
Abstract
Aims
The study evaluated the quality of cardiovascular prevention in real-world clinical practice. The recurrence of up to five cardiovascular events was assessed, as data on recurrence beyond the first event and interindividual variations in event rates past the second event have been sparse. Low-density lipoprotein cholesterol concentrations and lipid-lowering therapy use were investigated.
Methods
This retrospective register-based study included adult patients with an incident cardiovascular event between 2004 and 2016 treated in the hospital district of southwest Finland. Patients were followed for consecutive cardiovascular events or cardiovascular death, low-density lipoprotein cholesterol and statin purchases. The timing of event recurrence was evaluated, and predictive factors were assessed.
Results
A wide interindividual variation in cardiovascular event recurrence was observed, each additional event caused an increased risk, the median time of recurrence decreased from 7 to one year for the second and fifth event. Event rates increased correspondingly from 12 to 43/100 patient-years and were most pronounced in the first years following the previous event. The low-density lipoprotein cholesterol goal (<1.8 mmol/l) was reached by 18% in the year after the event and statin underuse was associated with an increased risk of recurrence. Six months after the index event high intensity statins were used by only 22% of the cohort.
Conclusion
The study provides new perspectives on individual risk assessment showing that event rates are not stable for all patients but increase 1.2–1.9-fold per consecutive event. The underuse of statins and poor adherence support the identification of these patients for intensified multifactorial preventive measures.
Introduction
Cardiovascular mortality and morbidity are large public health issues both in Europe and worldwide, although cardiovascular events have decreased and outcomes have improved in past decades.1–4 In particular, improved post-event survival makes it important to understand which patients are at high risk of recurrence.5,6
Elevated low-density lipoprotein (LDL) cholesterol concentration is a key risk factor of cardiovascular events. The positive effects of lowering LDL-cholesterol, on reducing new events and mortality are well established. Analyses of large clinical trials on intensive statin use show that a 1 mmol/l LDL-cholesterol reduction is associated with a 15–20% reduction of recurring major cardiovascular events.7,8 Current guidelines highlight the importance of achieving the largest LDL-cholesterol reduction possible, recommending both a minimum percentage LDL-cholesterol reduction (50%) and an absolute LDL-cholesterol treatment goal of less than 1.4 mmol/L (<55 mg/dL) for very high risk patients, and less than 1.8 mmol/L (<70 mg/dL) for high risk patients.5,6,9
Most published clinical studies observe event rates and outcomes associated with the first cardiovascular event during cardiovascular prevention, providing only limited information on event rates beyond the first recurrence. Even then, the focus has been on event rates and subsequent event types, mainly lacking LDL-cholesterol and statin intensity changes during follow-up.10–12 Common limitations of clinical trials are their limited representativeness and generalisability on unselected patient populations. In contrast, population-based studies can provide a better description of the relationship between recurring events and predisposing factors, such as patient behaviour regarding lipid-lowering medication use.
The aim of this population-based study was to investigate patients with multiple cardiovascular events, to determine the risk of recurrence and the relationship between previously well-established predictive factors beyond the first event. Furthermore, the timing of consecutive cardiovascular events, statin intensities and the proportion of patients reaching LDL-cholesterol concentration goals during cardiovascular prevention were assessed.
Methods
Patients (N = 28,625) with their first (index) cardiovascular event in the years 2004–2016 in the hospital district of southwest Finland (HDSWF) were included in this retrospective register-based study, reflecting everyday clinical practice. Definition of the index event was based on the International Classification of Diseases 10th version (ICD-10) codes of myocardial infarction (MI), unstable angina pectoris (UAP), ischaemic stroke (IS), transient ischaemic attack (TIA), ruptured aneurysm of the abdominal aorta, and procedure codes of coronary angioplasty, coronary bypass surgery, peripheral (lower limb) angioplasty and non-traumatic amputation (for diagnosis and procedure codes see Appendix 1). Data from 1996 to 2003 were used to exclude patients with earlier cardiovascular events. All the same types of cardiovascular events were collected from the electronic medical records until the end of follow-up or death, but also cardiovascular death was included (ICD-10 diagnosis codes I20–I79 as the main or immediate cause of death).
