
Abstract

The evidence on the inverse and independent association between regular physical activity and arterial thrombotic disease (atherosclerotic cardiovascular disease (CVD)) as well as mortality is very well established.1–3 Venous thromboembolism (VTE) (comprising deep-vein thrombosis (DVT) and pulmonary embolism (PE)) is closely related to arterial thrombotic disease via shared risk factors (such as obesity and cigarette smoking) 4 and pathophysiological mechanisms (such as coagulation, platelet activation and dyslipidaemia). 5 Just like arterial thrombotic disease, VTE constitutes a substantial public health burden and it is a preventable condition. 6 Until recently, there was diverging evidence on the link between physical activity and the risk of VTE. 7 Based on a pooled analysis of 14 prospective cohort studies, we have demonstrated that regular physical activity may also be associated with reduced risk of VTE. 8 There is, however, limited evidence on the role of specific physical activity types on the risk of VTE; knowledge of this relationship could provide insight into whether a particular physical activity type provides more or less benefits compared to others. Cross-country skiing, a seasonal high-intensity physical activity, is recognized as one of the most demanding aerobic activities and can be undertaken as a leisure-time physical activity or long-term endurance sport. The emerging evidence suggests that just like other physical activity types, cross-country skiing either undertaken as a leisure-time or competitive activity is associated with reduced risk of atherosclerotic vascular disease.9,10 Given the overall evidence and the link between physical activity, atherosclerotic CVD and VTE, we hypothesized that a relationship might exist between cross-country skiing and the risk of VTE. To our knowledge, no study has previously investigated the link between cross-country skiing and VTE. In this context, using a large general population-based sample of middle-aged Finnish men with no history of VTE at baseline, we sought to assess the prospective associations of leisure-time cross-country skiing habits with the risk of VTE.
We utilized participants (males aged 42–61 years at baseline) of the Kuopio Ischemic Heart Disease Risk Factor (KIHD) study for the present analysis. The KIHD is an ongoing prospective population-based cohort study, which was designed to evaluate emerging risk factors for vascular disease and other chronic disease outcomes. The study recruitment methods, physical examinations and measurements, and blood sample procedures and measurements of blood markers, have all been previously described in detail. 11 All baseline examinations and measurements were performed between March 20, 1984 and December 5, 1989. A 12-month physical activity questionnaire modified from the Minnesota Leisure-Time Physical Activity Questionnaire11,12 was used to assess leisure-time cross-country skiing habits (volume and duration) and was based on the winter season, as reported previously. 11 We included all first lifetime VTE events that occurred from study enrolment through to 2017. The diagnosis of DVT or PE required positive imaging tests and they were identified by computer linkage to the National Hospital Discharge Registry data maintained by the Finnish Institute for Health and Welfare. The research protocol was approved by the Institutional Review Board of the University of Eastern Finland. Written informed consent was obtained from all participants and all study procedures were conducted according to the Declaration of Helsinki. The current analysis is based on 2259 men with no history of VTE at study entry and with complete information on leisure-time cross-country skiing habits, relevant covariates and VTE events. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated using Cox proportional hazard regression models. We conducted all statistical analyses using Stata version MP 16 (Stata Corp, College Station, TX, USA).
Baseline participant characteristics overall and by levels of total volume of leisure-time cross-country skiing.
