-related factors in the present study were reported in the questionnaire and dichotomised; educational level (university degree or not), current smoking (yes/no), dietary intake of vegetables and fruit (high intake; one portion daily/almost daily or low intake; occasionally/never). Concerning alcohol, a weekly consumption of 4–6 bottles of strong beer, or 2–3 bottles of wine, or 0.35–0.75 l spirits was considered as a high intake. Heredity of high blood pressure, dyslipidaemia, diabetes mellitus or CVD was defined as self-reported presence of the conditions, respectively, in either the individual’s mother and/or father.
Clinical examination
Weight was assessed to the nearest 0.1 kg, and height to the nearest 0.5 cm. Waist circumference was measured in a standing position, midway between the lower rib margin and the iliac crest. An automatic device (HEM 711, Omron Healthcare, Bannockburn, Illinois, USA) measured systolic and diastolic blood twice in a seated position after 5 min of rest in a supine position. The mean of the two measurements was used. A venous blood sample was drawn from an antecubital vein after overnight fasting S-triglycerides and S-cholesterol were analysed using enzymatic methods (Bayer Diagnostics, Tarrytown, New York, USA). S-high-density lipoprotein (HDL) was measured after isolation of S-low-density lipoprotein (LDL) and S-very-low-density lipoprotein (VLDL), and S-insulin levels using the enzyme-linked immunosorbent assay (ELISA) technique (Boehringer Mannheim Gmbh, Germany). S-LDL was estimated using Friedewald’s method. S-glucose was measured with an enzymatic colorimetric test (Bayer Diagnostics, Tarrytown, New York, USA). The homeostasis model of insulin resistance (HOMA-IR) was calculated as (fasting serum glucose*fasting serum insulin/22.5). The hypertriglyceridaemic waist phenotype was defined as waist circumference of ≥90 cm (men) or ≥85 cm (women), and a triglyceride level of 2.0 mmol/l (men) or 1.5 mmol/l (women). 19 The long-chain polyunsaturated fatty acids eicosapentaenoic acid and linoleic acid were assessed as the proportions of these in serum cholesteryl esters as a valid marker of the dietary intake of these fatty acids, using methods previously described. 20
MetS
The MetS was classified according to the American Heart Association/National Heart, Lung, and Blood Institute’s criteria 1 including ≥3 of the following; fasting glucose ≥5.6 mmol/l or on drug treatment for elevated glucose, triglycerides ≥1.7 mmol/l or on drug treatment for elevated triglycerides, HDL<1.0 mmol/l (men) and <1.3 mmol/l (women) or on drug treatment for reduced HDL, systolic blood pressure ≥130 mm Hg or diastolic blood pressure ≥85 mm Hg or on antihypertensive drug treatment, or waist circumference ≥102 cm (men) and ≥88 cm (women).
CVD event and mortality surveillance
All participants were followed from the date of completion of the baseline investigation until the date of their death or until 31 December 2017. Cases of first-time CVD event (fatal or non-fatal myocardial infarction or ischaemic stroke) and death from any cause were ascertained through regular examinations of the National Cause of Death Register and the National Patient Register, using the International Classification of Diseases 10th revision codes: I21, I25, I46, I63, I64, I65 and I66. Only the main underlying cause was considered. Heart failure and haemorrhagic stroke were not included as they are not necessarily caused by atherosclerosis.
Statistics
The descriptive data is presented as proportions or median and 25th–75th percentile (Q1–Q3) with Kruskal Wallis analysis of variance (ANOVA) and Mann-Whitney U test (continuous variables) and Pearson Chi-Square (dichotomised variables) for trend and between group analyses. Sex-adjusted Cox-regression analyses studied trend and between group analyses for incidence rates of CVD, CVD morbidity and all-cause mortality. Multi-adjusted Cox regression modelling was used to assess the hazard ratio (HR) and 95% confidence interval (CI) and plot model-predicted survival curves (Figure 1) across a cross-tabulated variable of MetS (MetS or non-MetS) and PA at baseline (sedentary, light or moderate/high) for all three outcomes (with the group MetS+sedentary set as reference). The proportionality assumption was examined using scaled Schöenfeld residuals, detecting zero slopes for the scaled Schöenfeld residuals on functions of time for outcomes. Mediation analysis was performed using the structural equation modelling-based discrete-time survival mediation model. 21 We used path analysis and mediation models to examine indirect effects (ab path) of PA on CVD incidence, CVD mortality and all-cause mortality. We estimated 95% Monte Carlo CIs to determine if the mediated effects were statistically significant. A mediated effect was supported if the 95% Monte Carlo CI did not contain zero. SPSS (version 25.0) and Mplus version 8.3 were used for statistical analyses.