To differentiate consecutive cardiovascular events from each other, it was required that the diagnosis was made at the emergency room and/or by imaging. A minimum time interval of 7 days was required for an event to be classified as a new event. For coronary angioplasty and bypass, procedures were required to be more than 60 days apart from the previous event. For diagnosis of MI an elevated troponin-T (TnT) concentration was required, for unstable angina typical symptoms and normal TnT. The clinical thresholds of TnT had changed during the study period and corresponding cut-offs were used.
Data in the specialty care electronic patient register included diagnosis codes, healthcare visits, procedures, operations and laboratory values (permission number J16/17). The cohort was further linked to the national registries for causes of deaths from Statistics Finland, and the Social Insurance Institution for drug purchases of lipid medication (ATC statins C10AA01-08), diabetes medication (A10*) and blood pressure medication (angiotensin-converting enzyme inhibitors (ACEis) C09A, C09B; angiotensin receptor blockers (ARBs) C09C, C09D; renin inhibitors C09X). For comorbidity assessment at index, diagnosis codes and medications were assessed from the time period before the index. Diabetes was defined by ICD-10 codes (E10, E11, E12, E13, E14) or any purchase of ATC class A10* medicines; hypertension was defined as I10* or ACEi, ARB, renin inhibitor medication; chronic kidney disease (CKD) was defined as N18, Z49 or estimated glomerular filtration rate (eGFR) of less than 60 ml/min/1.73 m2, calculated from closest available serum creatinine value ± 3 months from index event.
Statin intensity
For each patient, the average statin use, during a sliding window of up to three consecutive purchases, was defined (total DDD purchased/window length). Statin intensity was defined as low (corresponding to simvastatin 7.5–15 mg/day), moderate (simvastatin > 15 mg/day), or high (atorvastatin >30 mg/day) with modified criteria from the American College of Cardiology (ACC)/American Heart Association (AHA) guideline on treatment of blood cholesterol 13 (see Appendix 2). Patients could further be grouped by purchase data to below low intensity use (i.e. irregular purchases resulting in statin intensity corresponding to simvastatin below 7.5 mg/day), or unmedicated if no purchases were recorded. The pre and post-index purchases were handled separately.
LDL-cholesterol concentrations
All LDL-cholesterol concentrations for each patient were used and treated with carry-forward imputation (i.e. LDL-cholesterol considered unchanged until new measurement) for analyses of changes in LDL-cholesterol during follow-up. The proportion of patients reaching different LDL-cholesterol goals (<1.8, 1.8–2.6, 2.6–3.0 and >3.0 mmol/l) after the index event were described at different time points up to 3 years after the event. Due to timing of the actual analysis the 2016 European Society of Cardiology (ESC) guidelines were used for classification of LDL-cholesterol goals. 5
Statistical analysis
The timing of consecutive events was described in time-to-event analyses by Kaplan–Meier estimates. The time to event was defined as the time from one cardiovascular event to the next, or cardiovascular death. Censoring events were non-cardiovascular deaths and end of follow-up. Factors affecting recurrent events were assessed with the Prentice, Williams and Peterson (PWP) recurrent event model using gap time (GT) and total time (TT). 14 As GT and TT models did not differ notably, GT results are presented. GT assesses the time between events, in which the time index is reset to zero after each recurrence. Predictors were assessed both in univariate and multivariable analyses. Index data regarding comorbidities, age and sex were included, statin intensities and an absolute change in LDL-cholesterol concentrations, with respect to the index value, were included as time varying covariable in the analyses.
