
Abstract
Aims
The aim of this study was to investigate the relation between body mass index (BMI) in young women, using weight early in pregnancy as a proxy for pre-pregnancy weight, and risk for early cardiovascular disease (CVD) and mortality.
Methods and results
In this prospective, registry-based study, we used weight data in early pregnancy from women, registered in the Swedish Medical Birth Registry, and who gave birth between 1982 and 2014 (n = 1,495,499; median age 28.3 years). Of the women, 118,212 (7.9%) were obese (BMI ≥ 30 kg/m2) and 29,630 (2.0%) severely obese (BMI ≥ 35 kg/m2). After a follow-up of median 16.3 years, we identified 3295 and 4375 cases of acute myocardial infarction (AMI) and ischemic stroke (IS) corresponding to 13.4 and 17.8 per 100,000 observation years, respectively, occurring at mean ages of 49.8 and 47.3 years. Compared to women with a BMI 20–<22.5 kg/m2, the hazard ratio (HR) of AMI increased with higher BMI from 1.40 (95% confidence interval (CI) 1.27–1.54) among women with BMI 22.5–<25.0 kg/m2 to 4.71 (95% CI 3.88–5.72) among women with severe obesity, with similar findings for IS and CVD death, after adjustment for age, pregnancy year, parity and comorbidities at baseline. Women with BMI 30–<35.0 and ≥35 kg/m2 had increased all-cause mortality with adjusted HR 1.53 (95% CI 1.43–1.63) and 1.83 (95% CI 1.63–2.05), respectively.
Conclusion
A significant increase in the risk for early AMI, IS and CVD death was noticeable in overweight young women, with a marked increase in obese women.
Introduction
Overweight, obesity and severe obesity rates have increased markedly in recent decades, 1 particularly in the young. 2 The prevalence of overweight in young Swedish women is now approaching 40%, and 10% are obese, 3 with an unprecedented proportion currently being severely obese as defined by having a body mass index (BMI) ≥ 35 kg/m2. Of all adult women in Sweden, almost 6% were estimated to be severely obese in 2014, close to the global average of 5%. 1 A high BMI is associated with several adverse cardiovascular and metabolic effects, more so among younger persons.4,5 Of the many studies conducted in this area, most have been conducted in middle-aged and older persons,6–8 with only a few studies having quantified the risk for early cardiovascular disease (CVD) and all-cause and CVD-related mortality in younger individuals,9–13 and none powered to reliably investigate the effect of severe obesity in young women. In young men, a strong relationship between BMI and early CVD exists, with a noticeable increase related to BMI in the normal range, and markedly elevated rates among the severely obese. 14 So far, very little data on the effect of severe obesity in young women on early CVD are available.
Young women compared to young men are protected from coronary heart disease (CHD) 15 and also have a lower risk of stroke – both conditions are rare in the young and middle-aged. With the current increase in overweight, obesity and severe obesity in young women leading to an unprecedented number of these categories at a young age, the purpose of this paper was to quantify the potential consequences of overweight and obesity – in particular, severe obesity – on the development of early CVD, CVD mortality and all-cause mortality in women.
Methods
Study population
We used the Swedish Medical Birth Registry (MBR) to identify all women aged 18 to 45 years who gave birth to their first child between 1982 and 2014 in Sweden. The MBR includes data on all births in Sweden from 1973 and onward (with the exception of 1990 and 1991, when no data were collected) with a coverage of 99%.
16
Weight at the first antenatal visit has been registered in the MBR since 1982, while self-reported height has been recorded from 1992. Data on height between 1982 and 1992 was obtained from records kept by the midwife at the delivery. Valid information on height and weight was recorded in approximately 80% and 70% of cases, respectively. Between 1982 and 1989, early pregnancy weight was only recorded using two digits (e.g. weight ≥ 100 kg was recorded as 99 kg) and was, therefore, estimated by subtracting gestational weight gain from weight at delivery.
16
A visual inspection of annual body weight deciles showed a larger than expected increase in body weight between 1989 and 1992. Because of this increase, the weights from 1982 to 1989 were adjusted by estimating annual weight increase within deciles from 1992 to 2003, which generated a nearly linear result.
17
Women aged 18–45 years were included in the study at the date of their first antenatal visit at 6–12 weeks of gestation (90% of pregnant women). To ensure a sufficient number of outcomes, women with incomplete data at first registration (e.g. height not registered before 1982) were allowed to be included up until their fourth registration. Of the 1,507,529 women included in this study, 345 were excluded because their reported height was <140 cm or >200 cm; 10,609 were excluded because of parity >4; and 1076 were excluded because of AMI or stroke registered prior to their index pregnancy (Figure 1). The Regional Ethics Review Board in Gothenburg approved the study.
