
Abstract
Background
Functional capacity is used as an indicator for cardiac testing before non-cardiac surgery and is often performed subjectively. However, the value of subjectively estimated functional capacity in predicting cardiac complications is under debate. We determined the predictive value of subjectively assessed functional capacity on postoperative cardiac complications and mortality.
Design
An observational cohort study in patients aged 60 years and over undergoing elective inpatient non-cardiac surgery in a tertiary referral hospital.
Methods
Subjective functional capacity was determined by anaesthesiologists. The primary outcome was postoperative myocardial injury. Secondary outcomes were postoperative inhospital myocardial infarction and one year mortality. Logistic regression analysis and area under the receiver operating curves were used to determine the added value of functional capacity.
Results
A total of 4879 patients was included; 824 (17%) patients had a poor subjective functional capacity. Postoperative myocardial injury occurred in 718 patients (15%). Poor functional capacity was associated with myocardial injury (relative risk (RR) 1.7, 95% confidence interval (CI) 1.5–2.0; P < 0.001), postoperative myocardial infarction (RR 2.9, 95% CI 1.9–4.2; P < 0.001) and one year mortality (RR 1.7, 95% CI 1.4–2.0; P < 0.001). After adjustment for other predictors, functional capacity was still a significant predictor for myocardial injury (odds ratio (OR) 1.3, 95% CI 1.0–1.7; P = 0.023), postoperative myocardial infarction (OR 2.0, 95% CI 1.3–3.0; P = 0.002) and one year mortality (OR 1.4, 95% CI 1.1–1.8; P = 0.003), but had no added value on top of other predictors.
Conclusions
Subjectively assessed functional capacity is a predictor of postoperative myocardial injury and death, but had no added value on top of other preoperative predictors.
Introduction
Cardiac events are among the most important complications after surgery and therefore preoperative cardiac risk assessment is essential. 1 According to current guidelines, estimation of preoperative functional capacity is a key tool in cardiac risk assessment and is used to guide the need for additional cardiac testing.2,3 A functional capacity of less than four metabolic equivalents (METs) is associated with an increased cardiac risk.2–5
The gold standard to determine a patient’s functional capacity is cardiopulmonary exercise testing (CPET).6,7 Although poor functional capacity as measured by CPET is a reasonable predictor of postoperative complications, CPET testing is not widely used, because it is time consuming and expensive. Therefore, in daily practice, preoperative functional capacity is often estimated by the patient’s self-reported activity, clinical observation during preoperative assessment, or a questionnaire such as the Duke activity status index questionnaire (DASI).4,5,8,9 Although subjective assessment of functional capacity is an easy and widely used method, there is conflicting evidence as to whether it is a good predictor of postoperative cardiac complications.4,5,8,10–17 A large study recently showed that preoperative subjective assessment of functional capacity neither accurately identified patients with poor cardiopulmonary fitness nor predicted postoperative morbidity and mortality. 17 The authors therefore recommended that subjective assessment should no longer be used. Despite this, subjective preoperative assessment of functional capacity is a widespread practice and changing long existing habits and incorporating new evidence into guidelines often requires several studies that confirm previous findings.
Therefore, we aimed to determine the added value of subjectively assessed functional capacity for predicting postoperative myocardial injury and infarction in elective surgical patients, on top of other preoperative predictors.
Methods
Study population
This cohort study included patients aged 60 years and over who underwent elective non-cardiac surgery under general or spinal anaesthesia with an expected postoperative length of hospital stay of at least 24 hours. Surgery took place at the University Medical Center Utrecht, a tertiary referral hospital in The Netherlands, between 1 July 2011 and 31 December 2014. A part of this cohort was included in previous publications.18,19 For patients who underwent surgery more than once within one year, only the first surgery was included in the analysis. The local medical ethics committee waived the need for informed consent because only routinely collected patient data were used and data were anonymised before analysis (University Medical Center Utrecht medical research ethics committee 11–120/C and 18-762/C).
Data collection
Data were obtained from electronic medical records. The Dutch municipal personal record database was consulted for mortality data.
