
Abstract
Background
European Action on Secondary and Primary Prevention by Intervention to Reduce Events (EUROASPIRE) V in primary care was carried out by the European Society of Cardiology EURObservational Research Programme in 2016–2018. The main objective was to determine whether the 2016 Joint European Societies’ guidelines on cardiovascular disease prevention in people at high cardiovascular risk have been implemented in clinical practice.
Methods
The method used was a cross-sectional survey in 78 centres from 16 European countries. Patients without a history of atherosclerotic cardiovascular disease either started on blood pressure and/or lipid and/or glucose lowering treatments were identified and interviewed ≥ 6 months after the start of medication.
Results
A total of 3562 medical records were reviewed and 2759 patients (57.6% women; mean age 59.0 ± 11.6 years) interviewed (interview rate 70.0%). The risk factor control was poor with 18.1% of patients being smokers, 43.5% obese (body mass index ≥30 kg/m2) and 63.8% centrally obese (waist circumference ≥88 cm for women, ≥102 cm for men). Of patients on blood pressure lowering medication 47.0% reached the target of <140/90 mm Hg (<140/85 mm Hg in people with diabetes). Among treated dyslipidaemic patients only 46.9% attained low density lipoprotein-cholesterol target of <2.6 mmol/l. Among people treated for type 2 diabetes mellitus, 65.2% achieved the HbA1c target of <7.0%.
Conclusion
The primary care arm of the EUROASPIRE V survey revealed that large proportions of people at high cardiovascular disease risk have unhealthy lifestyles and inadequate control of blood pressure, lipids and diabetes. Thus, the potential to reduce the risk of future cardiovascular disease throughout Europe by improved preventive cardiology programmes is substantial.
Introduction
The main objectives of cardiovascular disease (CVD) prevention are to reduce morbidity and mortality, improve quality of life and increase life expectancy. 1 The Joint European Societies (JES) guidelines on CVD prevention have been regularly updated since 19941–6 and their implementation evaluated with five cross-sectional surveys called EUROASPIRE (European Action on Secondary and Primary Prevention by Intervention to Reduce Events) from 1995–1996 to 2016–2018 through the European Society of Cardiology (ESC) EURObservational Research Programme (EORP).7–17
Primary prevention of atherosclerotic CVD remains a major challenge. Observational studies and randomised controlled trials verify that healthy lifestyles and the control of arterial hypertension, dyslipidaemia and diabetes prevent CVD events in people free from such disease.18–25 The aim of the primary care arm of EUROASPIRE V was to determine to what extent the 2016 JES guidelines on CVD prevention had been implemented in clinical practice in people at high risk of developing CVD.
Methods
Study design
The primary care arm of EUROASPIRE V was carried out in 78 primary care centres in 16 countries (Bosnia and Herzegovina, Bulgaria, Croatia, the Czech Republic, Egypt, Greece, Kazakhstan, Kyrgyzstan, Lithuania, Poland, Portugal, Romania, Russia, Sweden, Ukraine and the United Kingdom) during 2017–2018. Within each country one or more areas with a defined population were selected and a sample of ≥2 general practices serving that population were identified.
Study population
Men and women, ≥18–<80 years, free from any atherosclerotic disease, who had been prescribed one or more of the following: (a) blood pressure lowering drugs and/or (b) lipid-lowering drugs and/or (c) glucose-lowering (diet and/or oral drugs and/or insulin) ≥6 months to <2 years prior to the interview, were retrospectively identified from the medical records. The sampling principle was that patients treated for hypertension, dyslipidaemia or diabetes had an approximately equal chance of being included. Patients on each of these treatments might have one or more of the other drug therapies.
Data collection
Data collection was undertaken by trained research staff, who reviewed the medical notes and invited the patients to an interview and examination at least six months after the prescription of the blood pressure, lipid-lowering and diabetes therapy. Fasting (at least 12 h) blood samples were obtained at the same time.
Smoking was defined as self-reported smoking, and/or a breath carbon monoxide exceeding 10 ppm using a Smokerlyzer (Bedfont Scientific, Model Micro+).
Height and weight were measured in light indoor clothes without shoes using SECA scales 701 and measuring stick model 220 (SECA Medical Measuring Systems and Scales, Birmingham, UK). Overweight was defined as a body mass index (BMI) ≥25–<30 kg/m2 and obesity as BMI ≥ 30 kg/m2.
Waist circumference was measured using a metal tape horizontally in the mid-axillary line midway between the lowest rim of the rib cage and tip of the hip bone with the patient standing. Abdominal overweight was defined as a waist circumference of ≥80–<88 cm for women and ≥94–<102 cm for men and central obesity as a waist circumference of ≥88 cm for women and ≥102 cm for men.
Blood pressure was measured twice on the right upper arm in a sitting position with an automatic digital Omron Comfort M6 sphygmomanometers (OMRON Corporation, Kyoto, Japan) and the mean was used for the analyses. This sphygmomanometer has a specially designed Intelli Wrap Cuff Technology to give more accurate measurements as the unique pre-formed Comfort cuff adjusts to suit a variety of arm sizes and shapes. Raised blood pressure was defined as systolic blood pressure (SBP) ≥140 mm Hg and/or diastolic blood pressure (DBP) ≥90 mm Hg (≥140/85 mm Hg in patients with diabetes)
The physical activity target was defined by the following question ‘Do you take regular physical activity of at least 30 minutes duration on average five times a week?’