Flow chart of study population according to exclusion criteria. The flow diagram illustrates the number and reasons for exclusion.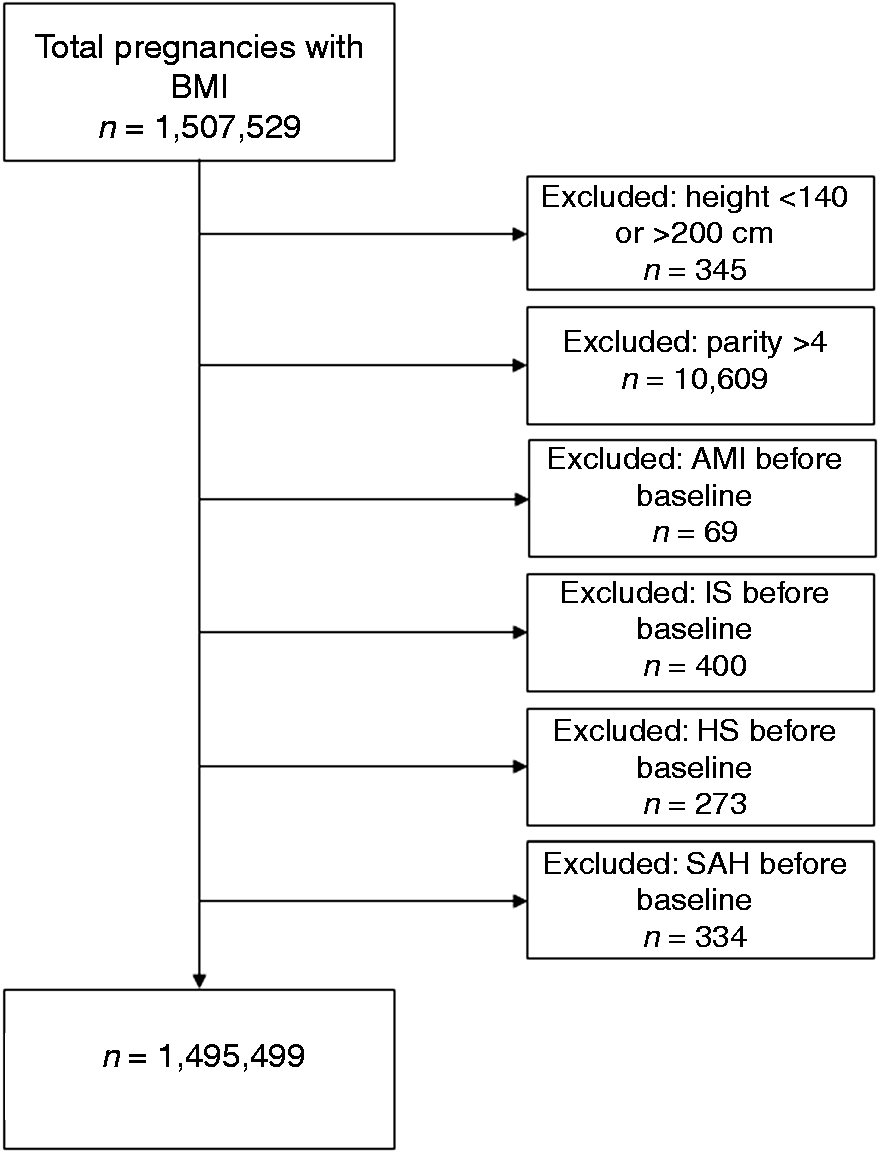
Exposure variables and covariate data
BMI was estimated by dividing body weight in kilograms by the square of height in meters (kg/m2). We subdivided the normal group (BMI 18.5– < 25 kg/m2) into three categories: lean (18.5– < 20 kg/m2, low–normal (20.0– < 22.5 kg/m2) and high–normal (22.5– < 25.0 kg/m2); the overweight group into (25.0– < 27.5 kg/m2 and 27.5– < 30 kg/m2); and the obese group into (30.0– < 35 kg/m2) and BMI ≥ 35 kg/m2, with the latter category defined as severe obesity.
We used the MBR to obtain information on age, weight, height, parity status, diabetes and smoking status from their first antenatal visit. The data were linked to the Swedish National Patient Register (NPR), through the Swedish personal identification number, to obtain data on baseline comorbidities.18,19 The individuals’ educational levels were obtained from the longitudinal integration database for health insurance and labor market studies. Education was classified as low (≤9 years), middle (10–12 years) and high (>12 years).
Diabetes and hypertension prevalence were combined from MBR (self-reported) and from NPR. Missing information in MBR for diabetes and hypertension was considered as non-diabetic and normotensive. Smoking was self-reported.
Outcomes and definitions
Sweden has a universal healthcare that provides low-cost outpatient and hospital care to all citizens. Main and contributory diagnoses are registered in the NPR according to the International Classification of Diseases (ICD; ICD-8 used until 1986, ICD-9 1987–1996, ICD-10 from 1997). This register and data from the National Cause of Death Register was used to obtain information on outcomes to define acute myocardial infarction (AMI), ischemic stroke (IS), death from CVD and from any cause (Supplementary Table 1).20,21 We defined young women as age below 45 years. The women in the study were followed from the date of their first antenatal visit until the first diagnosis of AMI, IS, death or until the end of the study, December 31, 2014 (whichever occurred first).