Preoperative assessment
All patients visited the preoperative anaesthesia assessment clinic where medical history, physical examination and, if indicated, further diagnostic testing was performed. Patients filled out a short questionnaire with regard to functional capacity (Supplementary Table 1). Functional capacity was estimated by anamnesis and physical examination by the attending anaesthesiologist or anaesthesia nurse. It was reported as poor (1–3 METs), moderate (4–7 METs), good (8–10 METs), high (>10 METs), or unknown in patients who were not able to perform any physical activity.
Outcomes
The primary outcome was postoperative myocardial injury, defined as a troponin-I elevation (>60 ng/L) within the first three postoperative days. Troponin I was analysed using the third-generation enhanced AccuTnI assay (Beckman Coulter, Brea, CA, USA). According to our postoperative care protocol, troponin was measured routinely on these first 3 days after surgery. The cut-off value of 60 ng/L was the 99th percentile with a variation coefficient less than 10%, in accordance with the fourth universal definition of myocardial infarction. 20
Secondary outcomes included postoperative inhospital myocardial infarction (POMI), defined according to the fourth universal definition of myocardial infarction, and all-cause one year mortality. 20 Clinical assessment of POMI was performed by a consultant cardiologist, in addition to retrospective adjudication by an independent cardiologist (RBG).18,19
Statistical analysis
Baseline characteristics were calculated as means, medians or percentages when appropriate. Data on functional capacity were missing in 7% of patients. These data were imputed using a multiple imputation model including patient characteristics, comorbidities and primary outcome data. Five datasets were imputed by the method of fully conditional specification.
Functional capacity was dichotomised into poor (<4 METs) and normal (≥4 METs), in accordance with international guidelines.2,3 Patients in whom the functional capacity was reported as unknown were classified as having a poor functional capacity because the functional capacity in these patients is likely to be poor. 4
Baseline characteristics were compared between patients with a poor and a normal functional capacity, by using the chi-square test for categorical variables and the t-test for continuous variables.
Next, the incidences of the primary and secondary outcomes were compared between patients with a poor and normal functional capacity using the chi-square test, and relative risks (RRs) were calculated. Univariable logistic regression analysis was used to determine the predictive value of functional capacity on myocardial injury. Consequently two regression models were built, in order to determine the added predictive value of functional capacity on top of other known preoperative predictors of mortality or cardiac complications, including the variables from the revised cardiac risk index (RCRI). 21 The first model included the individual variables from the RCRI, and variables that were significantly associated with the outcome in the univariable analysis. In the second model, functional capacity was added to the variables from the first model. The added predictive value of functional capacity was determined by comparing the area under the receiver operating curve (AUROC) of the two aforementioned models. Finally, the positive and negative predictive values of functional capacity were determined.
Subsequently, incidences of inhospital POMI and one year mortality were compared between patients with a poor and normal functional capacity using the chi-square test, and RRs were calculated. Multivariable logistic regression analysis was used to determine the added predictive value of functional capacity on top of other preoperative predictors for inhospital POMI and one year mortality. The variables used in the two regression models for one year mortality were the same as in the model for myocardial injury. Because the incidence of POMI was low, the number of variables in the two regression models for POMI was limited. Therefore only two variables were included in the first model, namely age and RCRI, and in the second model age, RCRI and functional capacity.
In a post-hoc sensitivity analysis, the analysis was repeated in complete cases only, hence after excluding patients with missing data for functional capacity.
Finally, differences between the patient’s self-reported functional capacity and the physician’s reported functional capacity were determined.
Throughout the analysis, a P value less than 0.05 was considered statistically significant. The statistical analysis was performed by using SPSS (release 25 for Windows).
Results
Baseline characteristics in patients with poor and normal functional capacity.
