
Abstract
Background
It is not clear if the European Systematic Coronary Risk Evaluation algorithm is useful for identifying prevalent subclinical atherosclerosis in a population of apparently healthy individuals. Our aim was to explore the association between the risk estimates from Systematic Coronary Risk Evaluation and prevalent subclinical atherosclerosis.
Design
The design of this study was as a cross-sectional analysis from a population-based study cohort.
Methods
From the general population, the Swedish Cardiopulmonary Bioimage Study randomly invited individuals aged 50–64 years and enrolled 13,411 participants mean age 57 (standard deviation 4.3) years; 46% males between November 2013–December 2016. Associations between Systematic Coronary Risk Evaluation risk estimates and coronary artery calcification and plaques in the carotid arteries by using imaging data from a computed tomography of the heart and ultrasonography of the carotid arteries were examined.
Results
Coronary calcification was present in 39.5% and carotid plaque in 56.0%. In men, coronary artery calcium score >0 ranged from 40.7–65.9% and presence of carotid plaques from 54.5% to 72.8% in the age group 50–54 and 60–65 years, respectively. In women, the corresponding difference was from 17.1–38.9% and from 41.0–58.4%. A doubling of Systematic Coronary Risk Evaluation was associated with an increased probability to have coronary artery calcium score >0 (odds ratio: 2.18 (95% confidence interval 2.07–2.30)) and to have >1 carotid plaques (1.67 (1.61–1.74)).
Conclusion
Systematic Coronary Risk Evaluation estimated risk is associated with prevalent subclinical atherosclerosis in two major vascular beds in a general population sample without established cardiovascular disease or diabetes mellitus. Thus, the Systematic Coronary Risk Evaluation risk chart may be of use for estimating the risk of subclinical atherosclerosis.
Introduction
The mortality from coronary artery disease is declining in developed countries, but cardiovascular disease is still a leading cause of mortality and morbidity. 1 Although there is overwhelming evidence that effective risk factor management reduces the risk of cardiovascular events, there is an urgency to improve the implementation of prevention guidelines. 2
European guidelines recommend using the Systematic Coronary Risk Evaluation (SCORE) charts to assess patients’ overall cardiovascular risk in order to guide risk factor treatment. 3 The SCORE algorithm estimates the 10-year absolute risk of a fatal cardiovascular event and is based on age, sex, smoking, systolic blood pressure and total cholesterol. An updated SCORE algorithm for Sweden was recently shown to more adequately predict the number of cardiovascular deaths compared with the previous version. 4 In addition to the 10-year absolute risk of a fatal cardiovascular event, information about the probability that an atherosclerotic disease is already present may increase the awareness of risk and thereby improve the patient’s motivation and call for specific secondary prevention measures. 5 However, it is not clear if the SCORE algorithm is useful for identifying subclinical atherosclerosis in a population of apparently healthy individuals and there are, so far, no SCORE charts indicating the risk of prevalent subclinical atherosclerosis.
We hypothesised that the SCORE algorithm can be useful also for estimating the risk of prevalent subclinical atherosclerosis in individuals without established cardiovascular disease or diabetes mellitus. Accordingly, our aim was to explore the associations between the risk estimates from the SCORE algorithm and the risk of prevalent subclinical atherosclerosis defined as presence of atherosclerosis in the coronary and carotid arteries. We also wanted to generate new SCORE charts that can be used in individual consultations. For these purposes, we used a recent large population survey in Sweden, the Swedish Cardiopulmonary Bioimage Study (SCAPIS).
Methods
SCAPIS
SCAPIS is a collaborative project between six Swedish universities, aiming to randomly invite 30,000 individuals from the general population living in six Swedish university cities (Gothenburg, Linköping, Malmö/Lund, Stockholm, Umeå and Uppsala), aged 50–64 years. The overall participation rate in SCAPIS was 50%. In addition to determining the traditional cardiovascular risk factors, the participants underwent extensive imaging, including non-contrast and contrast-enhanced computed tomography (CT) coronary angiography; CT scanning of the abdomen for the quantification of visceral and subcutaneous adipose tissue, liver fat; and ultrasound analysis for carotid artery atherosclerosis. 6 The study was approved by the Umeå Ethical Review Board (# 2010-228-31 M), and all participants provided written informed consent.
Study population
Of the 15,810 participants enrolled in the SCAPIS cohort between November 2013–December 2016, 13,411 participants were included in the analysis after excluding participants with; prevalent cardiovascular disease or diabetes mellitus and missing data (n = 1578 and 821, respectively) (Figure 1). In addition to assessing the traditional cardiovascular risk factors, we recorded data from a computed tomography scan of the heart and ultrasonography of the carotid arteries. We analysed coronary artery calcium score as present or absent coronary calcification and presence of plaques in any of the carotid arteries.