Statistical analysis
Baseline characteristics of the study population by body mass index (n = 1,495,499).
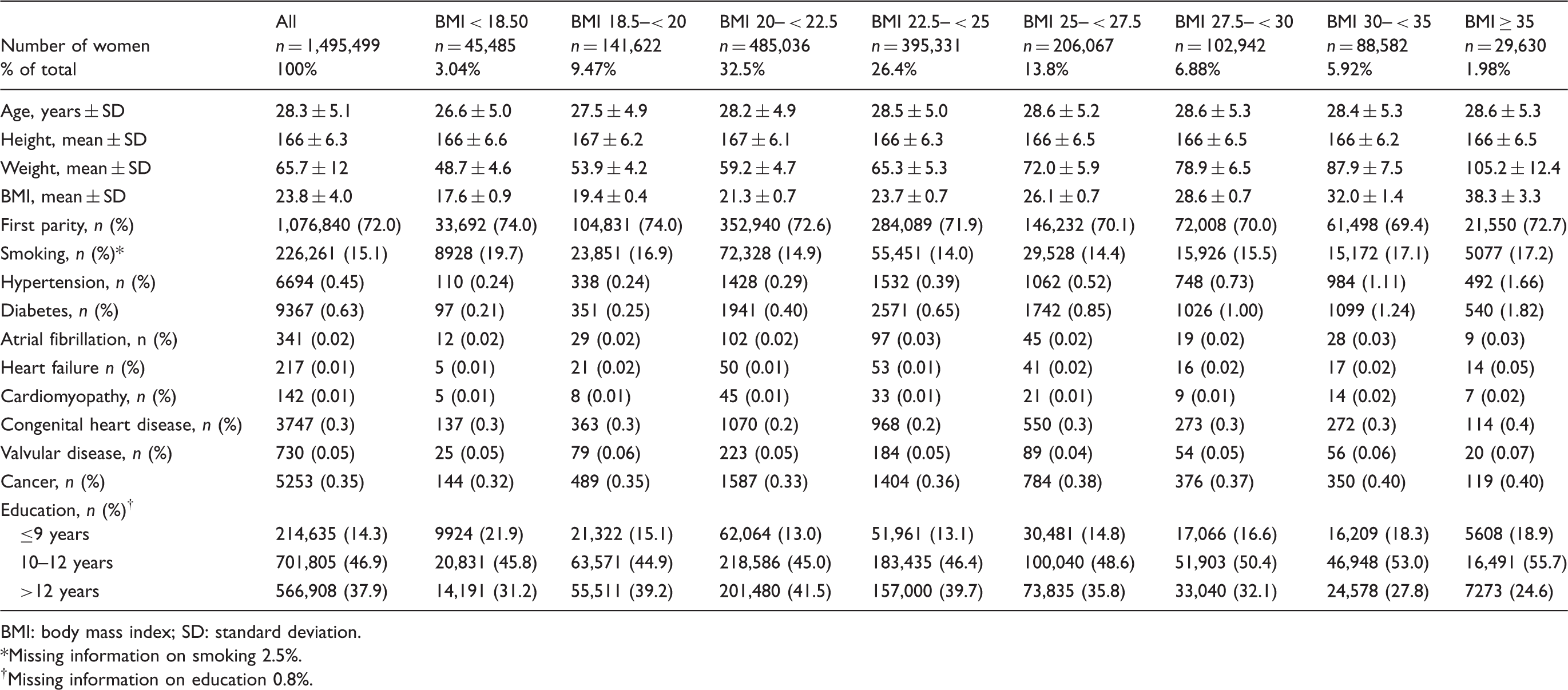
BMI: body mass index; SD: standard deviation.
Missing information on smoking 2.5%.
†Missing information on education 0.8%.
As a complement, two additional analyses were performed. Cox proportional hazards regression models where BMI was included as cubic spline with four knots placed at 5%, 35%, 65% and 95% of the observations (approximately BMI 19.0, 21.8, 24.2 and 31.6) were constructed. The incidence rates were calculated as the ratio of the number of events and the follow-up time in person-years.
Results
In total 1,495,499 women were identified from the MBR, with a mean age of 28.3 (standard deviation (SD) ± 5.1) years and a median follow-up of 16.3 years (interquartile range (IQR) 7.7–23.5). The baseline characteristics of the study population are shown in Table 1. The mean BMI was 23.8 kg/m2, 68.3% had a normal weight (BMI 18.5– < 25.0 kg/m2), while 20.6% were overweight (BMI 25.0– < 30.0 kg/m2), 5.9% were moderately obese (BMI 30– < 35 kg/m2) and 2.0% were severely obese (BMI ≥ 35 kg/m2). A total of 72.0% (n = 1,076,840) were pregnant with their first child. Diabetes mellitus and hypertension at baseline increased with increasing body weight, although the absolute levels stayed low (<2%), even among the obese. In addition, other comorbidities, such as congestive heart failure, cardiomyopathy and atrial fibrillation, although rare, also increased with higher BMI. A total of 226,261 women were smokers (15.1%), with a slightly U-formed relationship between smoking and body weight. Altogether, 37.9% had an education >12 years, higher in normal weight women and lower among the obese and severely obese.