Blood samples were analysed in the Central Laboratory (Laboratory in the National Institute for Health and Welfare, Helsinki, Finland), accredited by the Finnish Accreditation Service and fulfilling requirements of the standard SFS-EN ISO/IEC 17025:2005. During the course of the study the coefficient of variation (mean ± standard deviation (SD)) and systematic error (mean ± SD) were 1.2% ± 0.1 and 0.0% ± 1.0 for total cholesterol, 1.9% ± 0.5 and –0.1% ± 2.4 for high density lipoprotein-cholesterol (HDL-C), 1.3% ± 0.2 and –1.8% ± 2.0 for triglycerides and 0.9% ± 0.1 and –2.1% ± 3.4 for glycated haemoglobin (HbA1c), respectively. Total cholesterol, HDL-C and triglycerides were analysed in serum, and HbA1c in whole blood by enzymatic methods for total cholesterol, triglycerides and HbA1c and a homogenous method for direct measurement of HDL-C (reagents from Abbott Laboratories, Abbott Park, Illinois, USA). The level of low density lipoprotein-cholesterol (LDL-C) was calculated by Friedewald’s formula when the triglycerides level was <4.5 mmol/l. 26 Elevated LDL-C concentration was defined as ≥2.6 mmol/l (≥100 mg/dl).
Plasma glucose was analysed locally with a point-of-care technique (Glucose 201RT, HemoCue, Ängelholm, Sweden). 27 Elevated fasting glucose among patients with diabetes was defined as ≥6.0 mmol/l (≥110 mg/dl) and elevated HbA1c as ≥7.0% (International Federation of Clinical Chemistry (IFCC) ≥ 53 mmol/mol).
Data management
Data were submitted online to the data management centre (EORP, European Heart House, Sophia Antipolis, France). They were checked for completeness, internal consistency and accuracy and stored under the provisions of the National Data Protection Regulations.
Statistical analyses
Descriptive statistics were used to estimate the prevalence rates of risk factors and medication use at interview. Patients’ demographics, risk factor profiles and use of medication were described according to unweighted means, SDs and proportions. Prevalences were compared between gender and age groups according to Fisher’s exact test. All statistical analyses were undertaken using SAS statistical software (release 9.4, SAS Institute, Cary, North Carolina, USA) in the Department of Public Health, Ghent University, Belgium.
Ethical approval
National coordinators were responsible for obtaining local ethics committee approvals. Written, informed consent was obtained from each participant and stored in the patient file.
Outcome measures
The main outcome measures were the proportions of high CVD risk people achieving the lifestyle and risk factor targets as defined in the 2016 JES guidelines on CVD prevention: not smoking, healthy food choices and being physically active; a BMI < 25 kg/m2; blood pressure <140/90 mm Hg (<140/85 mm Hg in patients with diabetes), LDL-C < 2.6 mmol/l (<100 mg/dl), HbA1c as <7.0% (IFCC < 53 mmol/mol) and appropriate use of cardioprotective drug therapies for treatment of elevated blood pressure, lipids and glucose. 1
Results
Characteristics of the study population
A total of 3562 medical records were reviewed and 2759 patients attended the interview which, excluding patients who died, moved away and had a change in medical condition, corresponds to a participation rate of 70%. The distribution of study population attending interview by country, age and gender is presented in Supplementary Material Table 1. The mean (SD) age at interview was 59.0 (11.6) years and 57.6% were women.
Reasons for not being interviewed were: refusal to attend (62%), no response to the invitation letter (36%) and miscellaneous (2%). Women were significantly more likely to attend the interview (74% vs 66% in men).
Study outcomes
Lifestyle
The prevalence of smoking, obesity and central obesity are presented in Tables 1 and 2, Figure 1 and Supplementary Material Table 2.