Flow chart. CVD: cardiovascular disease; SCORE: Systematic Coronary Risk Evaluation.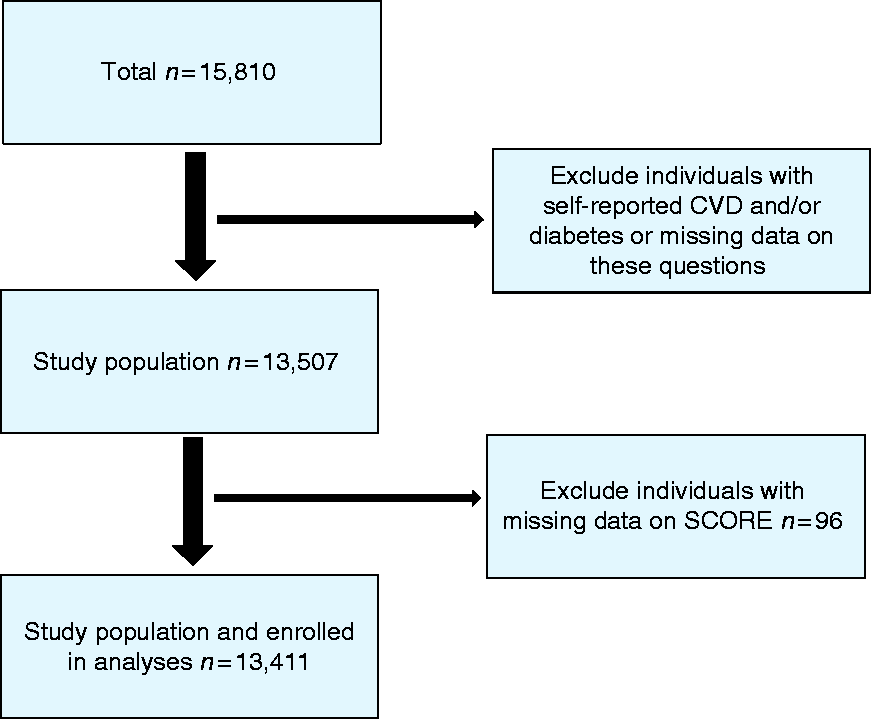
SCORE
The 2015 SCORE Sweden Risk Chart was used 4 to calculate a score for each participant. This requires data on sex, age, smoking, systolic blood pressure and total cholesterol. Current smoking status was collected from a questionnaire. Systolic blood pressure was measured in the supine position twice in each arm with an automatic device (Omron M10-IT. Omron Health Care Co., Kyoto, Japan) using the mean systolic blood pressure from the arm with the highest mean. Total cholesterol was analysed at the respective university hospital laboratory using a venous blood sample collected after an overnight fast. Based on the calculated SCORE, and presence of certain single risk factors (see below), each participant was assigned to one of four risk groups (low risk <1%, moderate risk 1–4%, high risk 5–9% or very high risk ≥ 10%).
Coronary artery calcification
Coronary artery calcification was assessed in non-contrast enhanced images from a state-of-the-art multi-slice computed tomography scanner (Siemens, Somatom Definition Flash, Siemens Healthineers, Erlangen, Germany). Imaging and analyses were performed using a calcium scoring protocol and the calcium content in each coronary artery was measured and summed to produce a total coronary artery calcification score (CACS) according to international standards.7,8 An Agatston score > 0 was defined as having coronary artery calcification.
Carotid artery plaque
Atherosclerosis in the carotid arteries was determined by using a standardized protocol with a Siemens Acuson S2000 ultrasound scanner equipped with a 9L4 linear transducer (both from Siemens Healthineers, Erlangen, Germany). The left and right carotid artery were insonated and atherosclerotic plaques in the common carotid artery, bulb or in the internal carotid artery fulfilling the Mannheim consensus 9 were identified. Accordingly, plaques were defined as focal structures encroaching into the arterial lumen of at least 0.5 mm or 50% of the surrounding Intima media thickness(IMT) value, or demonstrates a thickness > 1.5 mm as measured from the intima-lumen interface to the media-adventitia interface. Visually detected plaques in the carotid arteries, were summed as a number of total plaques value. Significant carotid atherosclerosis was defined by >1 plaque in the carotid arteries.
Statistics
The study population was described with total number and percentage, mean and 95% confidence interval (CI) or median and interquartile range (IQR). Chi-square, analysis of variance (ANOVA) and the Kruskal-Wallis test were used for analysing group differences.
As noted by others, the SCORE distribution is highly positively skewed in middle-aged population cohorts. CACS is commonly analysed as a categorical variable due to its known skewed distribution with a large proportion of zeros. A similar skewed distribution was noted for carotid plaque burden in this population, also with an excessive number of zeros. To meet the assumption of a linear relationship between the log odds and SCORE we used the log2 transformation of SCORE to investigate the association between SCORE and CACS and between SCORE and plaque burden using both logistic and nominal regression analyses. CACS was for the logistic regression analysis categorised into CACS < 100 vs CACS ≥ 100, while four categories commonly used in clinical praxis, were applied in the nominal regression model; 0, 1–99, 100–399, and ≥400. Carotid plaque burden was dichotomised into having no significant carotid atherosclerosis (≤1 plaque) vs having significant carotid atherosclerosis (>1 plaques) in at least one side of the carotid arteries for the logistic regression analysis, and into three categories for the nominal regression analysis; ≤1 plaque, >1 plaques in one of the carotid arteries, and >1 plaques in both sides of the carotid arteries. The C statistic was calculated for the logistic regression models.