Age at first incidence of acute myocardial infarction, ischemic stroke, hemorrhagic stroke, subarachnoid hemorrhage, cardiovascular mortality and any-cause mortality by body mass index (n = 1,495,499).
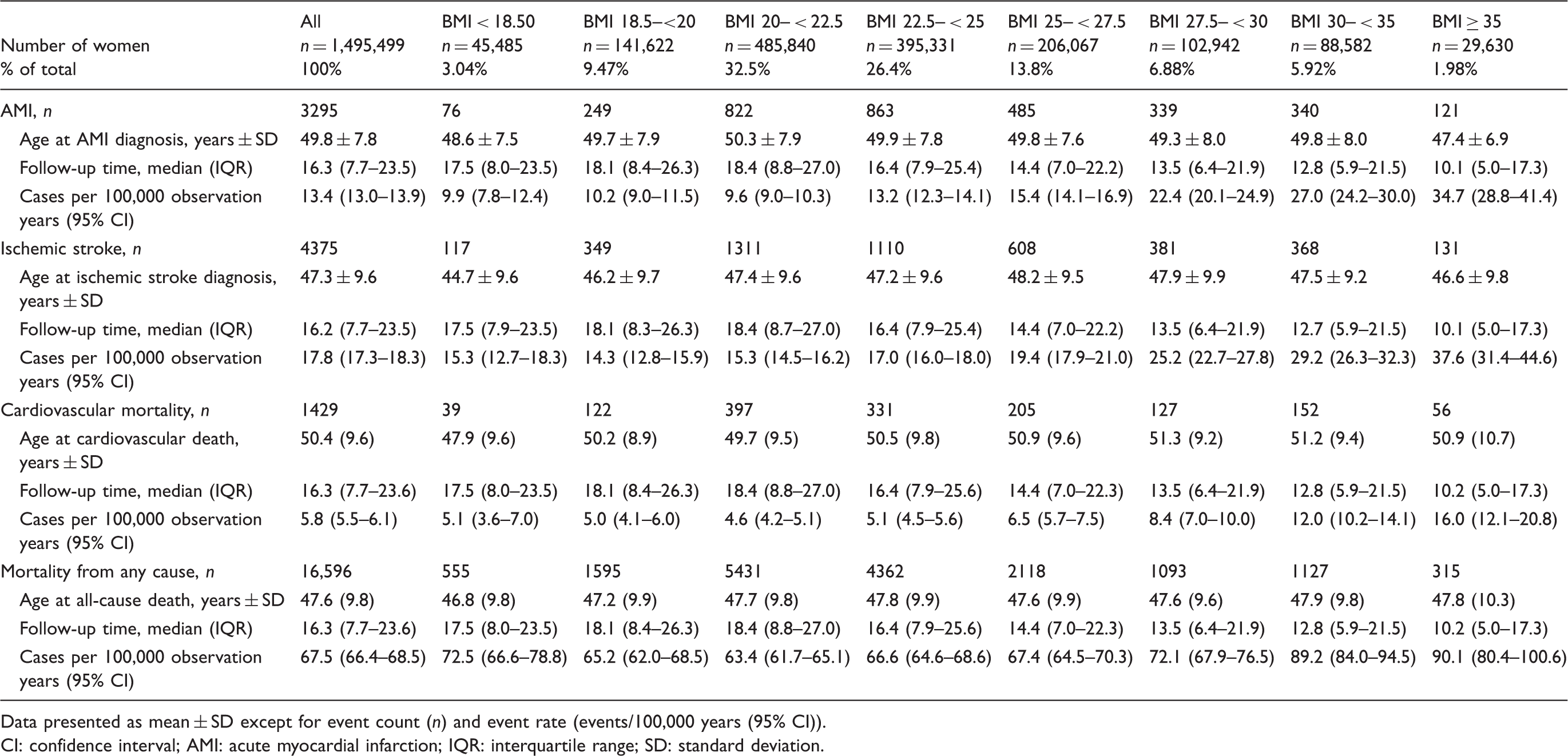
Data presented as mean ± SD except for event count (n) and event rate (events/100,000 years (95% CI)).
CI: confidence interval; AMI: acute myocardial infarction; IQR: interquartile range; SD: standard deviation.
Using a low–normal BMI of 20– < 22.5 kg/m2 as a reference, we found an increased risk for AMI already at high–normal BMI levels (BMI 22.5– < 25 kg/m2); HR of 1.40 (95% CI 1.27–1.54) after adjustment for age, pregnancy year, parity and comorbidities at baseline (Model 2), thereafter increasing gradually to HRs of 2.93 (95% CI 2.58–3.33) and 4.71 (95% CI 3.88–5.72) for women with obesity and severe obesity, respectively (Figure 2). Figure 2 shows a J-shaped association for IS, with a similarly adjusted HR of 2.92 (95% CI 2.43–3.50) in women with severe obesity, compared to the reference group.