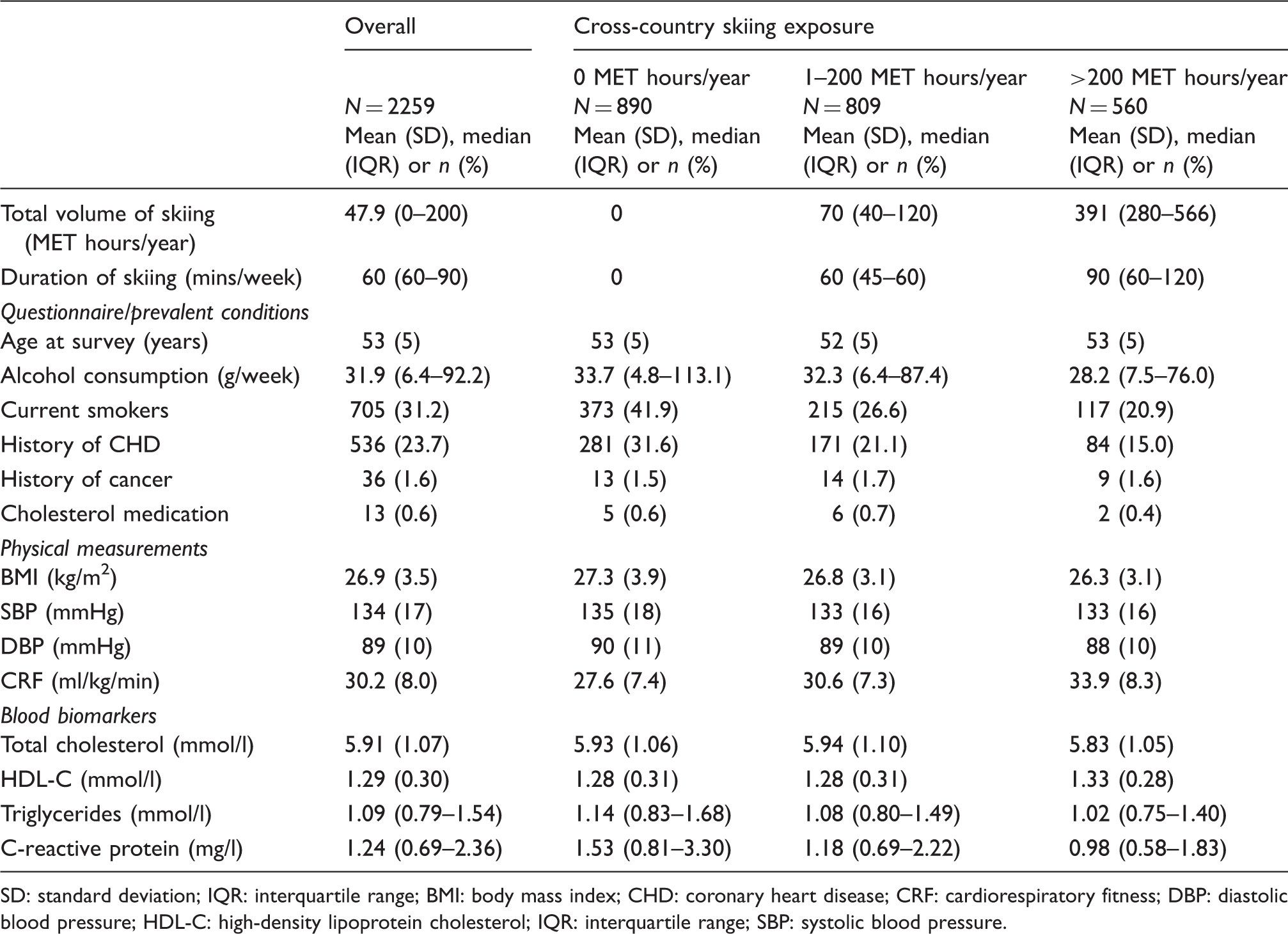
SD: standard deviation; IQR: interquartile range; BMI: body mass index; CHD: coronary heart disease; CRF: cardiorespiratory fitness; DBP: diastolic blood pressure; HDL-C: high-density lipoprotein cholesterol; IQR: interquartile range; SBP: systolic blood pressure.
Associations of total volume and duration of leisure-time cross-country skiing with venous thromboembolism.