Zero-inflated negative binominal regression technique has previously been suggested for analysing CACS, as it compensates for the excessive numbers of zeros in the dependent variable. 10 The model consists of two separate models. One model, a logit model, predicted whether an individual has a zero value or not. The second model, a negative binominal model predicted the value for participants who are not certain zeros. Finally, the two models were combined. In these models, CACS and also plaque burden were used as continuous variables and SCORE was used without transformation. Results of the zero-inflated models are given as Supplementary Material data. The results from the analyses are presented with odds ratios and 95% CIs.
Risk charts, corresponding to the SCORE chart, were generated for the probability of having CACS ≥ 100 and >1 plaques in at least one side of the carotid arteries, respectively. A logistic regression model was applied to estimate the probabilities based on sex, age, smoking, total cholesterol and systolic blood pressure and separate models for women and men were applied.
SPSS version 24 and R version 3.2.0 were used to perform the analyses.
Results
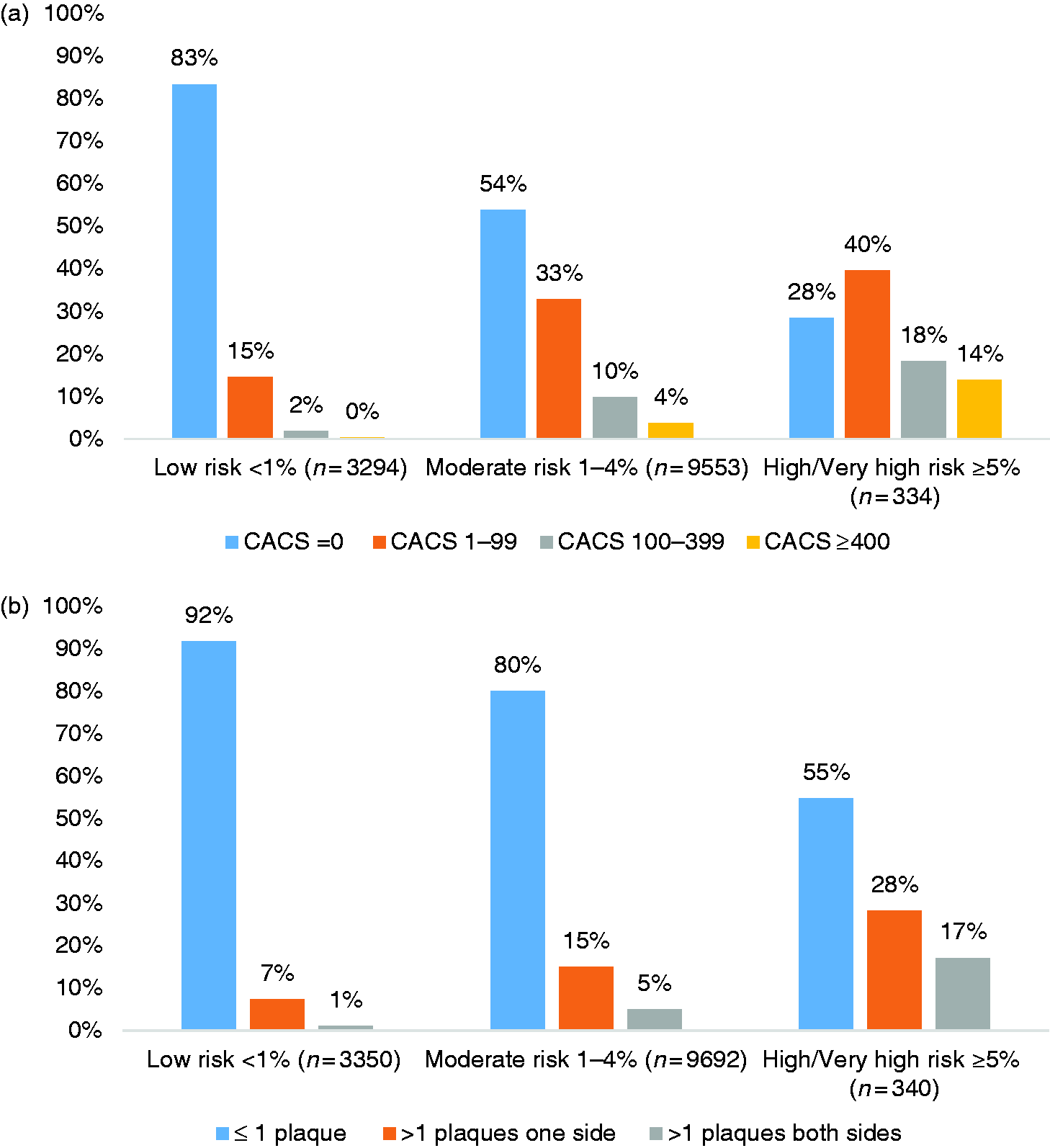
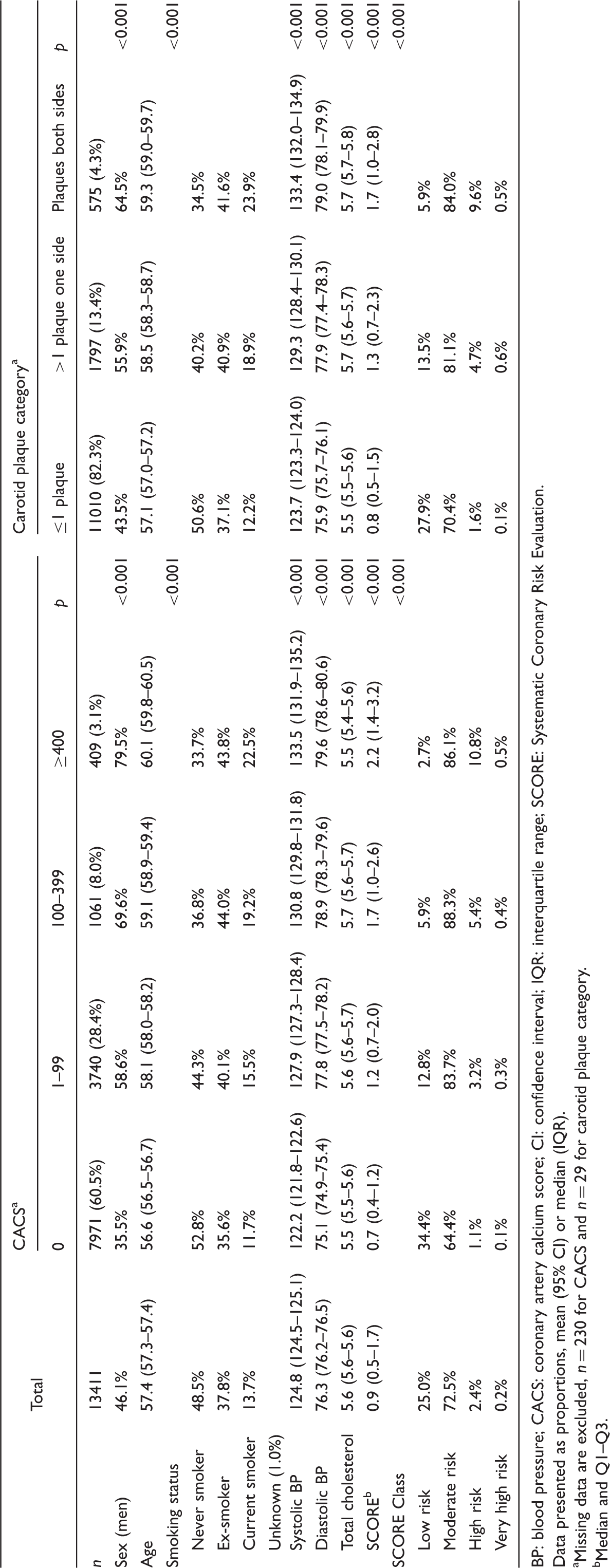