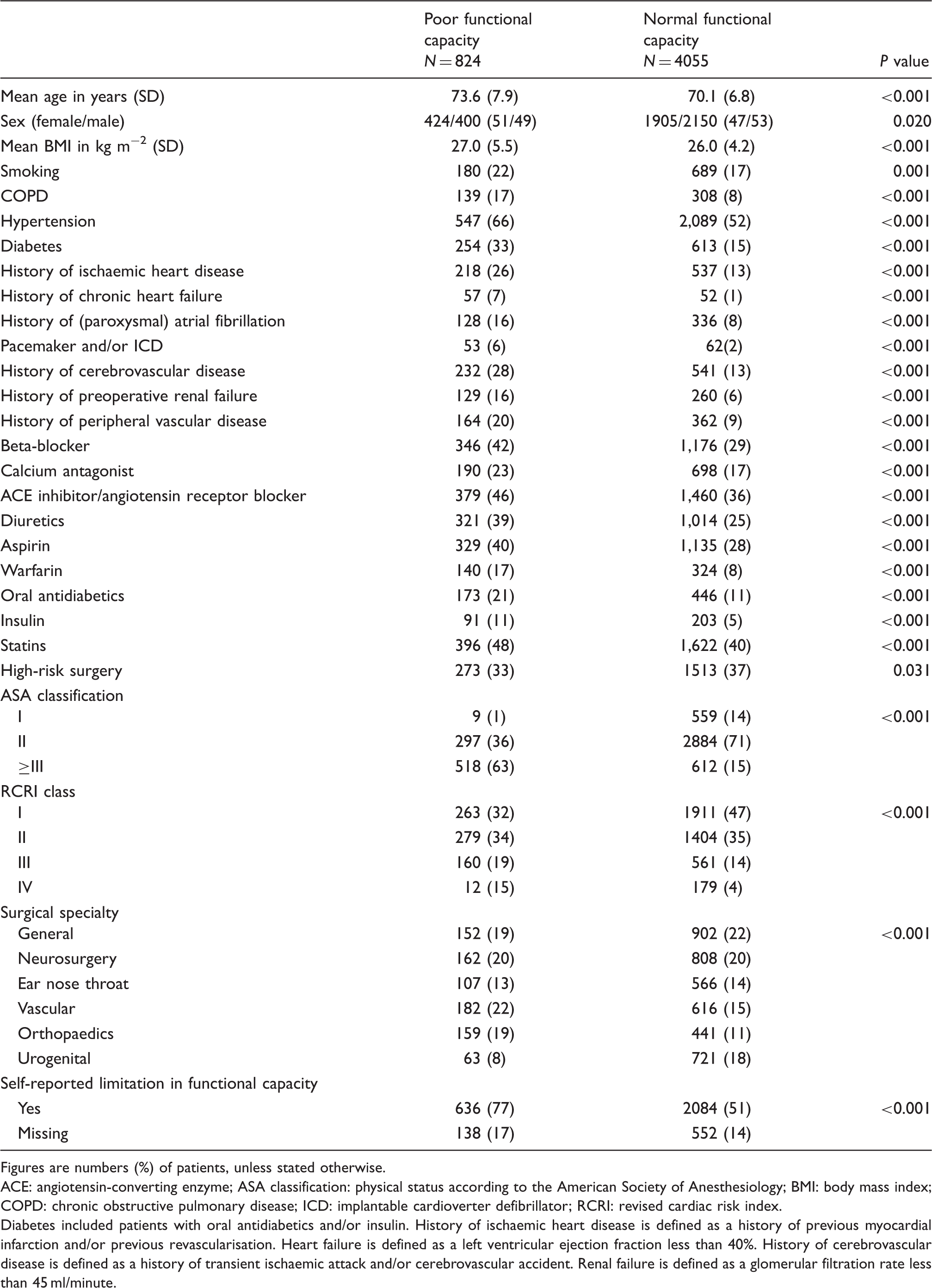
Figures are numbers (%) of patients, unless stated otherwise.
ACE: angiotensin-converting enzyme; ASA classification: physical status according to the American Society of Anesthesiology; BMI: body mass index; COPD: chronic obstructive pulmonary disease; ICD: implantable cardioverter defibrillator; RCRI: revised cardiac risk index.