Hazard ratios for acute myocardial infarction and ischemic stroke according to body mass index (BMI) groups (reference: BMI 20– < 22.5 kg/m2). α Model 3 is plotted in the figure. β separate analysis for a linear model above BMI 22.5 kg/m2.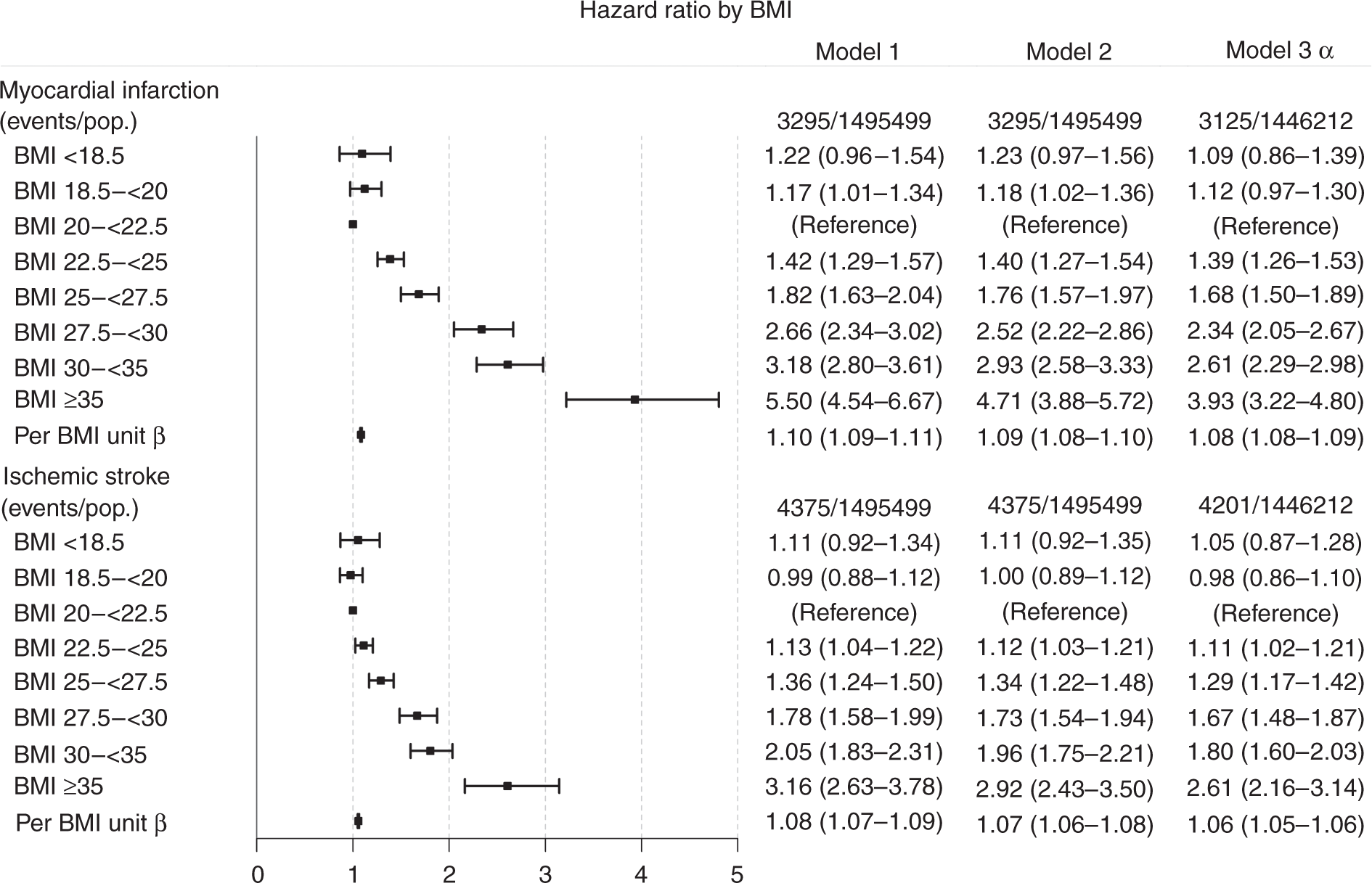
The adjusted HR for cardiovascular death increased markedly with rising BMI, and was 3.72 (95% CI 2.80–4.95) in women with severe obesity (Model 2). Furthermore, a moderately increased risk for death from any cause was observed in women with obesity and severe obesity (HR 1.53, 95% CI 1.43–1.63; and HR 1.83, 95% CI 1.63–2.05, respectively, after adjustment). Death from CVD and from any cause increased with rising BMI, with the highest rates in obese and severely obese women (Figure 3).