Coronary calcification was present in 39.5% and plaques in any of the carotid arteries in 56.0% of the participants. Baseline characteristics in different categories of CACS and plaque burden in the carotid arteries are shown in Table 1. The distribution of CACS > 0 and CACS ≥ 100 and atherosclerosis in the carotid arteries in relation to sex and age is shown in Figure 2(a)–(d) and in different SCORE categories is further illustrated in Figure 3(a) and (b), respectively.
Prevalence of coronary artery calcium score (CACS) > 0 (n = 5210), CACS ≥ 100 (n = 1470), plaque in any carotid artery (n = 7498) and >1 plaques in any carotid artery (n = 2372) by age and sex. (a) Systematic Coronary Risk Evaluation (SCORE) in three risk category groups by four groups of coronary artery calcium score (CACS). (b) SCORE in three category groups by three groups of carotid plaque. Overview of baseline characteristics in different categories of subclinical atherosclerosis. The Swedish Cardiopulmonary Bioimage Study (SCAPIS), 2013–2016. BP: blood pressure; CACS: coronary artery calcium score; CI: confidence interval; IQR: interquartile range; SCORE: Systematic Coronary Risk Evaluation. Data presented as proportions, mean (95% CI) or median (IQR). Missing data are excluded, n = 230 for CACS and n = 29 for carotid plaque category. Median and Q1–Q3.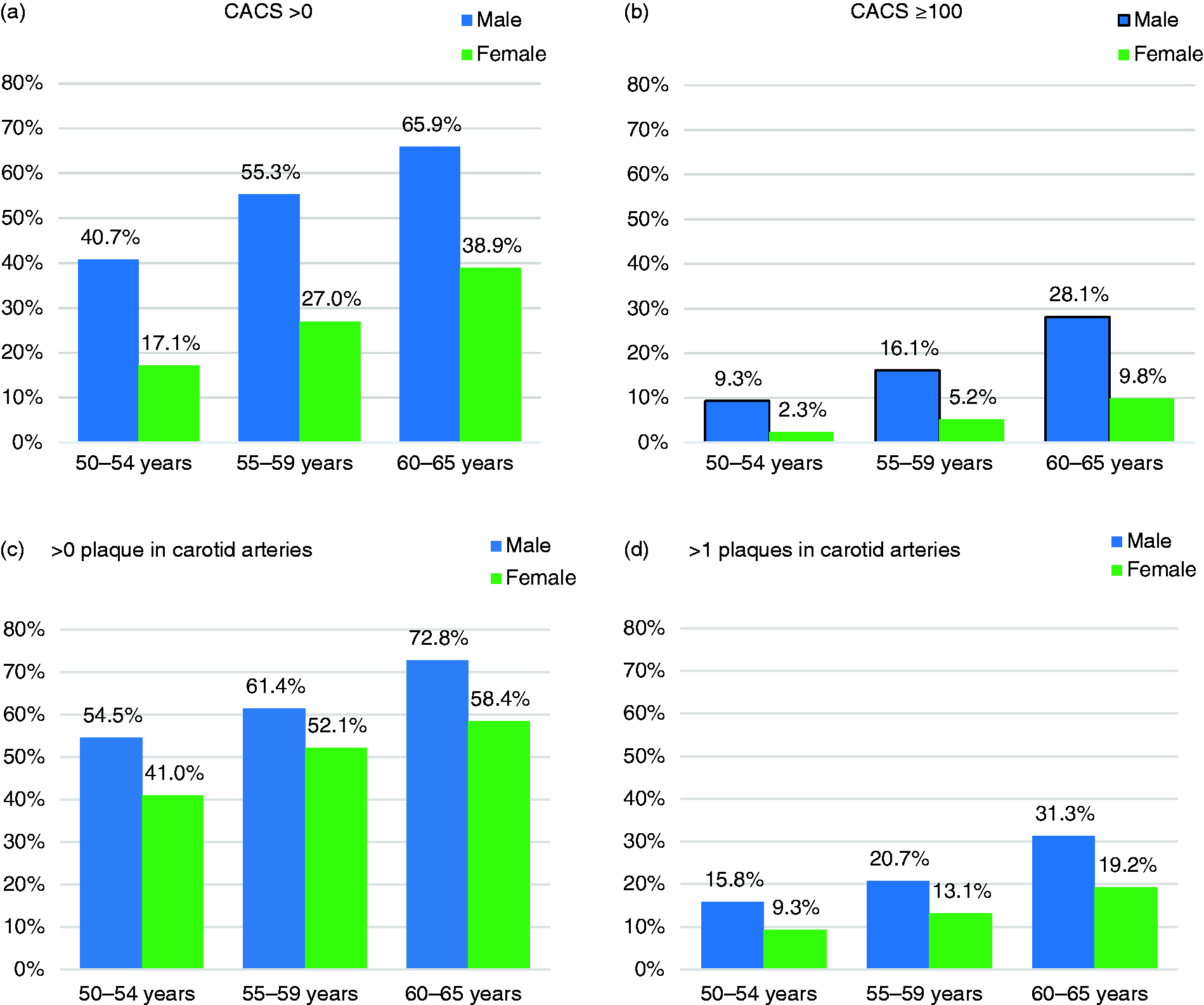