Diabetes included patients with oral antidiabetics and/or insulin. History of ischaemic heart disease is defined as a history of previous myocardial infarction and/or previous revascularisation. Heart failure is defined as a left ventricular ejection fraction less than 40%. History of cerebrovascular disease is defined as a history of transient ischaemic attack and/or cerebrovascular accident. Renal failure is defined as a glomerular filtration rate less than 45 ml/minute.
Primary outcome
Association between patient characteristics and postoperative myocardial injury.
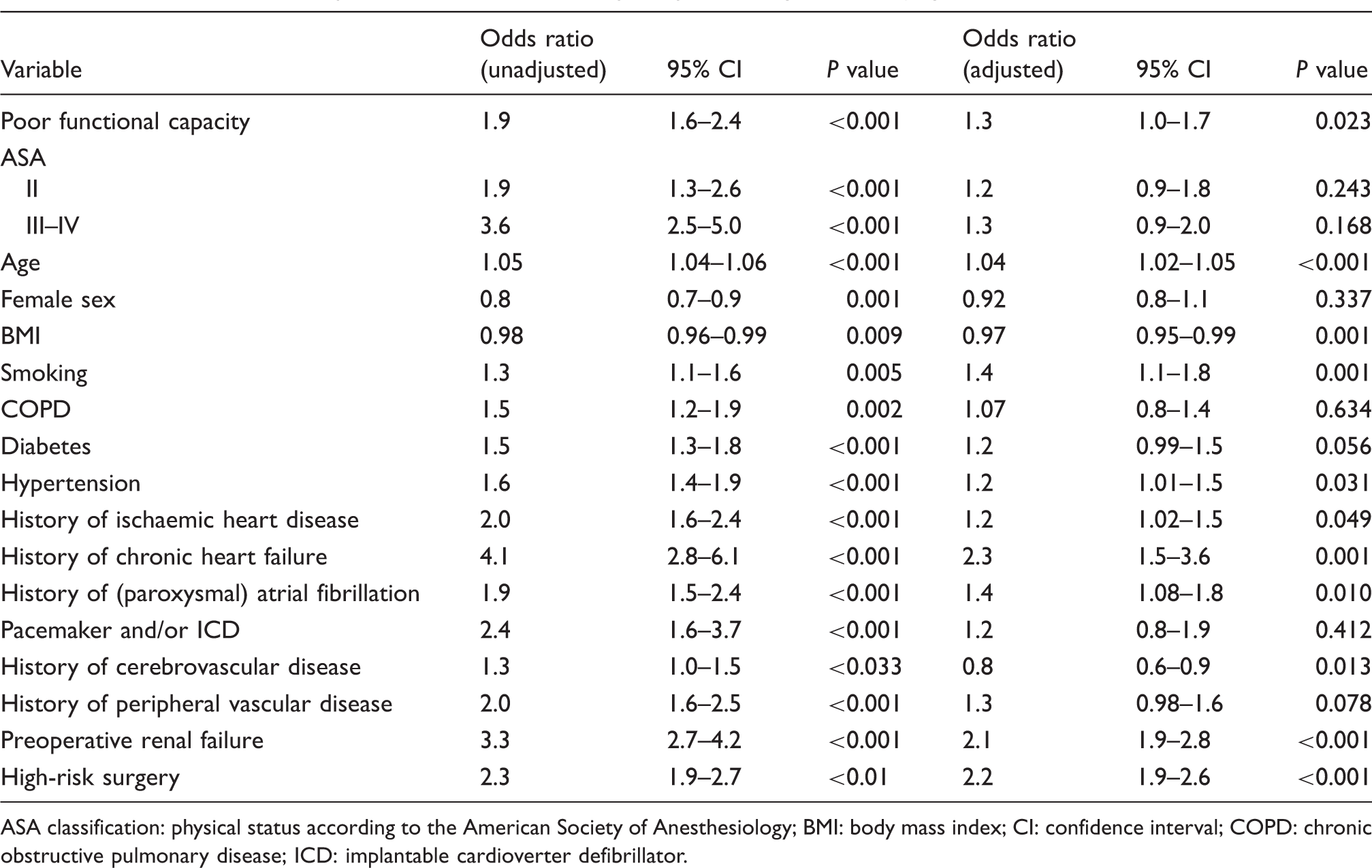
ASA classification: physical status according to the American Society of Anesthesiology; BMI: body mass index; CI: confidence interval; COPD: chronic obstructive pulmonary disease; ICD: implantable cardioverter defibrillator.