Hazard ratios for cardiovascular and any-cause death according to body mass index (BMI) groups (reference: BMI 20– < 22.5 kg/m2). α Model 3 is plotted in the figure. β separate analysis for a linear model above BMI 22.5 kg/m2.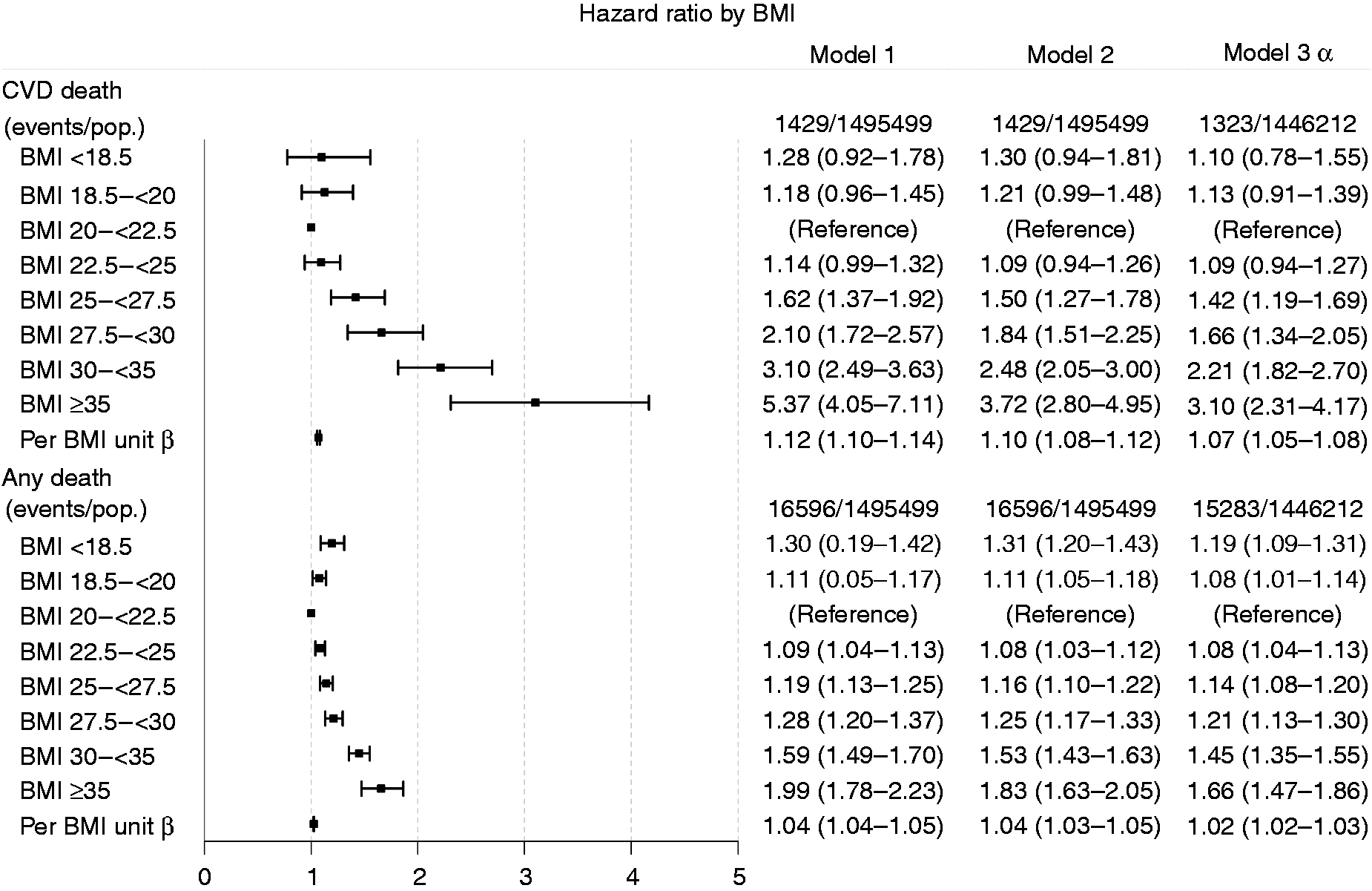
The risk of CVD and death increased exponentially by BMI groups when we also adjusted for smoking status and educational level, in addition to prior adjustments (age, pregnancy year, parity status and comorbidities at registration), Model 3. In women with BMI ≥ 35 kg/m2, the risk was 4.00 times higher (95% CI 3.30–4.86) to develop AMI, and 2.65 times higher (95% CI 2.21–3.18) to develop IS compared to women with reference BMI (20– < 22.5 kg/m2).
Figure 4 shows marginally J-shaped associations between the BMI at the time of registration for all outcomes with near-linear increases in unadjusted HR for AMI, IS and CVD death with higher BMI and less markedly so for mortality.