SCORE related to CACS
In a logistic model, a doubling of SCORE was associated with an increased probability to have CACS > 0 as compared to CACS = 0, odds ratio (OR) 2.18 (95% CI, 2.07–2.30), Wald χ2(1) = 850, p < 0.001, C statistic 0.75 (95% CI, 0.74–0.76). In an ordinal model, a doubling of SCORE was associated with an increased probability of being in a higher CACS category, OR 2.04 (95% CI, 1.97–2.10), Wald χ2(1) = 1840, p < 0.001. There was a higher proportion of antihypertensive or/and lipid lowering agent users with increasing CACS (Supplementary Material, Table S1). Sensitivity analysis showed that the association between a doubling of SCORE and the probability to have CACS > 0 as compared to CACS = 0 remained basically unchanged after excluding participants on antihypertensive (n = 2420) or/and lipid lowering (n = 941) agents, OR 2.17 (95% CI, 2.04–2.31), Wald χ2(1) = 595, p < 0.001. The zero-inflated models confirmed the association between SCORE and CACS (Supplementary Material). Data on sensitivity, specificity, positive and negative predictive values for different SCORE-levels are given as Supplementary Material Table S2(a) and (b). A SCORE < 1 could exclude CACS ≥ 100 with a negative predictive value of 98% and a SCORE ≥ 5 could detect CACS ≥ 100 with a positive predictive value of 32%.