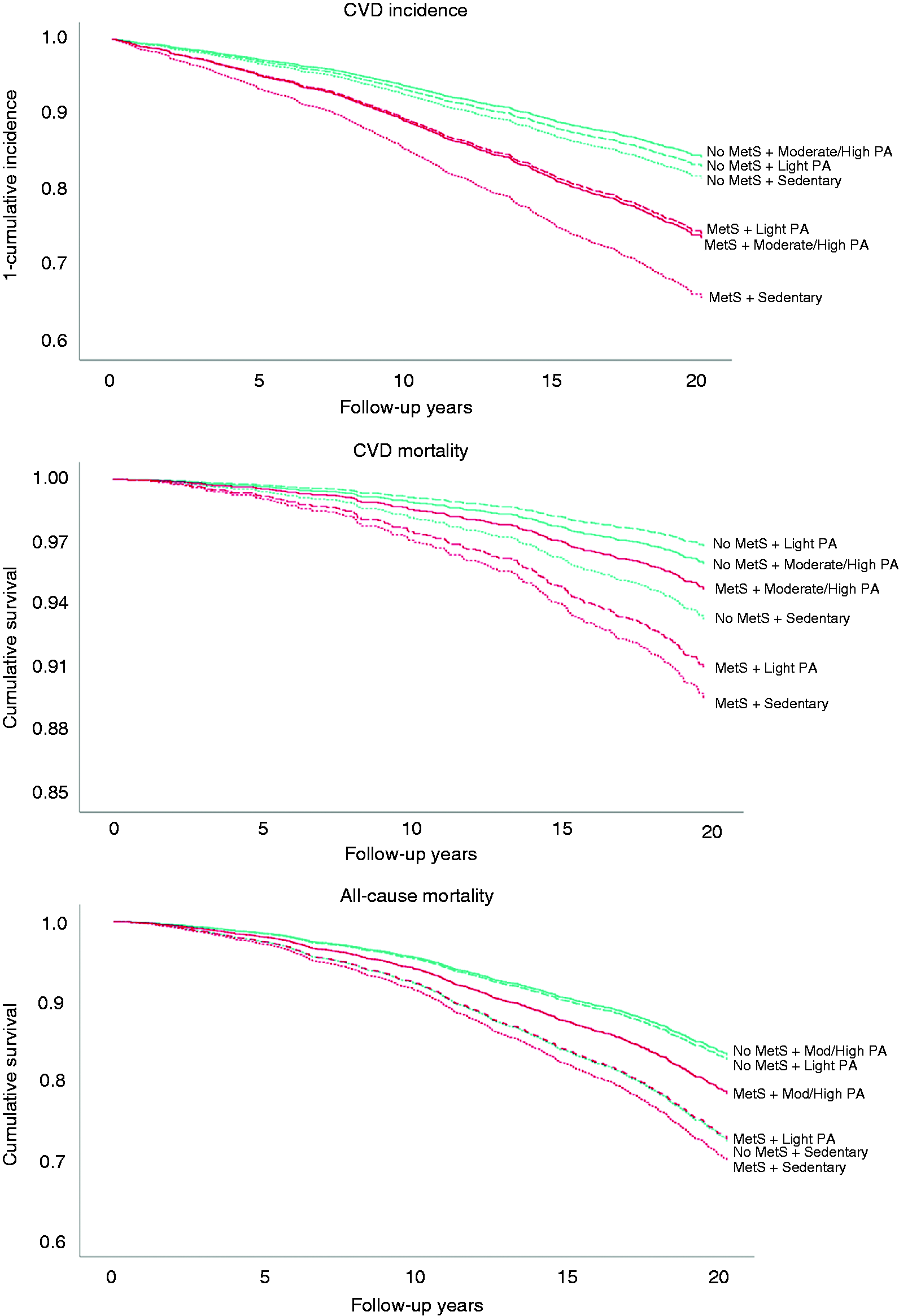
Model-predicted survival curves for cardiovascular disease (CVD) incidence, CVD mortality and all-cause mortality across the cross-tabulated variable of metabolic syndrome (MetS) prevalence and physical activity (PA) level. No MetSS = green lines; MetS = red lines. Sedentary = dotted lines; light PA = cross-hatched lines; moderate/high PA = solid lines. Adjusted for sex, educational level, smoking habits, intake of fruit and vegetables, alcohol consumption, % of linoleic acid and % of eicosapentaenoic acid of total fatty acids, and CVD heredity.