Association between body mass index (BMI) at registration and the risk of cardiovascular diseases and death of the study population. Adjusted for age, pregnancy year, parity and comorbidities.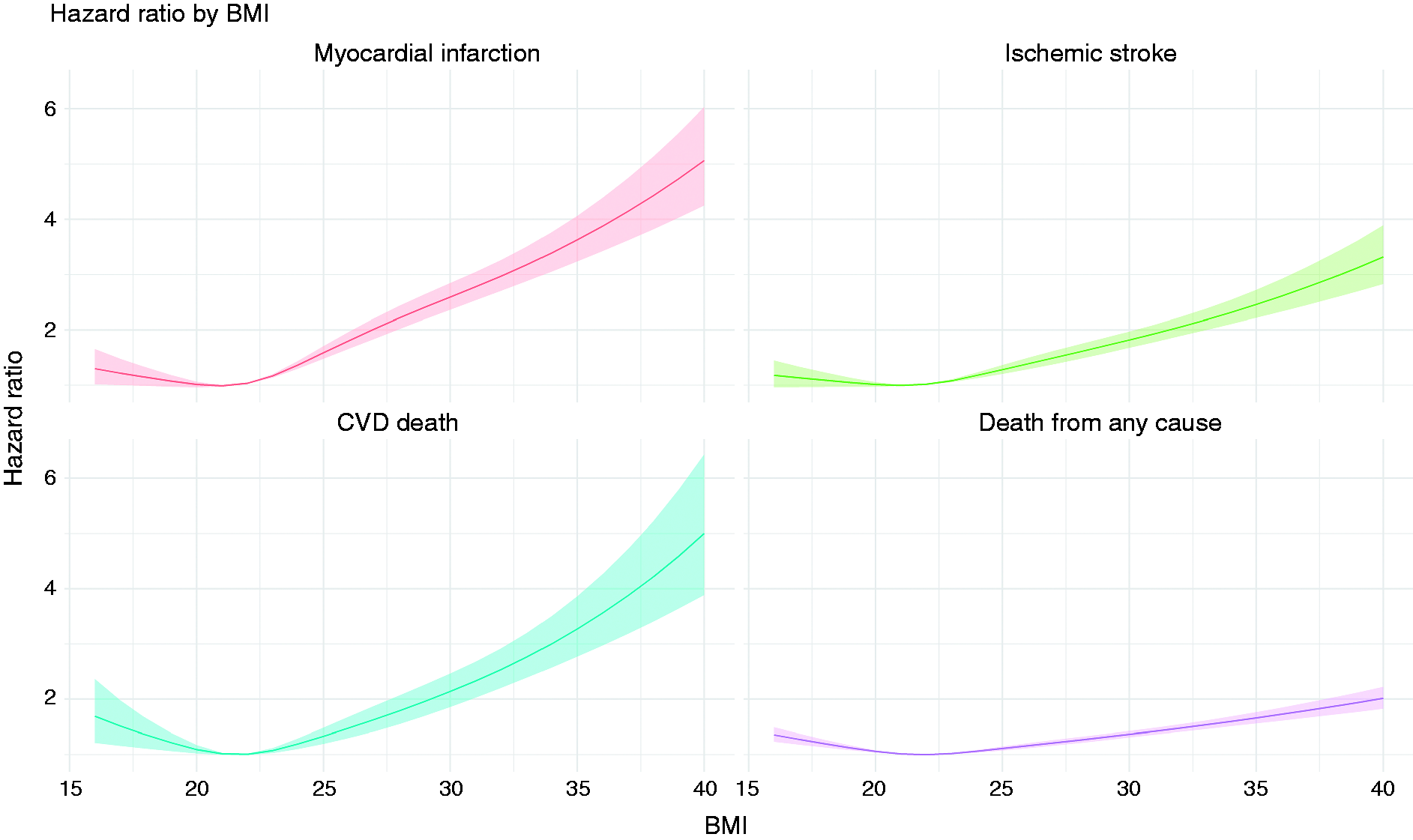
Discussion
In this large, nationwide, registry-based prospective cohort study of young women, we found slightly J-shaped relations between increasing BMI and several CVD outcomes, and that women with low–normal BMI at about 22 kg/m2 had the lowest risk, with a detectable increase in risk already within the normal weight range (22.5– < 25 kg/m2) for AMI, IS and CVD death, and markedly increased relative risks among the obese women. The highest HR for AMI was found in severely obese women, where, after adjustment for relevant baseline factors, the risk was four times higher than in women from the reference BMI group.
Previous studies have found an association of varying strength between obesity and risk for AMI in both men and women.8,23,24 Most of these studies were conducted in middle-aged populations, or with limited power in the obese and no separate analysis in the very obese subgroups.9,10 Of studies in the young, childhood obesity has been associated with the development of cardiovascular risk factors; Ortiz-Pinto et al. studied the risk of high blood pressure in children with excess weight and found that children who were obese at the age of four had an increased risk for high blood pressure at age six. 25 However, generally, young women are at very low risk of future AMI, requiring large populations with data on height and weight, in order to provide reliable risk estimates. The risk estimates for AMI in the present study are considerably higher than in older populations, likely reflecting the increasing importance of weight with younger age for the development of CVD reported in men and women aged 40 or older, 4 and are highly relevant in an era with increasingly large groups of young women with severe obesity.
