
Abstract

The current global obesity epidemic has contributed to an increased prevalence of atrial fibrillation (AF). 1 Although lifestyle modifications represent the mainstay of obesity therapy, recent guidelines acknowledge they are often unsuccessful for long-term prevention of cardiovascular morbidity and mortality. 2 The relationship between AF and obesity is of great clinical interest, with weight loss following bariatric surgery (BS) having been associated with a lower incidence of AF. 3 This study aims to investigate the impact of BS on the long-term incidence and resolution of AF using the Clinical Practice Research Datalink (CPRD), a national primary and secondary healthcare database of over 11 million patients. 4
Baseline demographic, clinical and treatment characteristics of the patients by bariatric surgery status.

BMI: body mass index; ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blocker.
Average follow-up length was 148 months (standard deviation (SD) 80 months). Across both cohorts the mean age was 50.4 years, 22.7% of patients were men, and median BMI was 43.30 kg/m2. The BS group had a slightly less favourable baseline risk factor profile, with higher rates of hypertension (P = 0.003) and diabetes (P < 0.001) but similar rates of hyperlipidemia, smoking, renal failure, alcohol intake and exercise. In addition, the BS group received higher rates of medical treatment during follow-up, with greater numbers of patients prescribed angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (P = 0.036), statins (P < 0.001) and fibrates (P = 0.036). The BS group displayed significantly greater weight loss during follow-up (–0.09 vs. + 4.03; P < 0.001). Patient demographic, clinical and treatment characteristics are outlined in Table 1.
The primary endpoint of new-onset AF occurred in 149 patients; 65 in the BS group and 84 in controls (adjusted hazard ratio (HR) 0.720, 95% confidence interval (CI) 0.492–1.054; P = 0.091), depicted in Figure 1(a). The secondary endpoint of AF resolution occurred more commonly in the BS group compared with controls (17 vs. 9; P = 0.049), depicted in Figure 1(b). New AF rates were similar across all BS types; gastric bypass (2.2%), gastric banding (2.7%) and sleeve gastrectomy (2.0%) (P = 0.238). Weight loss during follow-up was similar regardless of whether AF was experienced or not (–2.37 (22.75) kg vs. –2.52 (21.23) kg; P = 0.158).
Incidence and resolution of new-onset atrial fibrillation (AF) following bariatric surgery (BS) compared with controls. (a) Cumulative hazard of incident AF in BS and controls. (b) Cumulative AF resolution rates in BS and controls.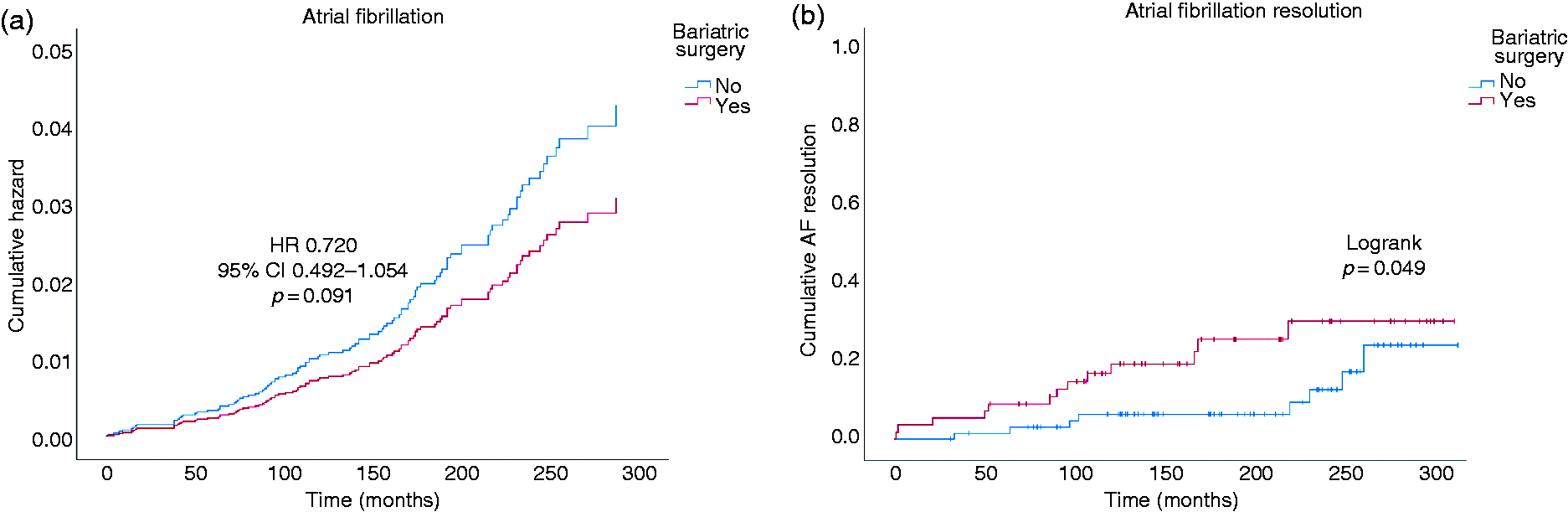
The results of this nationwide retrospective cohort study reveal an association between BS and increased rates of AF resolution; and describe a non-significant trend towards a lower incidence of new-onset AF. The mean follow-up length of 12.3 years represents one of the longest term follow-up times among similar published research.