Results
The prevalence of the MetS was 23.0% in the total population, more prevalent in men (26.6%) compared to women (19.8%). During the follow-up period, 661 participants experienced a non-fatal first-time CVD event (median follow-up 19.3 years). There were 187 deaths from CVD and 756 deaths from all-causes (median follow-up 19.5 years).
MetS participants were significantly worse-off regarding most of the risk factors constituting the MetS, the other cardiometabolic variables as well as the life-style-related variables, compared to non-MetS participants in sedentary, light as well as moderate/high PA groups at baseline (Table 1). Within non-MetS participants, there were significant beneficial associations between higher PA and continuous levels of the risk factors constituting the MetS (Table 1). Similar associations were seen for the other cardiometabolic variables, including insulin, fibrinogen, gamma-glutamyl transferase, triglycerides: HDL-ratio and prevalence of the hypertriglyceridaemic waist phenotype. Within MetS participants, only non-smoking, high intake of fruit/vegetables and fibrinogen were associated with PA level.
Characteristics of the study population in relation to prevalence of the metabolic syndrome and physical activity (PA) level.
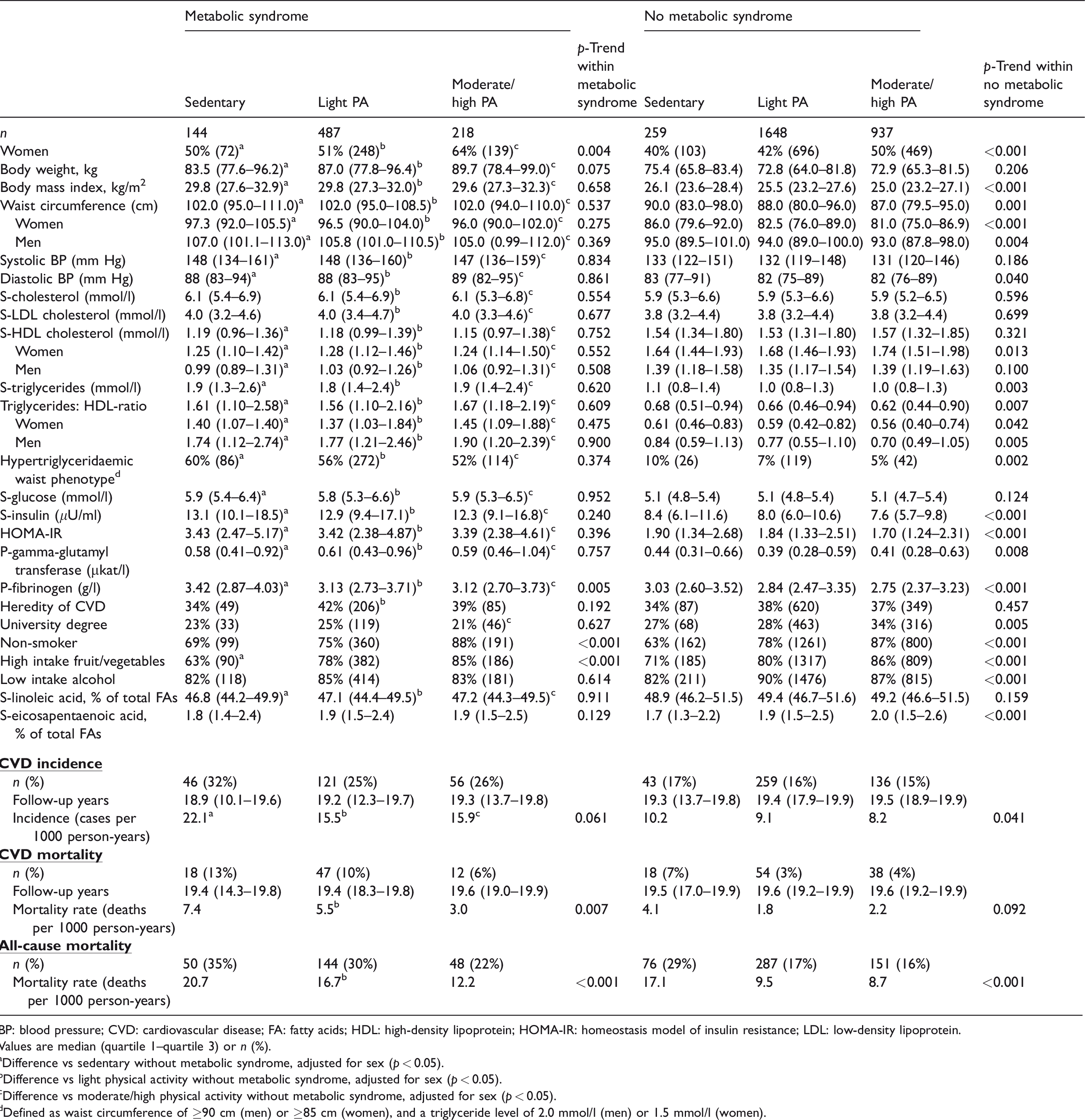
BP: blood pressure; CVD: cardiovascular disease; FA: fatty acids; HDL: high-density lipoprotein; HOMA-IR: homeostasis model of insulin resistance; LDL: low-density lipoprotein.