Similarly, the risk for IS increased in women with overweight, with an almost doubled risk in women with BMI ≥ 30 kg/m2 and an almost threefold increase among women with severe obesity, compared to lean women. The association between overweight and obesity and an increased risk for stroke has been reported by several studies, although not in women specifically in this age group. 26 A recent Danish study has shown that overweight and obesity during childhood is associated with increased risk for early IS in both men and women aged < 55 years, 27 and an increase in risk of IS has similarly been observed in men in late adolescence. 28 A recent meta-analysis of 44 cohort studies with over 100,000 cases of stroke found a non-linear, slightly J-shaped association, with a moderate increase in risk at very high BMI levels. 29 The Nurses’ Health study of largely middle-aged women 30 found increased BMI to be an important risk factor for IS.
Lee et al. studied 18,873 women pregnant in 1950 to 1976, with a median follow-up of 50 years, and found an adjusted relative risk for CVD in overweight and obese women with HRs of 1.17 and 1.30, respectively, in comparison with a broad category of normal weight women, which was considerably lower than in the present study. 10 However, there were only 82 events in the obese category, and, further, data collected many decades ago may not be relevant to younger women of today. A Danish study evaluated the risk for AMI and stroke in young women with overweight and obesity and showed that the risk was almost two times higher compared with normal-weight women within a follow-up period of 4.5 years (IQR 2.8–5.8 years), 9 but they used a broader reference weight category, whereas we, due to our larger population, were able to identify increased risk for both outcomes within the normal weight category, and, furthermore, a markedly increased risk among the currently growing group of very obese women.
In a previous study from the MBR, we found that increased body weight in younger women was strongly associated with the risk of early heart failure, with an almost fivefold higher risk among obese women. 31 In that study, which relied on hospitalizations for heart failure as an outcome, we were unable to distinguish between heart failure with reduced as opposed to preserved ejection fraction. A recent study on older women (≥60 years) with overweight and obesity found a very strong association between obesity and heart failure with preserved ejection fraction. 32 It is likely that the effect of obesity on the myocardium is even stronger than that on the atherosclerotic process involved in AMI and IS.
We found that the mortality in young women increased with rising BMI and the highest absolute and relative risk in obese women. Our results are in accordance with previous studies that showed a significantly increased risk for early mortality from being obese in women,33,34 but with numerically higher relative risk estimates, probably due to the young age of our population.
Of the outcomes in the present study, most were of atherosclerotic origin. The association between obesity and atherosclerosis is multifactorial. Mechanisms such as hemodynamic and metabolic factors, as well as an association between inflammation and oxidative stress, have been implicated in the development of CVD in individuals with obesity. 35 Regardless, the marked effects that we found have implications for preventive measures against the development of overweight and obesity from a young age.
The present study has several strengths, such as the very large population, which is needed for studying CVD outcomes, which are infrequent in young women, and the almost complete follow-up with a maximum follow-up period of 33 years. However, there are also several limitations. A first limitation is the lack of information on subsequent BMI level during follow-up; therefore, we were unable to account for changes in BMI. But perhaps more importantly, we lack data on previous BMI measures. Therefore, it is possible that our findings also reflect the cumulative burden of weight or BMI since childhood. Furthermore, we were not able to adjust for intervening risk factors, such as preeclampsia, diabetes or hypertension, which are also linked to obesity, and, as such, on the causal pathway between obesity and CVD. Nor were there any information on hormonal treatment, which might influence body weight. Also, information on BMI closer to a CVD event may be more crucial than BMI at baseline. Even so, it is more likely that tracking of overweight and obesity into middle age will be a causal link with respect to later development of risk factors. In addition, as only women subsequently giving birth were included in our study, they may not be representative of all women in general, but, even so, only about 15% of Swedish women never give birth.
In conclusion, we found that, compared to lean young women, severely obese had a markedly increased risk of early CVD, and that women even with only moderately elevated BMI also had a significantly increased risk for CVD, CVD death and death from any cause. This strong association between high BMI in young women and early CVD raises health concerns, because of increasing numbers of young women who are obese or very obese.
Supplemental Material
CPR908983 Supplemental Material - Supplemental material for Obesity, overweight and risk for cardiovascular disease and mortality in young women
Supplemental material, CPR908983 Supplemental Material for Obesity, overweight and risk for cardiovascular disease and mortality in young women by Pigi Dikaiou, Lena Björck, Martin Adiels, Christina E Lundberg, Zacharias Mandalenakis, Karin Manhem and Annika Rosengren in European Journal of Preventive Cardiology
Footnotes
Author contribution
PD, AR and LB conceived and designed the research; PD drafted the manuscript; MA performed statistical analysis; AR, LB and KM handled funding and supervision; AR acquired the data; AR, LB, KM, CEL and ZM critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by grants from the Swedish state under the Agreement Concerning Research and Education of Doctors (ALFGBG-427301), the Swedish Heart and Lung Foundation (2015-0438, 2017-0244 and 2018-0513), the Swedish Research Council (2013-5187 (SIMSAM), 2013-4236) and the Swedish Council for Health, Working Life and Welfare (FORTE; 2013-0325).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.