The post hoc sensitivity analysis including complete cases only yielded similar results.
Secondary outcomes
Association between patient characteristics and postoperative myocardial infarction.
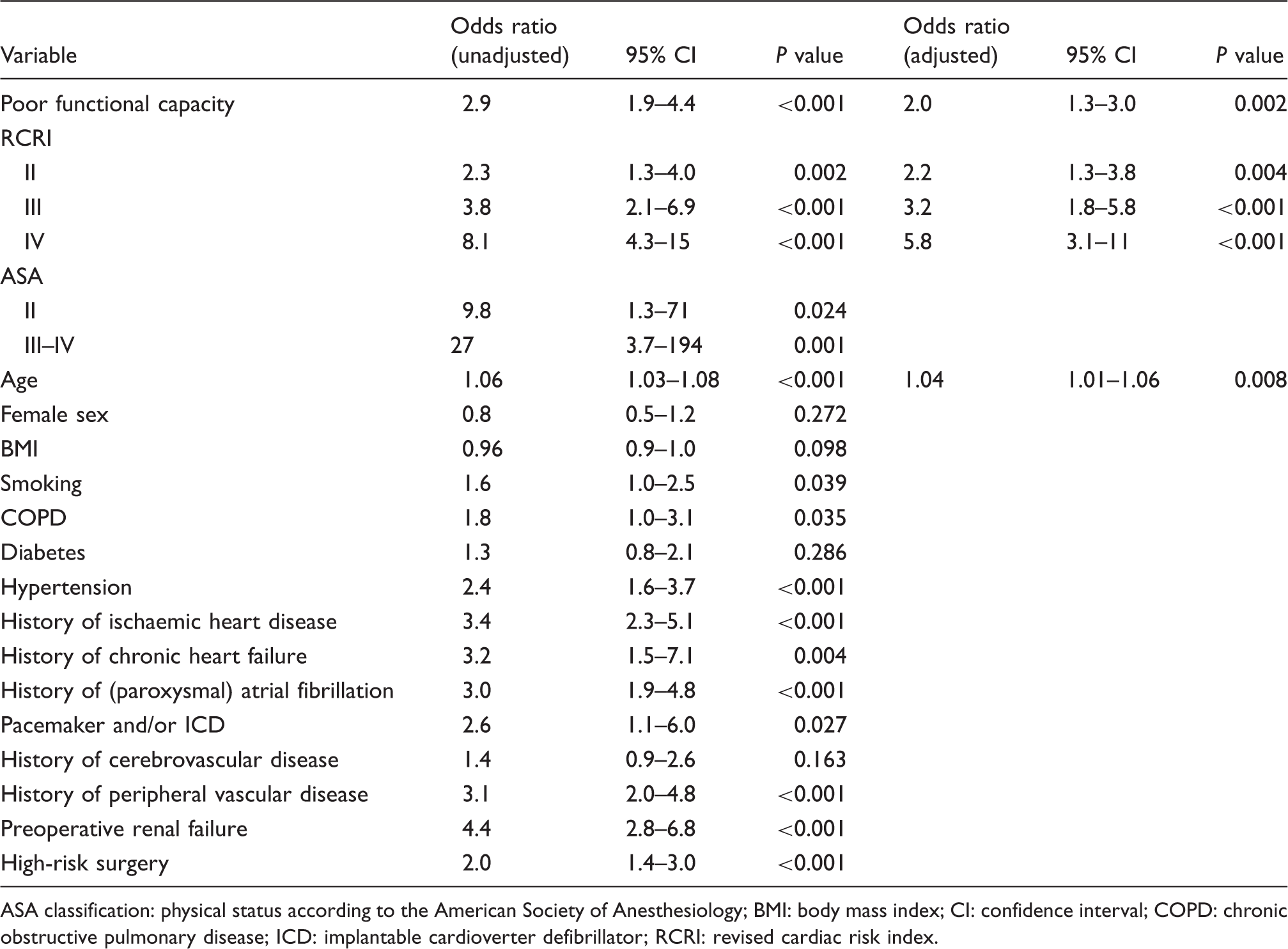
ASA classification: physical status according to the American Society of Anesthesiology; BMI: body mass index; CI: confidence interval; COPD: chronic obstructive pulmonary disease; ICD: implantable cardioverter defibrillator; RCRI: revised cardiac risk index.