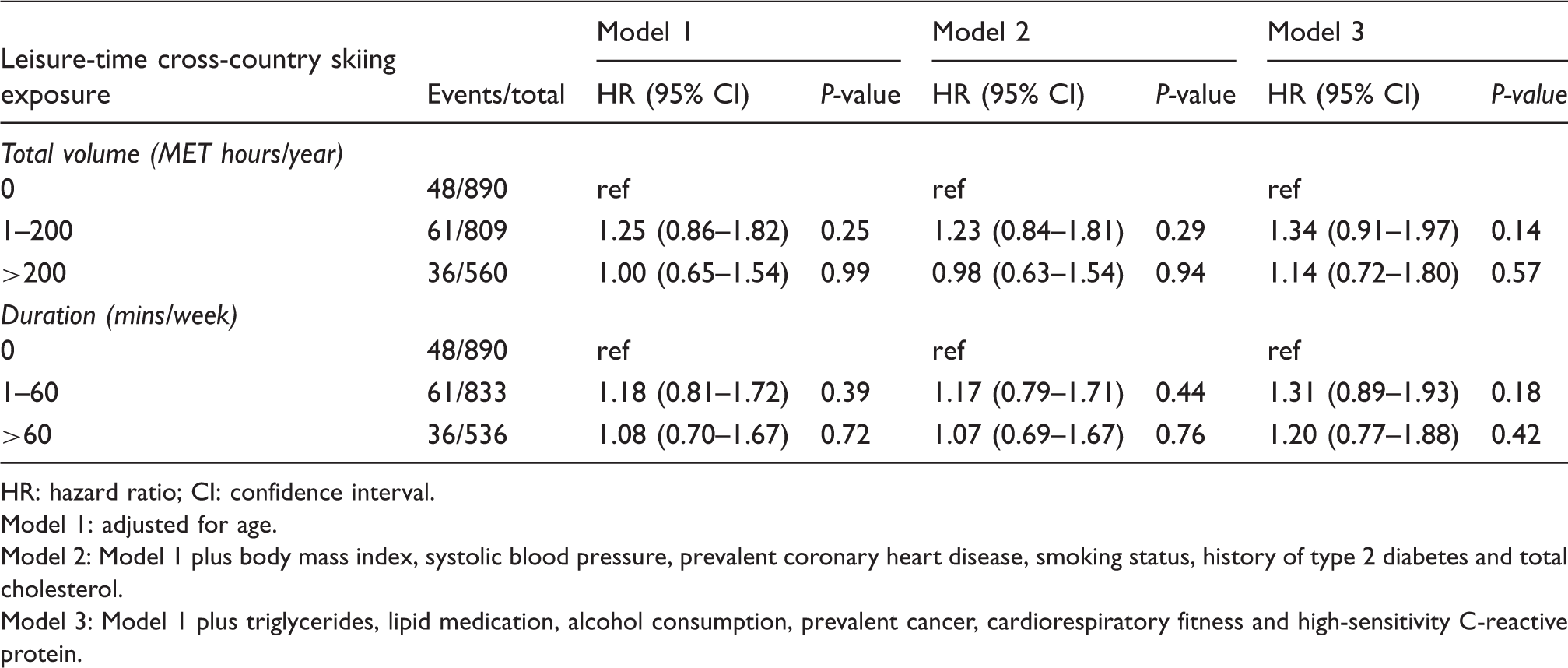
HR: hazard ratio; CI: confidence interval.
Model 1: adjusted for age.
Model 2: Model 1 plus body mass index, systolic blood pressure, prevalent coronary heart disease, smoking status, history of type 2 diabetes and total cholesterol.
Model 3: Model 1 plus triglycerides, lipid medication, alcohol consumption, prevalent cancer, cardiorespiratory fitness and high-sensitivity C-reactive protein.