SCORE related to plaque in the carotid arteries
In a logistic model, a doubling of SCORE was associated with an increased probability to have >1 plaques in any of the carotid arteries, OR 1.67 (95% CI, 1.61–1.74), Wald χ2(1) = 647, p < 0.001. In an ordinal model, a doubling of SCORE was associated with an increased probability of being in a higher carotid plaque category, OR 1.69 (95% CI, 1.63–1.76), Wald χ2(1) = 683, p < 0.001, C statistic 0.67 (95% CI, 0.66–0.68). There was a higher proportion of antihypertensive or/and lipid lowering agent users with increasing carotid plaques (Supplementary Material Table S1). In a sensitive analysis, where participants who reported using antihypertensive or/and lipid lowering agents were excluded, a doubling of SCORE was still associated with OR 1.66 (95% CI, 1.58–1.74), Wald χ2(1) = 475, p < 0.001 for having>1 plaques in any of the carotid arteries. The zero-inflated models confirmed the association between SCORE and carotid plaques (Supplementary Material). Data on sensitivity, specificity, positive and negative predictive value for different SCORE-levels are given as Supplementary Material Table S2(a) and (b). A SCORE < 1 could exclude more than one carotid plaque with a negative predictive value of 92% and a SCORE ≥ 5 could detect more than one carotid plaque with a positive predictive value of 45%.
Prevalence of atherosclerosis in coronary and carotid arteries
The prevalence of subclinical atherosclerosis in coronary and carotid arteries is graphically illustrated in Figure 4(a)–(d) showing the estimated prevalence of CACS ≥ 100 and>1 plaques in carotid arteries, respectively, stratified for; sex, age, systolic blood pressure, total cholesterol and smoking. The SCORE risk charts were useful to identify patients from low to a very high risk of having atherosclerosis.
(a) Estimated proportion (%) of men with coronary artery calcium score (CACS) ≥ 100 stratified by age, blood pressure (BP), cholesterol and smoking. (b) Estimated proportion (%) of women with CACS ≥ 100 stratified by age, BP, cholesterol and smoking. (c) Estimated proportion (%) of men with >1 carotid plaque in any carotid artery stratified by age, BP, cholesterol and smoking. (d) Estimated proportion (%) of women with >1 carotid plaque in any carotid artery stratified by age, BP, cholesterol and smoking.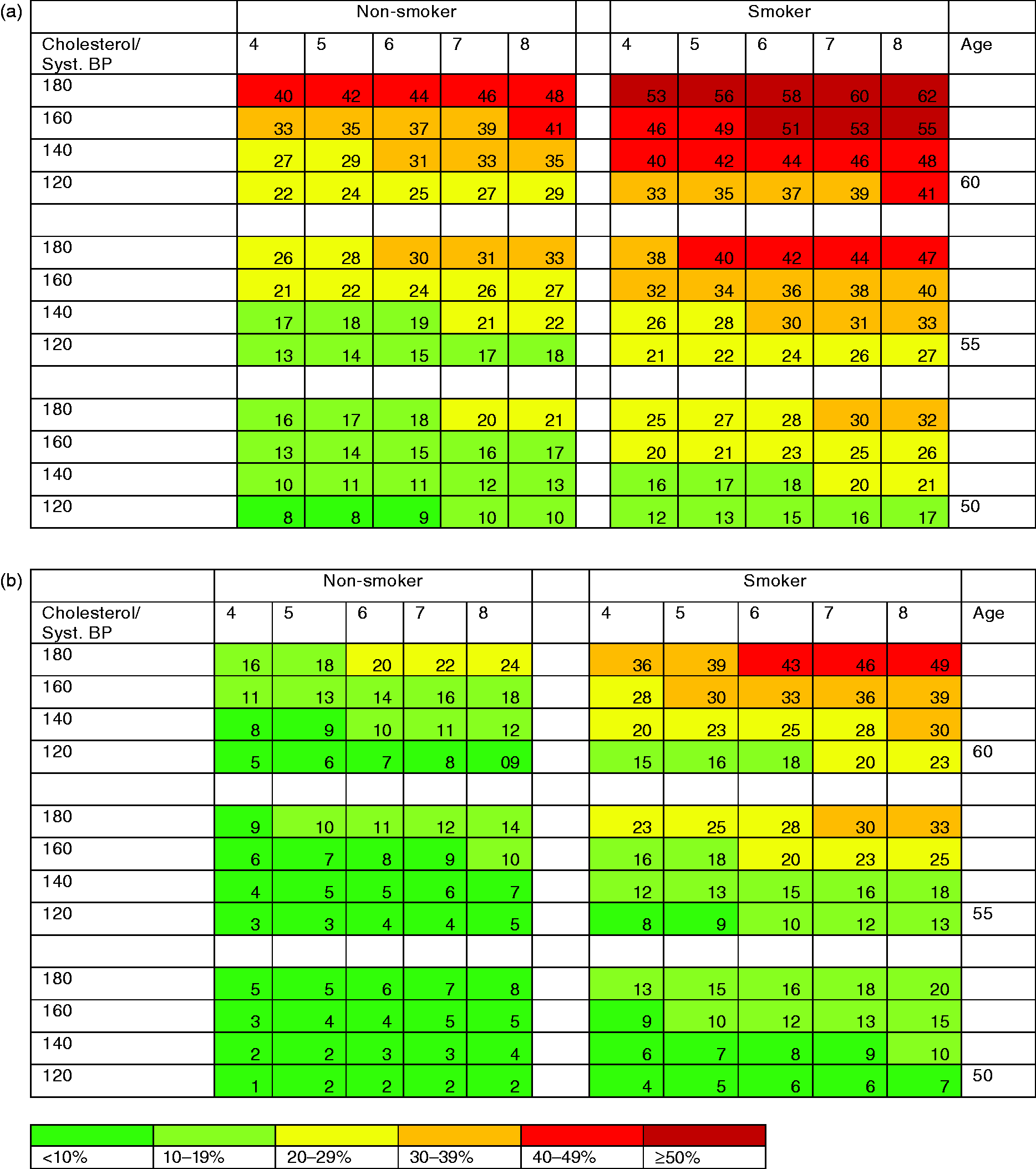
Discussion
This is the first analysis from the SCAPIS, which is so far the largest study in which a random sample from the general population has been examined for presence of both coronary artery calcification and carotid plaques. In the present analysis, including 13,411 participants, SCORE estimated risk was strongly associated with prevalent subclinical atherosclerosis in two major vascular beds in a general population sample without established cardiovascular disease or diabetes mellitus. The analysis also shows that the SCORE risk charts were able to stratify individuals from those with low risk to those with very high risk of having subclinical atherosclerosis. A SCORE < 1 indicated a low risk of significant coronary or carotid artery disease, with a negative predictive value of 92–98%, whereas a SCORE ≥ 5 indicated a high risk, with a positive predictive value of 32–45%.