Association between patient characteristics and one year mortality.
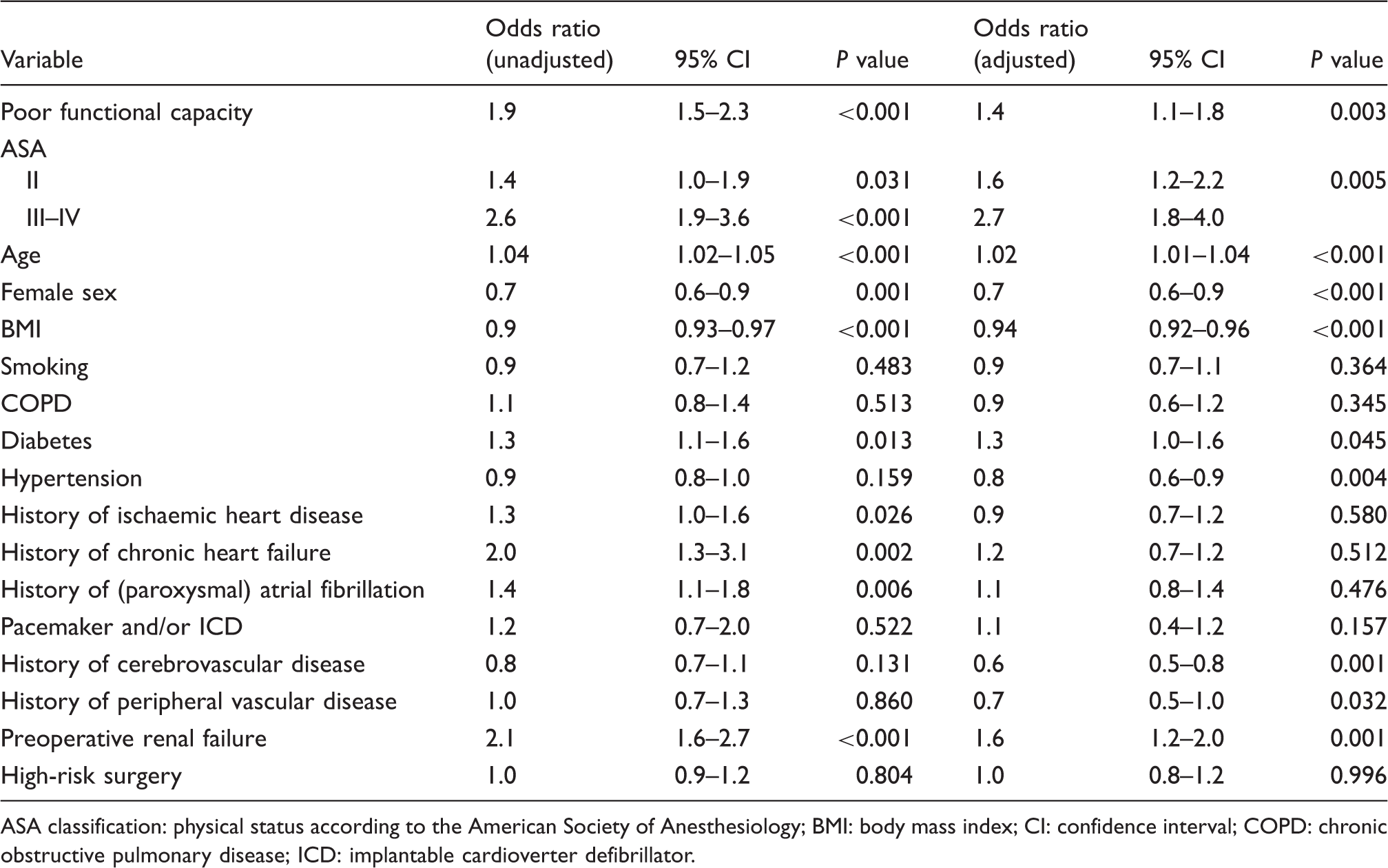
ASA classification: physical status according to the American Society of Anesthesiology; BMI: body mass index; CI: confidence interval; COPD: chronic obstructive pulmonary disease; ICD: implantable cardioverter defibrillator.