A link between BS and lower AF incidence has been found in previous studies. 2 The present study did not corroborate this, although a strong but non-significant trend was observed. In light of the biological plausibility of the effect taken together with previous literature, the authors recognise that the absence of significant association may be related to low overall event rates – with only 65 BS patients and 84 controls developing new-onset AF.
The role of weight loss on the long-term outcomes of AF is a current topic of debate. Previously, Mohanty et al. 5 did not show a benefit of weight loss prior to ablation, with Donnellan et al. 6 conversely showing that prior weight loss improved AF resolution post-ablation. Importantly, the patient populations in both aforementioned studies were significantly older than our relatively young cohort, and therefore may have had a more pronounced and sustained electrophysiological AF substrate. Unfortunately, the lack of granularity regarding tertiary care-level management of AF in the CPRD precludes its utilisation to address a similar question, and we were thus unable to assess ablation outcomes or the impact of AF substrate in this cohort.
BS positively impacts various cardiovascular risk factors, with reduced blood pressure, inflammatory markers and triglycerides, alongside improved glycaemic control and increased high-density lipoprotein cholesterol reported.7,8 In addition to metabolic changes, alterations in the gut endocrine milieu may explain some of these benefits. Unfortunately, due to the lack of laboratory data available in the CPRD, we were unable to explore whether similar associations exist in our cohort. Similarly, we could not address the effect of BS on nutritional deficiencies that may conversely predispose to AF.
Because of the retrospective nature of this study, it is possible the observed trend is influenced by greater awareness and earlier diagnosis of risk factors for AF in the BS group, resulting in concordantly higher rates of medical treatment. Furthermore, the BS group had an evidently worse baseline risk factor profile. This limitation may conceivably have introduced residual confounding, despite stratification for age, gender and BMI and post-hoc adjustment of analyses. Finally, due to the Read code-based recording system that the CPRD utilises, it was not possible to establish the exact method of diagnosis of AF (i.e. bedside ECG, 24-hour ECG, loop recorder, etc.). Therefore, prospective studies are essential to clarify the associations between BS and the incidence and resolution of AF.
In summary, this study demonstrates a higher rate of AF resolution among patients with obesity who underwent BS when compared with gender, age and BMI-matched controls. Furthermore, it identifies that BS may be associated with a trend towards lower AF incidence. In light of the rapidly progressive growth in obesity rates worldwide, this sheds light on the role of a potentially important, and often overlooked, cornerstone of preventive therapy for patients with obesity and AF.
Footnotes
Author contribution
MA, CE, PC and SP contributed to the conception or design of the work. OM, RKR, PZ, OK and AD contributed to the acquisition, analysis, or interpretation of data for the work. MA and CE drafted the manuscript. OM, RKR, PZ, OK, AD, PC and SP critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgements
Data access was provided by the Big Data & Analytical Unit (BDAU) at the Institute of Global Health Innovation (IGHI), Imperial College London, London, UK. Infrastructure support for this research was provided by the NIHR Imperial Biomedical Research Centre (BRC), Imperial College London, London, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Scientific approval was granted for the study by the regulatory agency’s independent scientific advisory committee; and ethical approval was granted by the Health Research Authority IRAS. Project ID: 203143. ISAC approval registration number: 16_140R2.
Funding
The author(s) received no financial support for research, authorship, and/or publication of this article.