Prevalence (%) of smokinga by age and sex.b Patients’ lifestyle characteristics by age and gender. ACE : Angiotensin converting enzyme; BMI: body mass index; LLD: lipid-lowering drugs. Smoking: self-reported smoking or >10 ppm carbon monoxide in breath; persistent smoking: self-reported smoking or >10 ppm carbon monoxide in breath in patients reporting to have been smoking in the month prior to the index event; overweight: BMI 25–30 kg/m2; obesity: BMI ≥ 30 kg/m2; central obesity: waist circumference ≥88 cm for women and ≥102 cm for men. p < 0.01; bp < 0.05. Reported lifestyle changes taken by patients to reduce their risk of heart disease within the last three years by age and gender. BMI: body mass index; BP: blood pressure. Change during the last three years reported by smokers; bp < 0.05; cp < 0.01; dprescribed by a doctor or other health professional.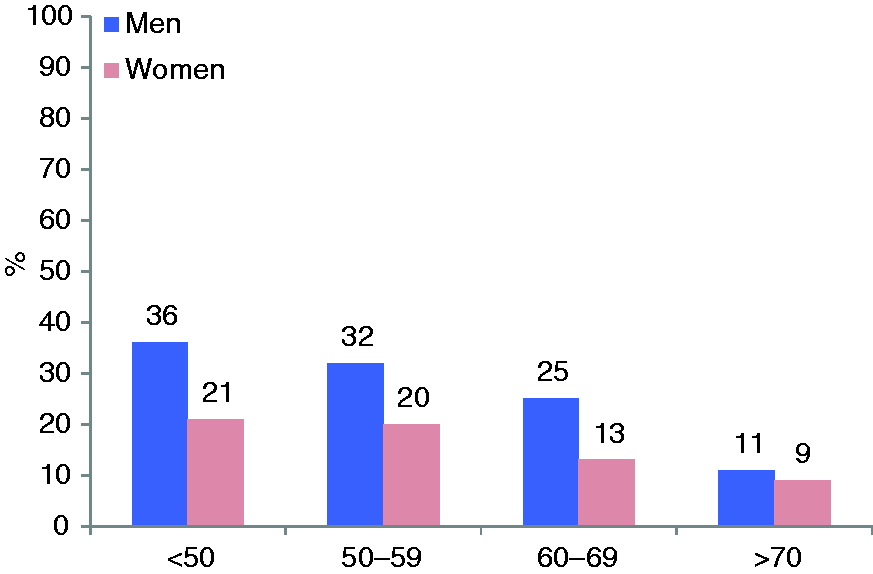
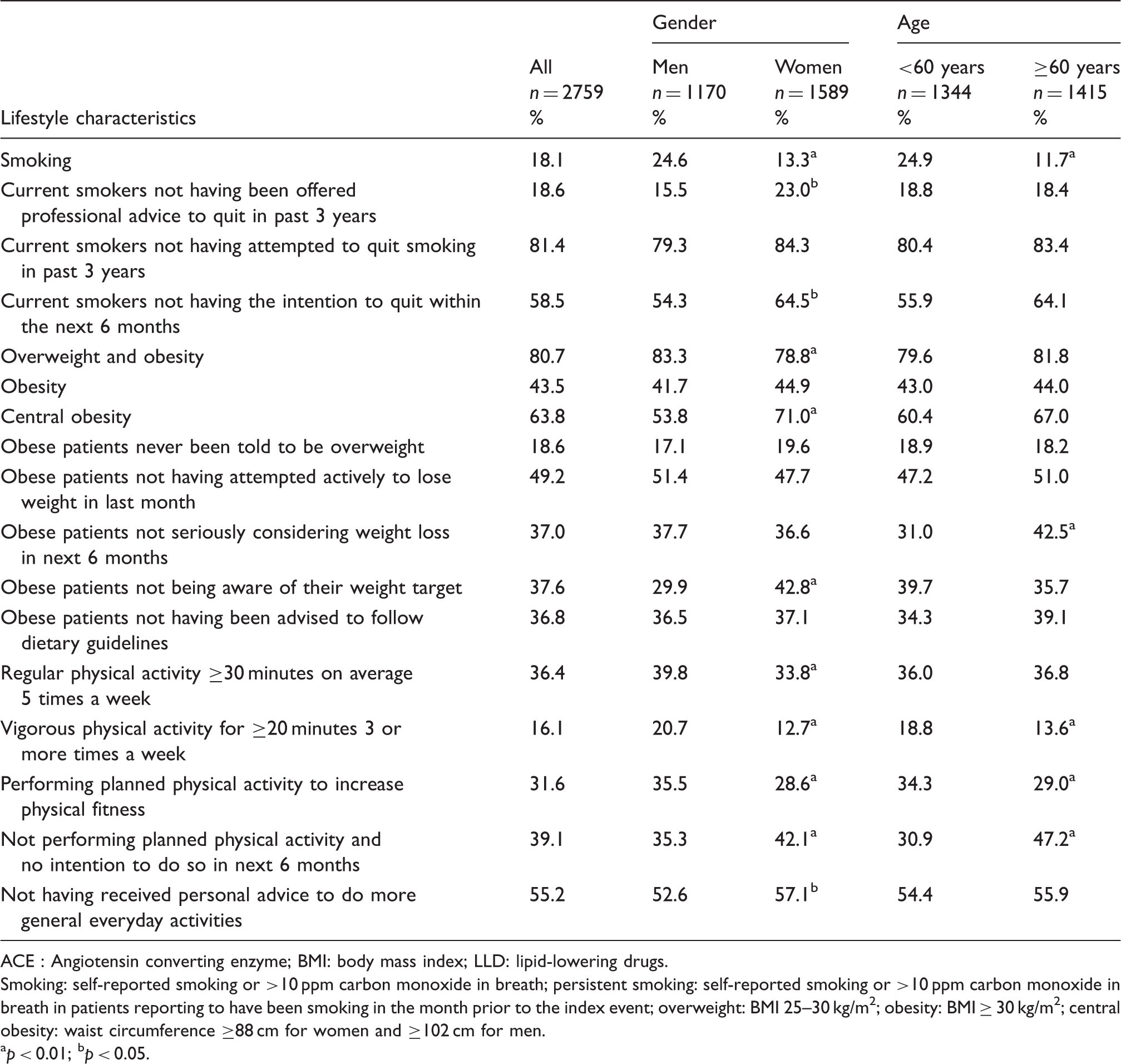
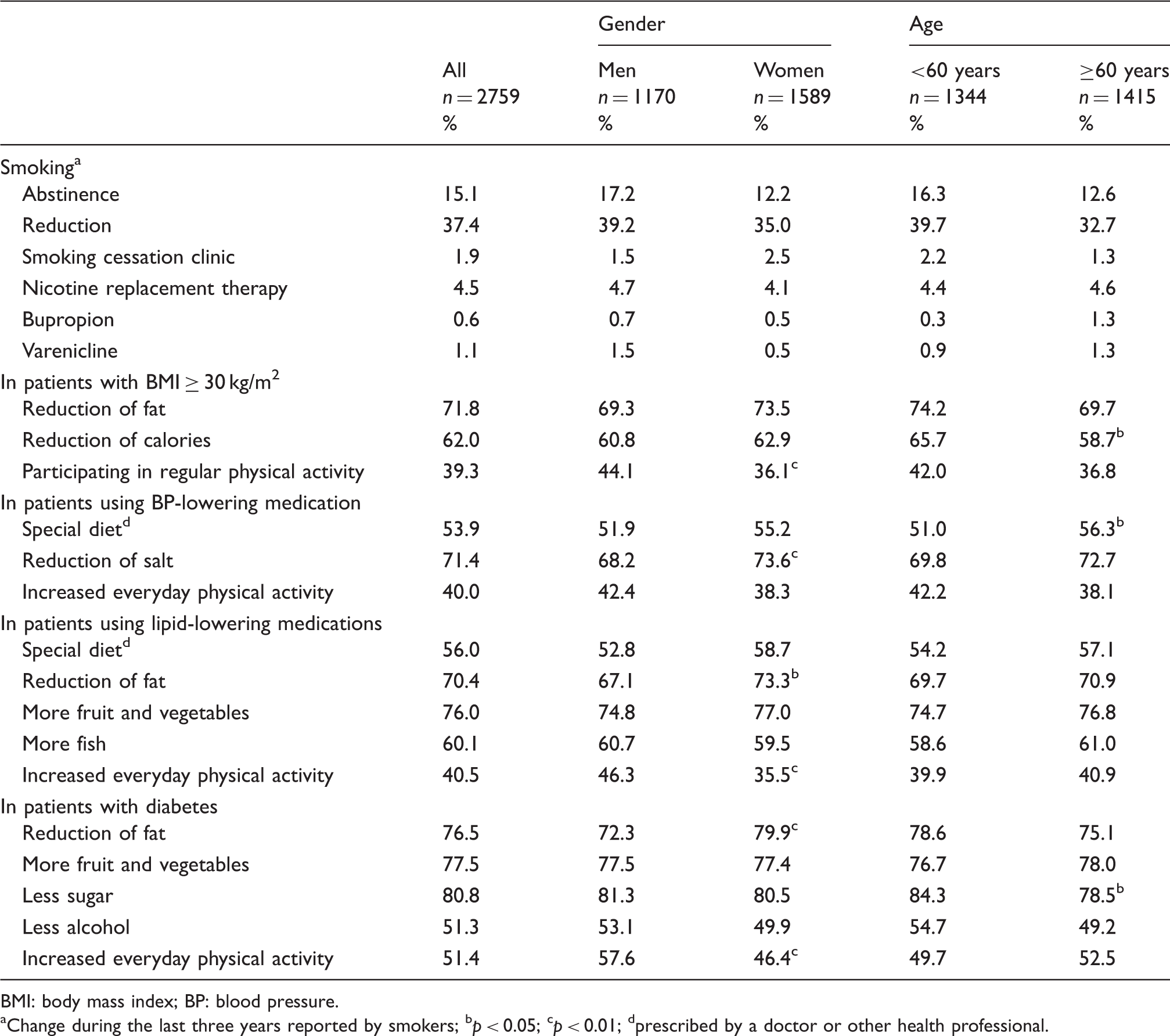
The overall prevalence of smoking was 18.1% (men 24.6%, women 13.3%), higher in patients <60 years. In the past three years 18.6% of current smokers had not been offered professional advice to quit and 58.5% reported no intention to stop within the next six months. Of the persistent smokers, 1.9% attended smoking-cessation clinics and nicotine-replacement and varenicline were used by 4.5% and 1.1% respectively.
Overall, 37.2% of patients (men 41.6%, women 33.9%) were overweight and 43.5% (men 41.7%, women 44.9%) were obese. The prevalence of central obesity was 63.8% (men 53.8%, women 71%). Of obese patients, 18.6% had never been informed that they were overweight, 37.6% were unaware of their weight target and 36.8% had not been advised to follow dietary guidelines.
Regular physical activity (≥30 min on average five times/week) was undertaken by 36.4% of the patients (men 39.8%, women 33.8%) while 39.1% did not perform any planned physical activity and had no intention to do so the next six months and 55.2% had not received any advice to increase their physical activities
Blood pressure, lipids and diabetes
Cardiovascular risk factor management by age and gender.