Though evidence suggests that there is an inverse and independent association between leisure-time cross-country skiing and arterial thrombotic disease,9,10 we found no evidence of an association in this first prospective evaluation between leisure-time cross-country skiing habits and risk of VTE in a general population-based cohort of middle-aged Caucasian men. Given the close inter-relationship between physical activity, atherosclerotic CVD and VTE as a result of shared risk factors and mechanistic pathways, and the fact that cross-country skiing is a high-intensity aerobic activity, these findings, therefore, seem unexpected. Furthermore, a defining characteristic of cross-country skiing is the simultaneous use of the upper and lower body, while simultaneously working both the “pulling” and “pushing” muscles of a lower and upper body; hence, it would be expected that the increased muscular activity of the lower limbs could also increase venous return and decrease VTE risk. 13 We postulate that our null findings could be as a result of important differences between the roles of regular physical activity and leisure-time cross-country skiing in VTE development. Since cross-country skiing is a seasonal activity, which is usually only possible during the winter months, its beneficial effects on atherosclerotic CVD and other adverse health outcomes has been suggested to reflect individuals’ total endurance physical activity. 10 Individuals who participate in long-distance ski racing have high physical activity levels and are likely to maintain regular physical activity throughout the year, which is evidenced by their high levels of CRF, 10 hence the suggestion that cross-country skiing may not have direct independent effects on atherosclerotic CVD. Furthermore, compared with endurance cross-country skiing, it is possible the intensity and volume of leisure-time cross-country skiing may not be adequate enough to provide beneficial effects on VTE. However, this is a purely speculative reason as there is no previously published observational study showing a beneficial effect of endurance cross-country skiing on the incidence of VTE. Another possibility for the null findings may reflect aetiological differences between arterial thrombotic disease and VTE. Though evidence suggests that these two disease conditions are closely related, they have historically been viewed as two distinct diseases 14 and it is generally believed that their pathogenesis differ. 15 Finally, the absence of evidence of an association could reflect study design factors and population characteristics such as (a) regression dilution bias due to the long follow-up duration; (b) residual confounding; and (c) age, sex or genetic background of the population. Due to the absence of previous investigations on the topic, other large-scale studies are needed to confirm or refute these findings.
Strengths of the current evaluation which are worth mentioning include the novelty; the large general population representative sample of middle-aged men with no history of pre-existing VTE at study entry; the long-term and zero loss to follow-up; and adjustment for a comprehensive panel of lifestyle and biological markers. There were some limitations and these included the relatively low VTE event rate attributed to the fact VTE is not necessarily a common outcome in approximately healthy middle-aged men; the inability to generalize the findings to women and other age groups; the absence of repeat assessments of cross-country skiing habits and, hence, inability to correct for regression dilution bias; the potential for misclassification bias due to the use of self-reported questionnaires in assessing cross-country skiing habits; biases inherent to observational cohort designs such as residual confounding and reverse causation; and the inability to evaluate specific VTE outcomes such as DVT and PE, due to availability of only total VTE outcomes.
In conclusion, there is no strong evidence to show that leisure-time cross-country skiing is associated with the risk of VTE in middle-aged Caucasian males. These findings support and extend evidence that potential risk factors for VTE and arterial thrombotic disease may not be similar and their pathogenesis may also differ. Nevertheless, investigations into the inter-relationship between leisure-time cross-country skiing, competitive or endurance cross-country skiing and VTE are warranted.
Footnotes
Author contribution
SKK, SK, TM and JAL contributed to the conception and design of the work. All authors contributed to the acquisition, analysis or interpretation of data for the work. SKK, SK, TM and JAL drafted the manuscript. All authors critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgements
Our gratitude is extended to the team of the of the Kuopio Research Institute of Exercise Medicine and the Research Institute of Public Health and University of Kuopio, Finland, for the collection and provision of the data for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Kuopio Ischemic Heart Disease Study was supported by the Finnish Foundation for Cardiovascular Research, Helsinki, Finland. SKK acknowledges support from the NIHR Biomedical Research Centre at University Hospitals Bristol NHS Foundation Trust and the University of Bristol (BRC-1215-20011).