Values are median (quartile 1–quartile 3) or n (%).
aDifference vs sedentary without metabolic syndrome, adjusted for sex (p < 0.05).
bDifference vs light physical activity without metabolic syndrome, adjusted for sex (p < 0.05).
cDifference vs moderate/high physical activity without metabolic syndrome, adjusted for sex (p < 0.05).
dDefined as waist circumference of ≥90 cm (men) or ≥85 cm (women), and a triglyceride level of 2.0 mmol/l (men) or 1.5 mmol/l (women).
MetS, PA and CVD incidence
In MetS participants, CVD incidence was higher in those reporting sedentary leisure time at baseline, with similar CVD incidence in those reporting light and moderate/high PA at baseline (Figure 1). This corresponded to a lower risk for the light PA group compared to the reference after multi-adjustment (Table 2). Only marginal differences in risk reductions were noted between different PA levels in non-MetS participants. Similar trends were observed for both men and women.
Hazard ratio (HR) (95% confidence interval (CI)) for incident cardiovascular disease (CVD), CVD mortality and all-cause mortality in relation to physical activity (PA) level, in the total population and in men and women, respectively.
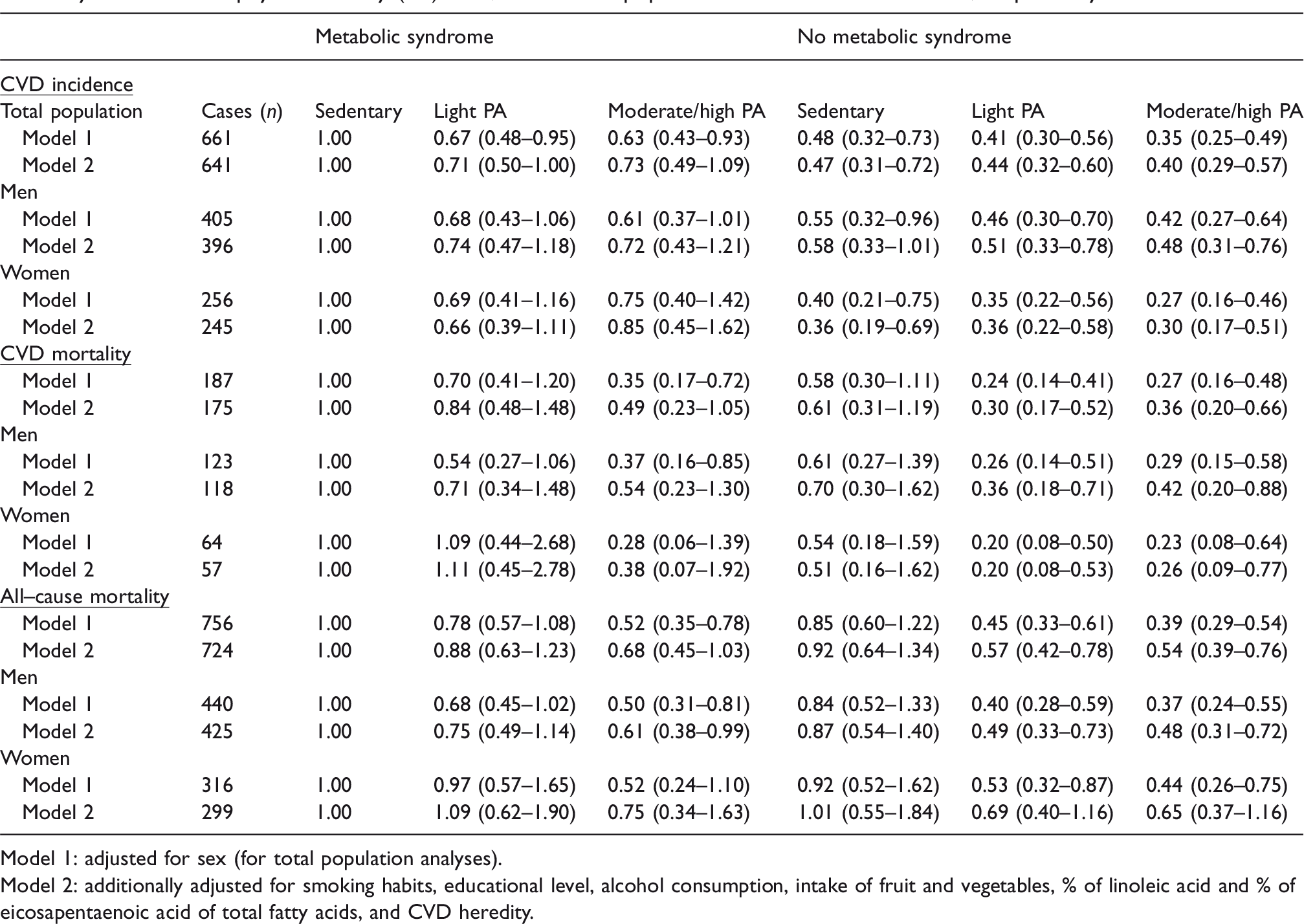
Model 1: adjusted for sex (for total population analyses).
Model 2: additionally adjusted for smoking habits, educational level, alcohol consumption, intake of fruit and vegetables, % of linoleic acid and % of eicosapentaenoic acid of total fatty acids, and CVD heredity.
MetS, PA and CVD mortality
MetS participants engaging in moderate/high PA at baseline had higher cumulative survival than non-MetS participants who were sedentary at baseline (Figure 1) as well as 65% reduced risk for CVD mortality compared to their sedentary counterparts (Table 2). However, this association became non-significant after multi-adjustment. For non-MetS participants, CVD mortality risk for men and women who were sedentary at baseline did not differ significantly from sedentary men and women with MetS. However, both light and moderate/high PA in non-MetS participants was associated with greater survival and lower risk compared to their sedentary counterparts.