Results
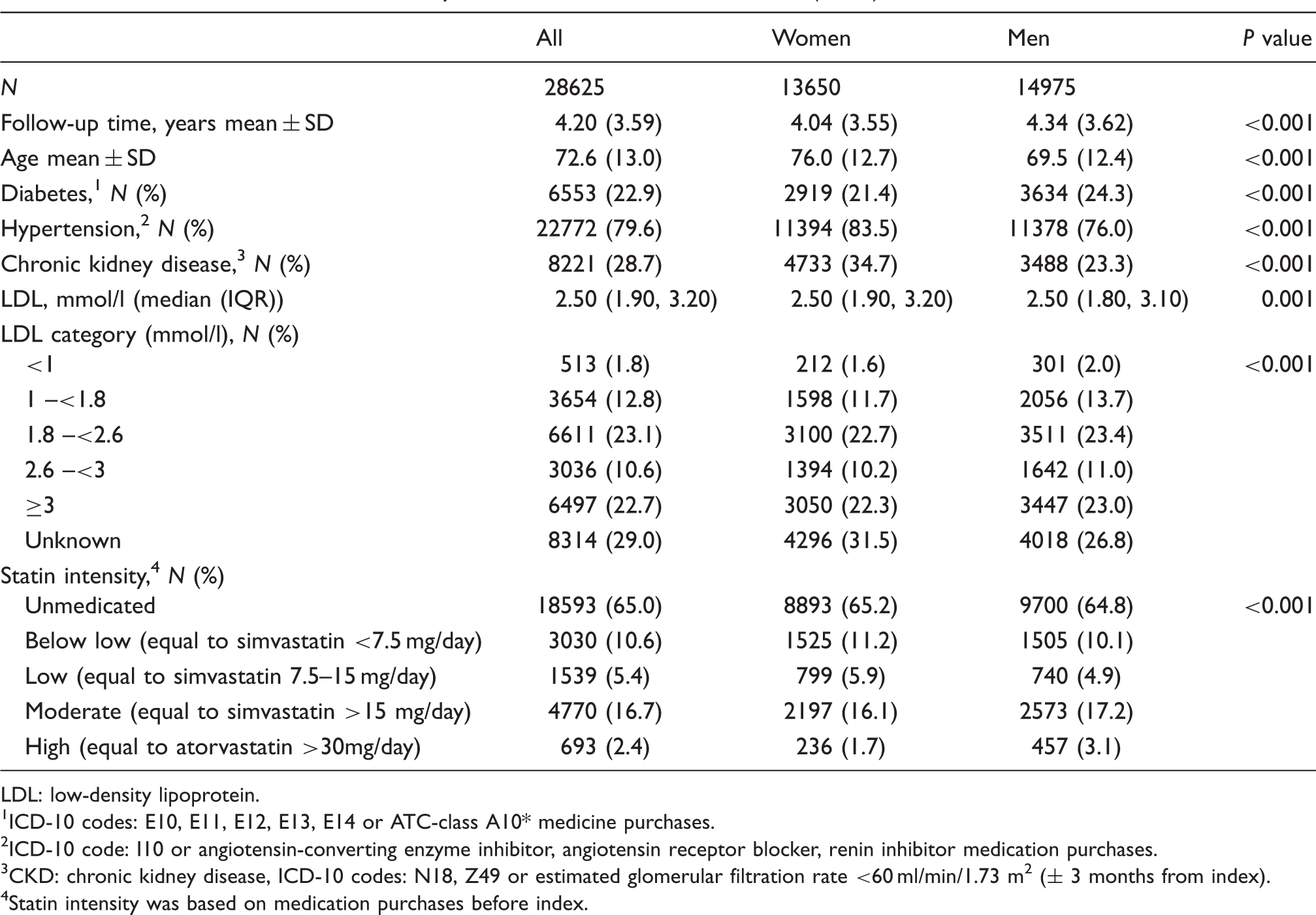
During the years 2004–2016, 28,625 patients had an incident (index) cardiovascular event and were followed for consecutive cardiovascular events (Figure 1). Characteristics of the cohort at the time of the index cardiovascular event are presented in Table 1. The mean age was 72.6 ± 12.9 years, and 52% were men. Female patients were on average 7 years older than men at the time of the incident event. Diabetes was evident in 23% of patients and hypertension in 80%. At the time of the index cardiovascular event, 65% of patients had no statin medication use and 11% were infrequent users based on purchase data (Table 1).
Timing of recurrent cardiovascular events (second to fifth) during cardiovascular prevention. Time to second event (a); time to third event (b); fourth event (c); fifth event (d). The median time and 95% confidence interval (CI) between consecutive events are presented in the top right corner of each graph. X axis: time in years; Y axis: survival probability. Patient characteristics of the study cohort at the time of the incident (index) cardiovascular event. LDL: low-density lipoprotein.
1
ICD-10 codes: E10, E11, E12, E13, E14 or ATC-class A10* medicine purchases.
2
ICD-10 code: I10 or angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, renin inhibitor medication purchases.
3
CKD: chronic kidney disease, ICD-10 codes: N18, Z49 or estimated glomerular filtration rate <60 ml/min/1.73 m2 (± 3 months from index).