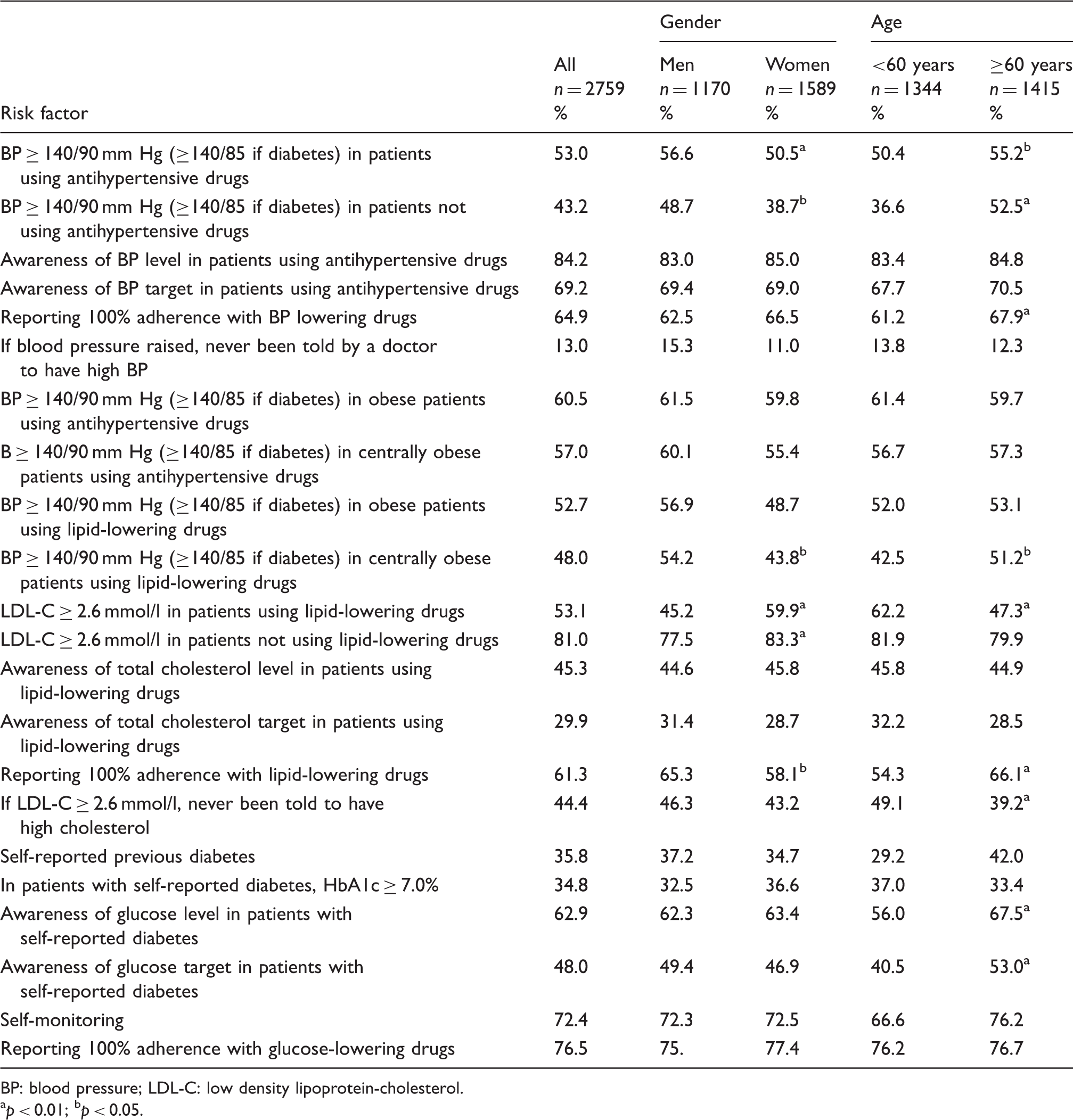
BP: blood pressure; LDL-C: low density lipoprotein-cholesterol.
p < 0.01; bp < 0.05.
Use of blood pressure (BP) lowering, lipid-lowering and antidiabetic therapies.
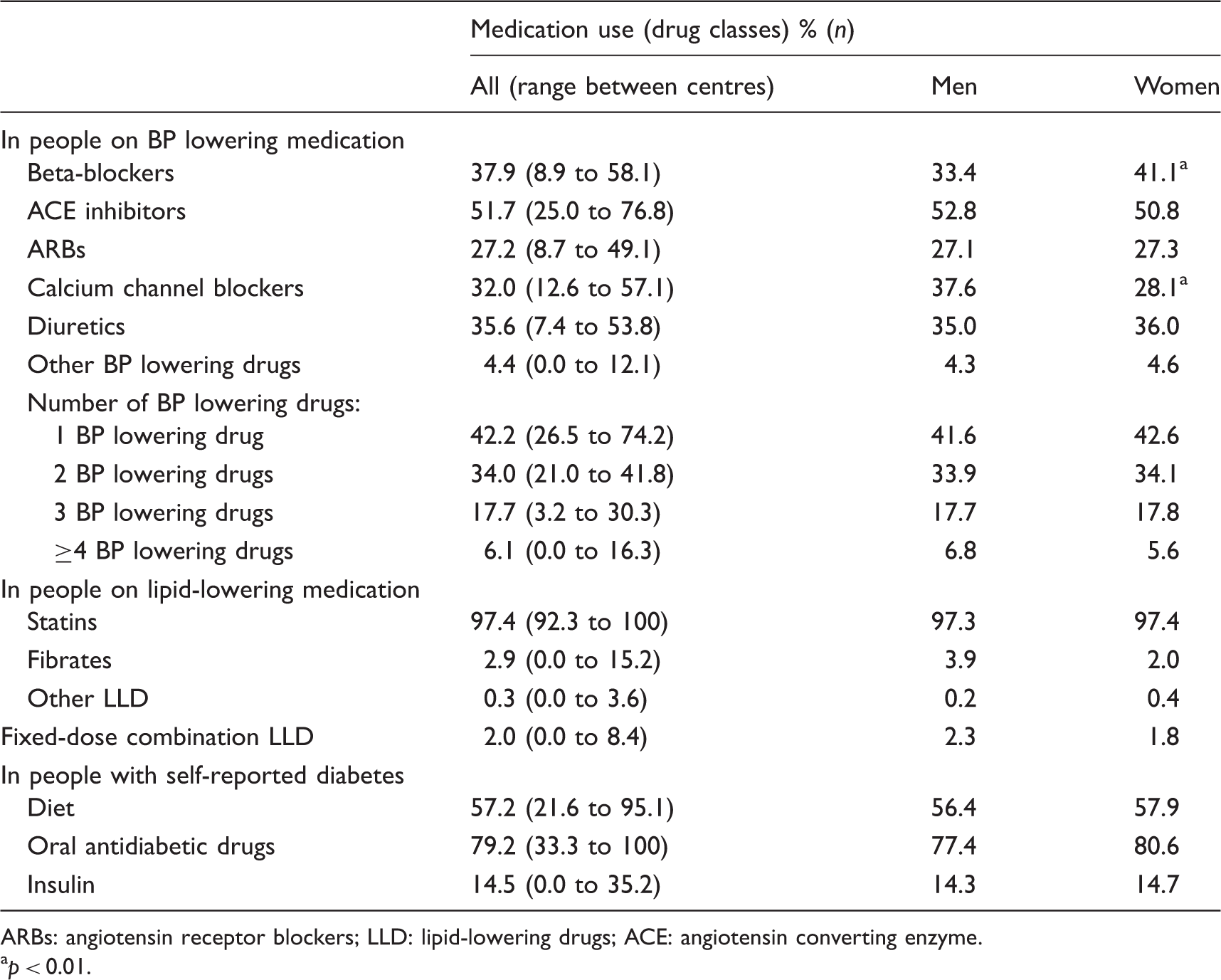
ARBs: angiotensin receptor blockers; LLD: lipid-lowering drugs; ACE: angiotensin converting enzyme. ap < 0.01.
Overall, 75.4% of patients were on antihypertensive medication but 53% (men 56.6%, women 50.5%) had blood pressure ≥140/90 mm Hg (≥140/85 mm Hg in people with diabetes). A total of 84.2% on blood pressure therapy were aware of their blood pressure level and 69.2% knew their recommended target. The most common medications were inhibitors of renin-angiotensin systems (ACE inhibitors/angiotensin receptor blockers (ARBs); 78.9%), followed by beta-blockers (37.9%), diuretics (35.6%) and calcium channel blockers (32%) with 42.2% on one, 34% on two, 17.7% on three and 6.1% on ≥4 blood pressure lowering drugs. Two-thirds of patients (64.9%) reported complete adherence with the intake of their blood pressure lowering drugs. Furthermore, blood pressure was elevated in 43.2% of patients not using antihypertensive medication. Of those being treated for hypertension 31.0% were also on lipid-lowering medication and 50.4% had an LDL-C ≥ 2.6 mmol/l. Of those with hypertension not on lipid-lowering medication 80.8% had an LDL-C ≥ 2.6 mmol/l.
Lipid-lowering medication was prescribed in 34.1% and in this group 97.3% were on statins, 2.9% on fibrates and 0.3% on other lipid-lowering drugs. Overall, 61.3% reported 100% adherence with lipid-lowering drugs. Still, 53.1% of these patients (men 45.2%, women 59.9%) had LDL-C ≥ 2.6 