The predictive value of the multivariable model for mortality (consisting of the variables age, sex, BMI, ASA classification, comorbidities and high-risk surgery) had an AUROC of 0.65. Adding functional capacity to this model did not change the predictive value (0.65).
The post hoc analysis in patients without missing data again showed comparable results for all these outcomes.
With regard to the self-reported functional capacity, 690 patients (14%) did not report their functional capacity. Of the 4189 patients who did report, 1469 patients (35%) reported no limitations. The 2720 patients with self-reported limitations stated that this was most often due to nerve/joint/muscular problems (N = 393, 14%), low endurance (N = 404, 15%), fatigue (N = 262, 10%), or multiple reasons (N = 1469, 50%). When comparing patients’ and physicians’ estimations in the 4189 patients with self-reported functional capacity, we found a discrepancy in 2134 patients (51%). Fifty patients (1%) who self-reported having ‘no limitations’, were classified by the physician as having poor functional capacity, and 2084 (50%) patients who self-reported having limitations were classified by the physician as having normal functional capacity. Functional capacity was estimated by both patient and physician as poor in 636 patients (15%) and as normal in 1419 patients (34%).
Discussion
In this cohort study including older patients undergoing elective non-cardiac surgery, subjective estimation of functional capacity before surgery was significantly associated with postoperative myocardial injury, POMI and mortality. Patients assessed as having poor functional capacity had a slightly increased risk of postoperative myocardial injury (OR 1.3), POMI (OR 1.7) and death (OR 1.4). However, in predicting these events such subjective assessment had no added value on top of other preoperative predictors.
The literature
Several other studies investigated the relationship between subjectively assessed functional capacity and postoperative (cardiac) complications, with conflicting results.
Reilly and colleagues found that self-reported poor functional capacity was an independent predictor of cardiac ischaemia and cardiovascular complications on top of other patient characteristics, including age, in patients undergoing major surgery. 4 A study by Shah and colleagues in patients with pulmonary hypertension also showed that a patient’s self-reported poor functional capacity was associated with longer lengths of hospital stay and major complications. 15 However, in those studies the added value of functional capacity was not determined, nor were troponin levels monitored.
The added value on top of other known information was determined in a study by Wiklund and colleagues in 5939 patients undergoing elective non-cardiac surgery. 5 The authors found that subjective assessment of functional capacity predicted postoperative cardiac complications in univariable analysis, but that it had no added predictive value on top of age and ASA classification, which is in accordance with our study. 5 The METS study, a recent cohort study in 1401 patients undergoing major non-cardiac surgery, showed no added predictive value of the physician’s subjective assessment of functional capacity on patient outcomes, including myocardial injury, 30 day mortality and one year mortality. 17
The lack of an additive effect of subjectively assessed functional capacity may be explained by the physicians’ inability to estimate functional capacity correctly based on anamnesis and short clinical observation. This was also observed in the METS study; only 15% of patients with a low DASI were correctly assessed by physicians as having low functional capacity. However, in patients with higher DASI scores, 97% of the physicians estimated them as having moderate to good exercise capacity. 22 The DASI questionnaire is a more objective measure of functional capacity and an easier and cheaper method of estimating functional capacity as compared to CPET testing.8–12,16,23–25 In the METS study, the DASI was significantly associated with myocardial injury and death after adjustment for other variables. 17
Another test to determine functional capacity more objectively is the six-minute walk test (6MWT). Several studies have determined the relation between the 6MWT and postoperative (cardiac) complications and mortality.23,26–28 Those studies showed conflicting results but overall no good relation between the 6MWT and postoperative complications. 25 However, some more recent studies showed a good relation between a low 6MWT and cardiopulmonary complications.26,27 Finally, a recent study by Shulman and colleagues in patients undergoing major surgery showed that the 6MWT was predictive of death and myocardial infarction. 28
Gait speed is another test for functional capacity and is used in elderly patients in the assessment of frailty. 29 There is a relation between low gait speed and increased mortality in elderly patients undergoing cardiac surgery.30,31 In a study by Kamiya and colleagues gait speed was comparable to the 6MWT in a subgroup of patients undergoing cardiac surgery. 31 No studies have compared gait speed with 6MWT with regard to myocardial injury and mortality in patients undergoing non-cardiac surgery.