Strengths and limitations of this study
The major strength of the present population-based study is the sample size of more than 13,000 randomly selected individuals examined according to a common, standardised and detailed protocol. Still, the study confers a risk of selection bias, and because of the observational nature we cannot determine causality. Regarding potential selection bias we know from the pilot study that low socio-economic status was associated with lower participation rate. 11 Furthermore, we observed an association between living in a low-socioeconomic status area and elevated coronary artery calcification. 12 However, this bias would most likely confer an underestimation of the relationship between SCORE and subclinical atherosclerosis in our study. CACS was used as a marker of subclinical atherosclerosis in the coronary arteries and is recommend by clinical guidelines in Europe 3 in selected asymptomatic individuals. Calcification is associated with the extent of total coronary plaque burden13,14 but coronary artery calcification is not an indicator of the (in)stability of an atherosclerotic plaque 15 and absence of calcification does not exclude presence of non-calcified plaques, which may be a limitation. If the non-calcified plaques could also have been identified (increasing the pre-test likelihood), this would have resulted in higher positive predictive values. Finally, the study included participants in one country who were mainly from European origin. Thus, our findings may not be generalisable to other populations.
Comparison with other studies
The association between future risk for cardiovascular disease and CACS has already been well established.16,17 Our findings are in accordance with a smaller study published in 2011 from the Multi-Ethnic Study of Atherosclerosis (MESA) showing a strong association between the estimated 10-year Framingham Risk Score and CACS in 5660 individuals between 45–84 years of age. 18 For each increase of 5% in the 10-year risk for coronary heart disease events using the Framingham Risk Score, the odds of having a positive CACS nearly doubled. 19 Also, in the Progression of Early Subclinical Atherosclerosis (PESA) study, including 4066 bank employees between 40–54 years of age, the prevalence of subclinical atherosclerosis was higher in those with higher Framingham 10-year risk score. 20 In that study, 58% of those at low risk according to SCORE had signs of subclinical atherosclerosis defined as CACS > 0, or plaques detected in the carotids, abdominal aorta or iliofemoral territories, compared with 90% in those with at least a moderate risk. In our study, the majority of subjects were in the moderate SCORE risk group. Interestingly, a previous study in the field on a predominantly low-risk group without cardiovascular disease found that current decision thresholds using SCORE had a very low sensitivity, especially in women, to detect increased vascular ageing. 21 We have used visually detected plaques in the carotid arteries according to the Mannheim consensus 9 as a measure of carotid atherosclerosis in this study. However, other studies in the field have used total plaque area in mm2. 22
The novelty of our study is that it explores the association between SCORE and subclinical vascular disease by measuring both coronary artery calcification and atherosclerotic plaques in the carotid arteries in a large random contemporary sample of the general population. In this aspect, the results from our study fill a gap of knowledge. The age distribution pattern, illustrated in Figure 2(a)–(d), of prevalent subclinical atherosclerosis is overall similar in carotid and coronary arteries, however, with differences between men and women. The degree of association between coronary and carotid atherosclerosis remains an unsolved issue that remains to be scrutinised in future publications.
Clinical implications
Most guidelines recommend a mixture of opportunistic and systematic screening.3,23 In Europe, the SCORE charts are recommended in apparently healthy people and not for those with established cardiovascular disease or at high risk for other reasons such as type 2 diabetes or chronic kidney disease. In many countries, the general practitioners have a unique role in identifying individuals at risk but without established cardiovascular disease and assessing their eligibility for preventive intervention that may include lifestyle changes and pharmaceutical treatment.