mmol/l. Of these, 45.3% had been informed of their cholesterol levels and only 29.9% were aware of their target. Of patients on no lipid-lowering medication 81% had a LDL-C ≥ 2.6 mmol/l (men 77.5%, women 83.3%). Of those being treated for dyslipidaemia, 70.8% were also on anti-hypertensive medication and 48.9% had a blood pressure above the recommended target. Of dyslipidaemic patients not on anti-hypertensive medication, 35.6% had a blood pressure above the target.
The prevalence of self-reported diabetes at interview was 35.8% (men 37.2%, women 34.7%) and 34.8% of people in this group had a HbA1c ≥ 7.0%. The majority (79.2%) were on oral glucose-lowering drugs, 14.5% on insulin and 57.2% on diet; 76.5% reported 100% adherence with glucose-lowering drugs. In patients with known diabetes, ACE inhibitors/ARBs were prescribed in 56.0%, statins in 38.0% and both statins and ACE/ARBs in 26.0%. Of those with diabetes, 69.8% were on anti-hypertensive medication and 64.8% had a blood pressure ≥ 140/85 mm Hg. Of those with diabetes not on anti-hypertensive medication, 55.1% had a blood pressure ≥140/85 mm Hg. A total of 39.5% were on lipid-lowering medication but 41.9% had an LDL-C ≥ 2.6 mmol/l. Of those with diabetes not on lipid-lowering medication, 74.5% had an LDL-C ≥ 2.6 mmol/l.
Discussion
Principal findings
The EUROASPIRE V survey in primary care clearly demonstrates that a large majority of patients at high CVD risk fail to achieve lifestyle, blood pressure, lipid and glycaemic targets as defined in the 2016 JES guidelines on CVD prevention in clinical practice. A wide gap still exists between the evidence-based guidelines and everyday clinical practice.