4
Statin intensity was based on medication purchases before index.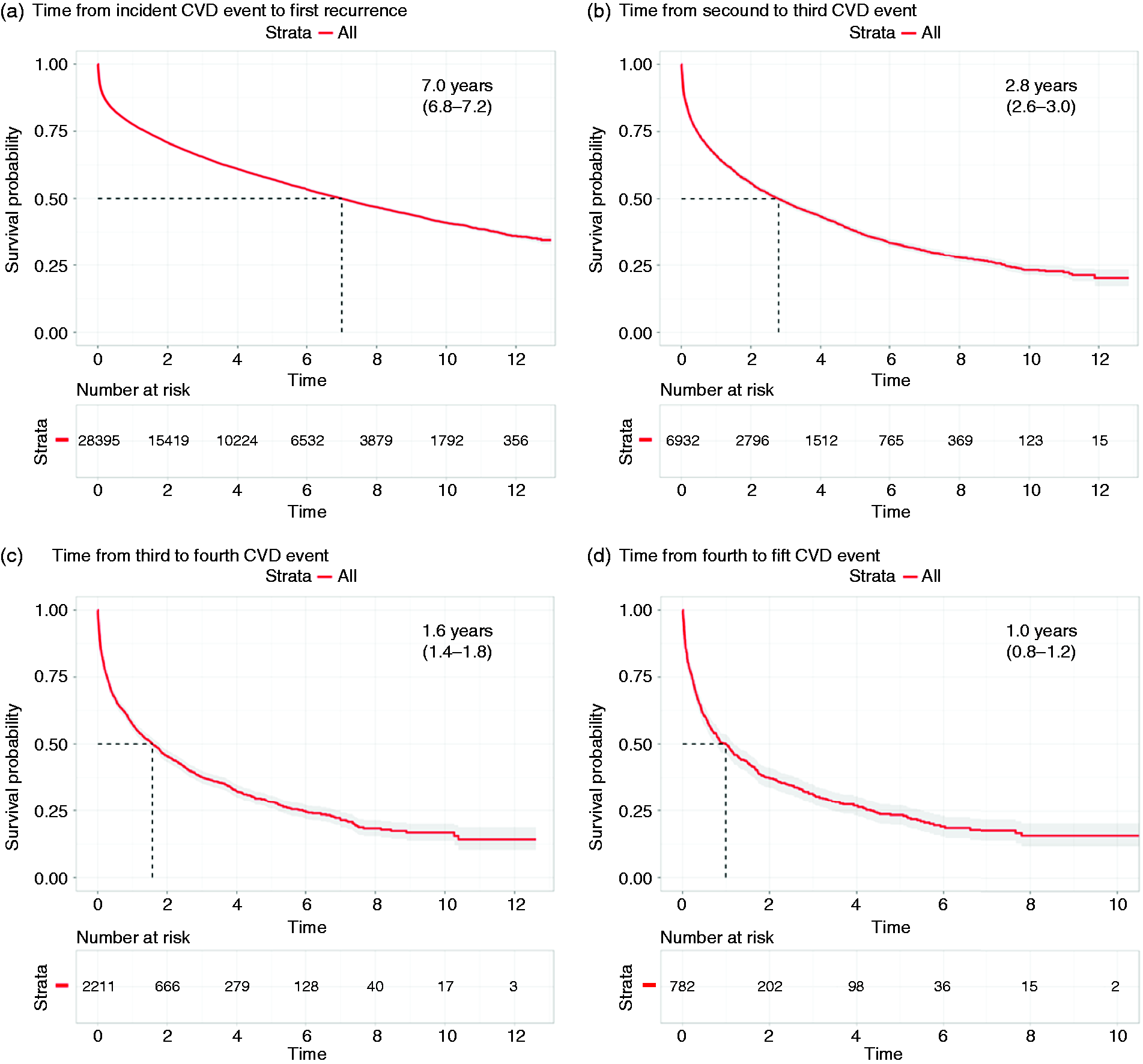
The median time between each consecutive event decreased from 7.0 years (95% confidence interval (CI) 6.8–7.2) for the second event, to 2.8 (2.6–3.0), 1.6 (1.4–1.8) and 1.0 (0.8–1.2) years for the third, fourth and fifth events (Figure 1). Thus, event rates increased from 12.0 events/100 patient-years for the second event to 23.2 events/100 patient-years for the third event, and 35 and 43 events/100 patient years for the fourth and fifth event, respectively (Figure 2).