What is the clinical relevance of knowing whether an individual has a high probability of having subclinical atherosclerosis? Firstly, most cardiovascular risk factor management guidelines do not advocate the use of coronary or carotid imaging to detect subclinical atherosclerosis for treatment decisions. However, the finding that a doubling of SCORE was associated with a doubling of the odds for having significant subclinical calcification in the coronary arteries and almost a doubling of the odds for having carotid plaques is easy to remember as a rule of thumb applicable in clinical practice. Secondly, and maybe more importantly, the final decision regarding preventive treatment is made by the physician together with the patient, where the patient’s perception of risk is important. This was recently illustrated in a randomised clinical trial where ultrasound-based pictorial information targeting both primary care physicians and individuals, reduced the cardiovascular disease risk factor burden after one year. 24 Accordingly, the perception of the link between the patient’s modifiable risk factors, such as smoking, lipids and blood pressure and subclinical atherosclerosis may be enhanced by using the charts illustrated in Figure 4(a)–(d) and, thus, may be helpful to motivate the patient to adhere to lifestyle changes and pharmaceutical treatment. Thirdly, future studies may demonstrate detection of subclinical atherosclerosis by imaging to be beneficial in primary prevention. This will increase the importance of identifying individuals who will have a high probability of a positive imaging test result.
Conclusions
In summary, subclinical atherosclerosis in the coronary and carotid arteries was highly prevalent in this middle-aged cohort without established cardiovascular disease or diabetes mellitus. The SCORE estimated risk proved, beyond predicting the 10-year absolute risk of a fatal atherosclerotic event, to also be a potentially clinically useful tool for evaluating the risk for having prevalent subclinical atherosclerosis. The risk charts visualising the link between patient’s modifiable risk factors and the risk of having subclinical atherosclerosis may also be relevant to motivate the patient to adhere to suggested lifestyle changes and pharmaceutical treatment.
Supplemental Material
CPR909300 Supplemental Material - Supplemental material for Systematic Coronary Risk Evaluation estimated risk and prevalent subclinical atherosclerosis in coronary and carotid arteries: A population-based cohort analysis from the Swedish Cardiopulmonary Bioimage Study
Supplemental material, CPR909300 Supplemental Material for Systematic Coronary Risk Evaluation estimated risk and prevalent subclinical atherosclerosis in coronary and carotid arteries: A population-based cohort analysis from the Swedish Cardiopulmonary Bioimage Study by Carl J Östgren, Stefan Söderberg, Karin Festin, Oskar Angerås, Göran Bergström, Anders Blomberg, John Brandberg, Kerstin Cederlund, Mats Eliasson, Gunnar Engström, David Erlinge, Erika Fagman, Emil Hagström, Lars Lind, Maria Mannila, Ulf Nilsson, Jonas Oldgren, Ellen Ostenfeld, Anders Persson, Jonas Persson, Margaretha Persson, Annika Rosengren, Johan Sundström, Eva Swahn, Jan E Engvall and Tomas Jernberg in European Journal of Preventive Cardiology
Footnotes
Acknowledgements
Editorial support was provided by Ebba Bergman, Uppsala Clinical Research Center, Sweden. The analyses were previously presented as a poster at the American Heart Association Annual Congress in Chicago November 10-12, 2018.
Author contribution
CJÖ, TJ, OA, KC, ME, EF, EH, MM, UN, EO, AP, JP, ES, KF, SS, GB, AB, JB GE, DE, LL, JO, MP, AR, JS and JEE contributed to the to the conception, design and data interpretation of the work. CJÖ, TJ, OA, KC, ME, EF, EH, MM, UN, EO, AP, JP, ES and KF contributed to the acquisition or analysis of data for the work. CJÖ and TJ drafted the manuscript. All revised the manuscript, gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the International committee of medical journal editors(ICMJE) uniform disclosure form and declare no support from any organisation of the submitted work apart from the support from research financiers stated below that supported the conduct of the SCAPIS study and individual research support from the government and A Rosengren’s support from AFA Insurance as stated below. Outside the submitted work, E Hagström reports having received grants and personal fees from Sanofi, Amgen; S Söderberg reports being an advisory board member and receiving received speakers’ honoraria from Actelion, Bayer, MSD; J Sundström reports being an advisory board member for Itrim. All other authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The main funding body of SCAPIS is the Swedish Heart-Lung Foundation (2019-0012). The study is also funded by the Knut and Alice Wallenberg Foundation (2014-0047), the Swedish Research Council (822-2013-2000) and VINNOVA (Sweden’s Innovation agency) (2012-04476), the University of Gothenburg and Sahlgrenska University Hospital, Karolinska Institutet and Karolinska University Hospital, Linköping University and University Hospital, Lund University and Skåne University Hospital, Umeå University and University Hospital, Uppsala University and University Hospital. The main funder, the Swedish Heart-Lung Foundation, supported the study by providing project management support throughout the study, however the final decision has always been made by the national steering committee (represented by the six responsible universities and university hospitals that conducted the study). None of the funding parts have been involved in the data analysis or data interpretation and the decision to submit is solemnly up to the authors. Individual research support: from the Swedish state under the agreement between Swedish government and the county councils, the ALF-agreement (ALF-GBG-718851 to G Bergström, O Angerås, J Brandberg, E Fagman, A Rosengren), (ALF-VLL-548791 for S Söderberg) and (ALF-LIO-700841 for JE Engvall). A Rosengren has also received research grant from AFA Insurance (160334) for the submitted work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.