A major concern is that nearly one-fifth of high CVD risk patients were smokers with a prevalence higher in men than women and in patients <50 years. Moreover, two-fifths of current smokers did not intend to quit smoking within the next six months. Despite the evidence that stopping smoking is the most cost-effective strategy for prevention of CVD,1,28 only a small minority of patients attended smoking cessation clinics or were prescribed pharmacological support. There is a failure of the primary care system to provide professional support for smoking cessation, including prescription of evidence based medications like varenicline and buproprion, and to address all aspects of lifestyle including recommending physical activity, especially in older groups. These poor outcomes on smoking and physical activity management in such high risk patients could be seen as professional negligence.
A large majority of high CVD risk patients were overweight or obese and nearly two-thirds were centrally obese with the highest prevalence in women. Of concern is that one-fifth of obese patients were never told that they were overweight, and that more than a third were unaware of their weight target and without any dietary recommendations. Healthy diet and weight reduction in overweight and obese patients are recommended in order to reduce the blood pressure, lipids and the risk of diabetes mellitus type 2.1,29 In this survey, the majority of obese patients reported reducing fat and calorie intake but only two-fifths participated in regular physical activity.
There is a wealth of scientific evidence that control of blood pressure, lipids and glucose can reduce the risk of future CV events in high risk patients.21–25 However, blood pressure management was poor with less than half of patients on blood pressure lowering medication achieving the guideline targets, slightly better in women than men. Although a majority of patients were aware of their blood pressure level and the target to be achieved only 65% reported complete adherence with their treatment. Of note is that more than two-fifths of high CVD risk patients, because of dyslipidaemia and/or diabetes, had elevated blood pressure without being prescribed any antihypertensive therapy. The management of LDL-C was surprisingly poor, with less than half of patients on lipid-lowering medication achieving the recommended target. Lipid control was better in men than women. Surprisingly, less than half of patients on lipid-lowering medication were aware of their cholesterol levels and less than a third knew their cholesterol target. However, over three-fifths of patients reported 100% adherence with lipid-lowering drugs. Similar to blood pressure, the majority of patients selected as being at high risk, because of treated hypertension and/or diabetes, had elevated LDL-C but without any prescription of lipid-lowering therapy. More than two-fifths of patients with elevated LDL-C had never been told they had high cholesterol. In this survey, blood pressure was better controlled in women than men and the reverse was true for LDL-C, with similar observations reported in previous EUROASPIRE III and IV surveys in primary care.14–16
There may be several explanations for the poor blood pressure and lipid management, such as low-dose prescriptions, not up-titrating doses to achieve targets, using monotherapy, poor patient adherence and physician inertia to treat patients to targets according to the most recent guidelines. Large clinical trials demonstrate that most patients with hypertension can achieve and sustain adequate blood pressure control, however only with the use of two or more blood pressure lowering drugs. In this survey, more than two-fifths of patients on anti-hypertensive therapy were on only one, while one-third were on two and just one-fourth on three or more blood pressure lowering drugs.
According to the JES guidelines, people with diabetes mellitus type 2 should be considered and managed as high CVD risk and prescribed cardioprotective medications including ACE inhibitors/ARBs and statins. 1 However, in this survey more than a third of patients with known diabetes had HbA1c above the recommended target of <7%. Overall, nearly three-fifths were on ACE inhibitors/ARBs and only just over one-third on statins.
One important finding of this survey is that a large majority of patients identified on the basis of being on blood pressure and/or lipid-lowering medications and/or having diabetes, were found to have more than one of these risk factors. Counting the number of uncontrolled cardiovascular risk factors (current smoking, elevated blood pressure, elevated LDL-C or uncontrolled diabetes), 38.7% had one, 40.1% had two, 10.8% had three and 0.6% had four of them inadequately managed. This underlines the importance of multifactorial cardiovascular risk factor management as the total CVD risk is a consequence of the interaction of many risk factors and modest increases of several risk factors can be more harmful than a high level of a single risk factor. Treating single risk factors in isolation is less effective than screening for and managing all CVD risk factors, and where one risk factor is detected it is essential to screen for and manage all the others.
Comparison with other surveys
The results of EUROASPIRE V are in accordance with other earlier surveys of primary prevention in Europe, USA and other parts of the world.30–34 Most of them focused on the control of a single risk factor while the information on management of multiple CVD risk factors in patients at high CVD risk is limited. By comparison with the EURIKA study on 7641 patients from 12 European countries free of clinical CVD, and with at least one major CVD risk factor, blood pressure and LDL-C control in EUROASPIRE V was slightly better. 30 Among patients with treated hypertension, 39% of patients in EURIKA achieved the blood pressure target compared to 47% of patients in EUROASPIRE V. Among treated patients with dyslipidaemia, 41% of patients in EURIKA attained an LDL-C of <3 mmol/l, compared to 47% achieving LDL-C of <2.6 mmol/l in EUROASPIRE V. In another European study, 32% of high CVD risk patients were smokers, 36% were obese, 49% had blood pressure >140/90 mm Hg, 64% total cholesterol ≥5 mmol/l and 14% a fasting glucose levels >6.1 mmol/l. 31 Predictors of risk factor control were medication adherence and health-related quality of life. Being single and having a lower educational level was associated with poorer risk factor control. The International ChoLesterol management Practice Study (ICLPS) investigated achievement of LDL-C targets in patients at high or very high CVD risk receiving lipid-modifying therapy in countries outside Western Europe. 32 The proportion of patients achieving guideline-specified treatment targets was 44% for LDL-C, 55% for blood pressure and 39% for diabetes.