Strengths and weaknesses
A major strength of our study is the routine postoperative assessment of myocardial injury by troponin measurements, which makes it unlikely that early postoperative cardiac events were missed. Although this clinical protocol was not always followed as troponin was not measured in 10% of the patients, these missing data were likely to be random as reported previously in a part of this cohort. 19 This study also has some weaknesses. First, data on functional capacity were missing in 7% of patients. However, these data were imputed because these were likely not to be missing at random, and we also performed a post hoc complete case analysis that did not change the results. Second, because CPET was not performed, we could not determine whether the subjectively estimated functional capacity correlated to the actual functional capacity. Finally, as the assessment of functional capacity was not standardised, this may have varied between individual physicians, which may have influenced the results. However, this variation in assessments also reflects daily practice.
Clinical implications and addition of knowledge
Few aforementioned studies determined the added value of functional capacity tests. Our study, including a large number of patients, confirmed the results from the METS study and adds new insight on the additive effect of subjective functional capacity on other preoperative predictors. 17
Future directions
Given the findings from those studies it could be considered to use more objective tools to assess preoperative functional capacity, such as the DASI or other structured questionnaires. Currently, the MET REPAIR study is recruiting patients to assess the value of preoperative functional capacity as assessed by a structured questionnaire in predicting (cardiac) complications and death. 32 It is of interest whether this has any added value on top of other preoperative variables to predict cardiac complications. In the light of limited (human) resources in medicine, questionnaires such as the DASI and more objective tools to estimate functional capacity such as the 6MWT and gait speed should only be used if they have any additive value, because although these are simple to perform they still cost time and manpower.
Conclusion
In patients undergoing non-cardiac surgery, subjectively assessed preoperative functional capacity was a predictor of postoperative myocardial injury, infarction and death, but had no added value on top of other preoperative predictors.
Supplemental Material
CPR906918 Supplemental Material - Supplemental material for Added value of subjective assessed functional capacity before non-cardiac surgery in predicting postoperative myocardial injury
Supplemental material, CPR906918 Supplemental Material for Added value of subjective assessed functional capacity before non-cardiac surgery in predicting postoperative myocardial injury by Marije Marsman, Judith AR van Waes, Remco B Grobben, Corien SA Weersink and Wilton A van Klei: on the behalf of the JROAD Investigators in European Journal of Preventive Cardiology
Footnotes
Author contributions
JARW, WAK and MM contributed to the conception or design of the work. MM drafted the manuscript. All authors contributed to the acquisition, analysis or interpretation of data to the work and revised the manuscript critically and gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by a grant from the International Anesthesia Research Society (clinical scholar research award 2011 to WAK); and by a grant from the Friends of the University Medical Center Utrecht foundation/the Dirkzwager–Assink Fund to WAK.
Previous work
A part of the raw data collected in this study was used in a previous study:
Van Waes JA, Grobben RB, Nathoe HM, et al. One-year mortality, causes of death, and cardiac interventions in patients with postoperative myocardial injury. Anesth Analg 2016; 123: 29–37.
Van Waes JA, Nathoe HM, de Graaff JC, et al. Myocardial injury after noncardiac surgery and its association with short-term mortality. Circulation 2013; 127: 2264–2271.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.