MetS, PA and all-cause mortality
In MetS participants, moderate/high intensity PA attenuated the risk for all-cause mortality to similar levels as for non-MetS participants who engaged in either light or moderate/high intensity PA at baseline. Also, the cumulative survival was higher for MetS participants engaging in moderate/high intensity PA than sedentary non-MetS participants (Figure 1). All-cause mortality risk did not differ between sedentary MetS and non-MetS participants, while engaging in light or moderate/high PA decreased the risk in both groups.
In further sensitivity analysis, we excluded CVD cases and deaths occurring in the first two years of follow-up, finding only marginal changes in the effect size of the estimates and no changes of significance between the groups of the cross-tabulate variable (data not shown).
Mediation analyses
None of the indirect effects of PA on CVD incidence were statistically significant (Supplementary Material Table S1. Direct effects, univariate analyses and model description are in Supplementary Material Tables S2–S5 and Supplementary Material Figure S1). PA had a statistically significant indirect effect on CVD mortality through triglycerides in non-MetS, which yielded a 0.045-unit increase in the log odds of CVD mortality during the 20-year follow-up period.
PA had a statistically significant indirect effect on CVD and all-cause mortality via fibrinogen in non-MetS participants, and on all-cause mortality via fibrinogen in MetS participants. However, the difference in magnitude of the indirect effect between non-MetS and MetS participants for all-cause mortality was not statistically significant (p = 0.468). The mediated effects of PA on CVD mortality and all-cause mortality via fibrinogen yielded a decrease in the log odds of mortality during the 20-year follow-up period.