Strengths and limitations
A major strength is that data were collected using face-to-face interviews with standardised methods and equipment, including central laboratory analyses, rather than data from general practice medical records where the risk factor recording is usually incomplete. A limitation may be the way that patients were identified, through prescription of blood pressure and/or lipid-lowering and/or diabetes therapies, rather than screening to detect those at highest multifactorial CVD risk. High CVD risk screening would have been labour-intensive requiring assessment of a large number of people to detect those at highest risk, while selecting those already at high medical risk because they were being treated with drug therapies was easier. The majority of these selected patients had more than one risk factor which puts them at high multifactorial risk for CVD requiring a comprehensive approach to risk factor reduction. The reason for choosing three geographical regions with a minimum of two general practices in each area in each country was to increase the representativeness of the study.
Conclusions
Many European patients at high CVD risk have unhealthy lifestyles including sedentary behaviour and high prevalence of smoking, overweight, obesity and central obesity. The control of blood pressure, lipids and diabetes is poor with the majority of patients not achieving guideline-recommended targets for CVD prevention. There were considerable variations between countries in lifestyle and risk factor management that may be explained by the differences in drug prescribing and local healthcare policies. The results demonstrate that both patients and physicians pay insufficient attention to lifestyle risk factors which can unfavourably impact on the control of blood pressure, lipids and diabetes. Thus, there is considerable potential to raise the standards of preventive cardiology through modern preventive cardiology programmes 35 addressing all aspects of lifestyle, multifactorial risk factor management supported by comprehensive pharmacological therapy in order to reduce the risk of future CVD.
Supplemental Material
CPR908698 Supplemental Material - Supplemental material for Primary prevention efforts are poorly developed in people at high cardiovascular risk: A report from the European Society of Cardiology EURObservational Research Programme EUROASPIRE V survey in 16 European countries
Supplemental material, CPR908698 Supplemental Material for Primary prevention efforts are poorly developed in people at high cardiovascular risk: A report from the European Society of Cardiology EURObservational Research Programme EUROASPIRE V survey in 16 European countries by Kornelia Kotseva, Guy De Backer, Dirk De Bacquer, Lars Rydén, Arno Hoes, Diederick Grobbee, Aldo Maggioni, Pedro Marques-Vidal, Catriona Jennings, Ana Abreu, Carlos Aguiar, Jolita Badariene, Jan Bruthans, Renata Cifkova, Kairat Davletov, Mirza Dilic, Maryna Dolzhenko, Dan Gaita, Nina Gotcheva, Hosam Hasan-Ali, Piotr Jankowski, Christos Lionis, Silvia Mancas, Davor Milićić, Erkin Mirrakhimov, Rafael Oganov, Nana Pogosova, Željko Reiner, Duško Vulić, David Wood and on behalf of the EUROASPIRE V Investigators in European Journal of Preventive Cardiology
Footnotes
Author contribution
KK contributed to conception and design, data acquisition, analysis and interpretation, drafted and critically revised the manuscript. GDB, DDB, LR, AH, DG, AM, PMV, CJ and DW contributed to conception and design, data acquisition, analysis and interpretation, and critically revised the manuscript. AA, CA, JBa, JBr, RC, KD, MDi, MDo, DG, NG, HHA, PJ, CL, SM, DM, EM, RO, NP, ZR and DV, contributed to conception and design, data acquisition and critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
The authors wish to acknowledge the Registry Executive Committee and Steering Committee of the EORP. Data collection was conducted by the EORP department from the ESC by Emanuela Fiorucci, Viviane Missiamenou and Florian Larras. All investigators are listed in Appendix 1. The EUROASPIRE Study Group is grateful to the administrative staff, physicians, nurses and other personnel in the hospitals in which the survey was carried out and to all patients who participated in the surveys. Some of the results of this study were presented at the World Congress of Cardiology (5–9 December 2018, Dubai, UAE) and EUROPREVENT congress (11–13 April 2019, Lisbon, Portugal).
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: KK, had grant support from the ESC for the submitted work. JBr was supported by grant No 17-29520A from Agency for Medical Research, Ministry of Health of the Czech Republic for the submitted work.AM reported personal fees from Bayer, Fresenius, Novartis, outside the submitted work; DG reported grants from Esperion and IMI/European Union, outside the submitted work. ZR reported honoraria from Sanofi-Aventis, outside the submitted work. GDB, DDB, LR, AH, PMV, CJ, AA, CA, JBa, RC, KD, MDi, MDo, DG, NG, HHA, PJ, CL, SM, DM, EM, RO, NP, ZR, DV, DW declared that they had no conflict of interest. The authors had full access to the data and took responsibility for its integrity. All authors have read and agreed to the written manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Since the start of EORP, the following companies have supported the EUROASPIRE V survey through research grants to the European Society of Cardiology: Amgen, Daiichi Sankyo, Eli Lilly, Pfizer, Sanofi, Ferrer and Novo Nordisk. The sponsors of the EUROASPIRE surveys had no role in the design, data collection, data analysis, data interpretation, decision to publish, or writing the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.