Discussion
In a long-term follow-up of a population-based and representative cohort of 60-year old Swedish men and women, MetS participants had a significantly higher incidence of a first-time CVD event, CVD mortality and all-cause mortality compared to non-MetS participants, but PA of different intensities attenuated the risks in both groups. Specifically, in MetS participants, light intensity PA attenuated CVD incidence risk after multi-adjustment, and moderate/high PA diminished the risk for CVD and all-cause mortality in sex-adjusted analyses, but became non-significant after multi-adjustment. Non-MetS participants had a lower risk for CVD incidence regardless of activity level (including sedentary) compared to MetS participants, but a significantly decreased risk of CVD and all-cause mortality, light or moderate/high intensity PA were needed in non-MetS. Interestingly, sedentary non-MetS participants did not have significantly lower risk for CVD mortality and all-cause mortality compared to sedentary MetS participants. Hence, today’s widespread sedentary behaviour means a risk increase for everyone.
The clinical definition of the MetS as an all-or-none condition may not adequately reflect individual differences in cardiometabolic risk. Some people may just barely meet or not meet the criteria set, whereas other may have a severe MetS. Hence, some of the underlying mechanisms explaining the effect of PA on clinical outcomes in both MetS and non-MetS individuals, may be linked to variations in the components of the MetS. In the present study, we found large variations of these variables with PA levels, especially in non-MetS participants. For example, waist circumference, diastolic blood pressure, triglycerides and HDL (in women) were significantly worse in sedentary, compared to more active, non-MetS participants. Importantly, this was also seen for insulin, fibrinogen, gamma-GT and triglycerides: HDL ratio. The hypertriglyceridaemic-waist phenotype has previously been associated with a worse cardiometabolic risk profile and an increased risk for coronary artery disease, 19 was twice as common (10% vs 5%) in sedentary compared to moderate/highly active non-MetS participants. While previous studies conclude important effects of exercise training (hence more intense PA) on potential underlying mechanisms for increased CVD risk in metabolic unhealthy individuals, 23 the findings in the present study add knowledge of the important role of light PA for these individuals. The following mediation analyses showed few, but important, significant indirect effects of PA on the outcomes. At baseline, MetS participants had generally higher fibrinogen levels. Interestingly, fibrinogen appeared to be a mediating factor in the effects of PA for future risk of CVD and all-cause mortality, especially in non-MetS participants. This is a reminder of the fact that the MetS often causes a prothrombotic condition and that factors, which is not included in the definition by the MetS, can explain the increased risk. In total, these findings reinforce the importance to consider PA level in clinical evaluations of future CVD risk and in the prevention and treatment of the MetS.
The present findings are in agreement with a few previous prospective cohort studies.10–12,24 For example, individuals with clustering of CVD risk factors have been shown to be at greater risk of incident coronary heart disease and premature cardiovascular death,10,24 however, high PA at baseline attenuated this risk and was comparable to inactive individuals without clustering of risk factors. Also, in a population-based sample of 23,747 middle-aged Scottish men and women, the CVD risk associated with poor metabolic health was substantially lower in participants being physically active, with the minimal protective threshold for mortality in participants with clustered metabolic abnormalities defined as a weekly bout of moderate-to-vigorous PA. 11 In an 11-year follow-up of 10,134 men and women aged 45–79 years, physically active participants with MetS had a lower risk of coronary artery disease than participants without MetS who were physically inactive. 24 The present study adds to the current literature with the unique features of being a representative sample of its source population (60-year-old men and women), and the extensive analyses of variation in cardiometabolic risk factors with PA level in both MetS and non-MetS.
The potential attenuating effect of even light-intensity PA on CVD incidence in MetS participants, is particularly important for older adults, as individuals in this age group, to a greater extent than younger age-groups, tend to spend a greater portion of their waking hours sedentary and to less extent achieve recommended exercise intensity levels.16,17 Furthermore, we have previously reported that left ventricular hypertrophy was twice as common (12%) in individuals with MetS compared with individuals without MetS (6%). 25 As expected, left ventricular hypertrophy was strongly linked to high blood pressure. As both left ventricular hypertrophy and high blood pressure are key determinants for future cardiac events, the present findings that light-intensity PA may attenuate some of this risk, even after adjustment for other central life-style related factors, provides an important health message.
Randomised controlled PA intervention studies in MetS individuals with future cardiovascular risk or all-cause mortality as end-points are lacking. However, there are several reports in the literature from intervention studies demonstrating that the cardiovascular risk factors clustering in the MetS can be reduced with increased PA. In women aged 45–75 years, it was demonstrated that exercise training had a positive impact of cardiometabolic risk factors as well as the prevalence of the MetS after six months. 26 From a randomised controlled study of 101 68-year-old individuals recruited from the present study cohort who were sedentary, overweight, and abdominally obese, it was demonstrated that PA on prescription reduces sedentary time and increases PA level. 27 This was accompanied by reduced body weight, waist circumference, sagittal abdominal diameter, neck circumference, as well as favourable effects on body composition, blood lipids and glucose-insulin homeostasis. Interestingly, reducing sedentary time was also closely associated to telomere elongation in the intervention group. 28 Coronary artery calcium, an independent predictor of coronary artery disease, was cross-sectionally studied among 678 middle-aged Swedes (52% women). 13 Among participants with moderate-high fitness (estimated by cycle ergometer test) the odds of having a high coronary artery calcium score was halved, compared to those with low fitness. Furthermore, MetS individuals had 47% higher odds for high coronary artery calcium score compared with those without MetS – however, moderate-high fitness seemed to partially attenuate this risk.
Strength and limitations
Strengths of the present study are the relatively large and population-based cohort of both men and women and the long-term follow-up, with a high response rate at baseline, implying that results may be translated to 60-year-old men and women in Stockholm, Sweden. The cohort was thoroughly characterised, which allow a detailed description of the participants as well as adjustments for several potential confounders in the analyses. Furthermore, it enables investigation of potential mediators between PA and long-term outcomes in MetS as well as non-MetS participants. Another strength is the high validity of Swedish national population registers, which allows us to recruit individuals from the general population as well as follow them in terms of morbidity and mortality. Limitations include self-report of PA and other lifestyle-related factors, and that the status of the participants was investigated only at baseline. Our analyses regarding mediating factors may provide a deeper insight regarding the protective effects from PA. However, such analyses must be interpreted with great caution due to many reasons. The complexity of the MetS is one and the fact that statistical relationships are obviously not the same as causal relationships is another.
Summary
In the light of a rapidly increasing prevalence of the MetS worldwide, we find that our observations regarding beneficial effects of PA at different intensity levels on CVD mortality and total mortality, in both MetS and non-MetS participants, are encouraging. The risk reductions seen already at light intensity PA level for CVD incidence in MetS participants, and for all outcomes in non-MetS participants, are highly relevant from both a clinical and public health perspective, and may be an important message to individuals resistant to engagement in more intense PA. Moreover, fibrinogen, a marker for a prothrombotic state, appears to be a mediating factor in the protective effects from PA which underlines the importance of factors not included in the clinical definition of the MetS. The promotion of PA should be more encouraged in prevention, as well as in treatment of the MetS, and be considered a cornerstone in preventive strategies in clinical practice as well as in society.
Supplemental Material
CPR916596 Supplemental Material - Supplemental material for Physical activity attenuates cardiovascular risk and mortality in men and women with and without the metabolic syndrome – a 20-year follow-up of a population-based cohort of 60-year-olds
Supplemental material, CPR916596 Supplemental Material for Physical activity attenuates cardiovascular risk and mortality in men and women with and without the metabolic syndrome – a 20-year follow-up of a population-based cohort of 60-year-olds by Elin Ekblom-Bak, Mats Halldin, Max Vikström, Andreas Stenling, Bruna Gigante, Ulf de Faire, Karin Leander and Mai-Lis Hellénius in European Journal of Preventive Cardiology
Footnotes
Author contribution
EEB, MH, BG, UdF, KL and M-LH contributed to the conception or design of the work. EEB, MH, MV, AS, BG, UdF, KL and M-LH contributed to the acquisition, analysis, or interpretation of data for the work. EEB, MH and M-LH drafted the manuscript. All authors critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgement
The authors gratefully acknowledge Merja Heinonen and all personnel engaged in the baseline investigation, as well as the register studies, which formed a basis for the long-term follow-up. The authors also wish to acknowledge all of the participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by grants from the Swedish Heart and Lung Foundation (19990395, 20030620, 20050587, 20060345, 20080612, 20090588), and King Gustaf V and Queen Victoria’s Foundation/The Swedish Order of Freemasons Grand Swedish Lodge (2011, 2012, 2013, 2014, 2015). AS was supported by an international postdoc grant from the Swedish Research Council (2017-00273).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.