Overview of cardiovascular events in the study cohort stratified by event number. The median time to next event is shown above horizontal arrows (median, 95% confidence interval (CI)), and the number at risk of a consecutive event below the arrow. Below each consecutive event, the proportion of outcomes are presented. *Cardiac: myocardial infarction, coronary angioplasty, coronary by-pass; IS: ischaemic stroke; OTHER: peripheral angioplasty of lower limbs, non-traumatic amputation of part of lower limb, ruptured aneurysm of abdominal aorta; TIA: transient ischaemic attack. Event rate is per 100 patient-years.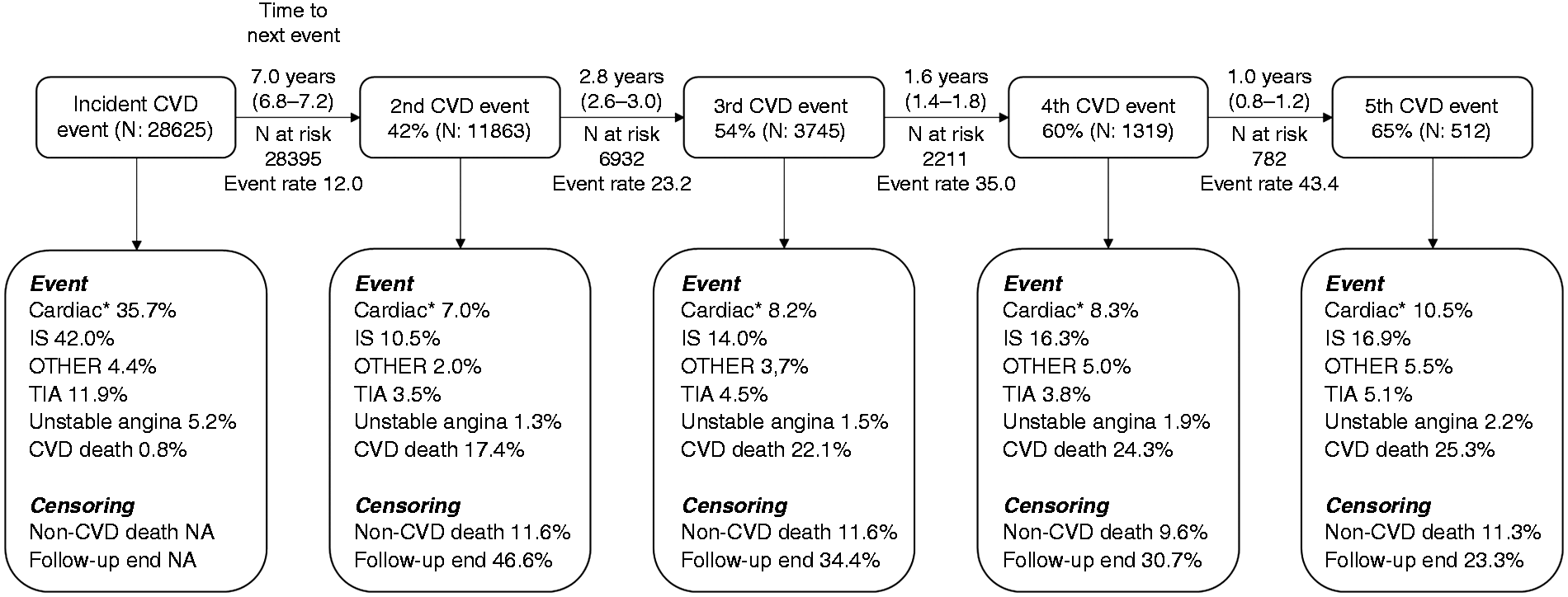
The most common index event types were ischaemic stroke (42%) and cardiac events (35.7% MI, coronary bypass surgery, coronary angioplasty, Figure 2). There were differences in index event types between sexes, with women presenting more often with ischaemic stroke and men with cardiac events (see Appendix 3). During the mean cardiovascular prevention period of 4.2 years 42% of patients had at least one additional cardiovascular event including cardiovascular death. Up to five separate events were recorded in 512 individual patients (1.8% of the total cohort). Independent of the event number, cardiovascular mortality was the most common event type (Figure 2).
Recurrent event analysis of factors associated with recurrent cardiovascular events. PWP model with gap time.
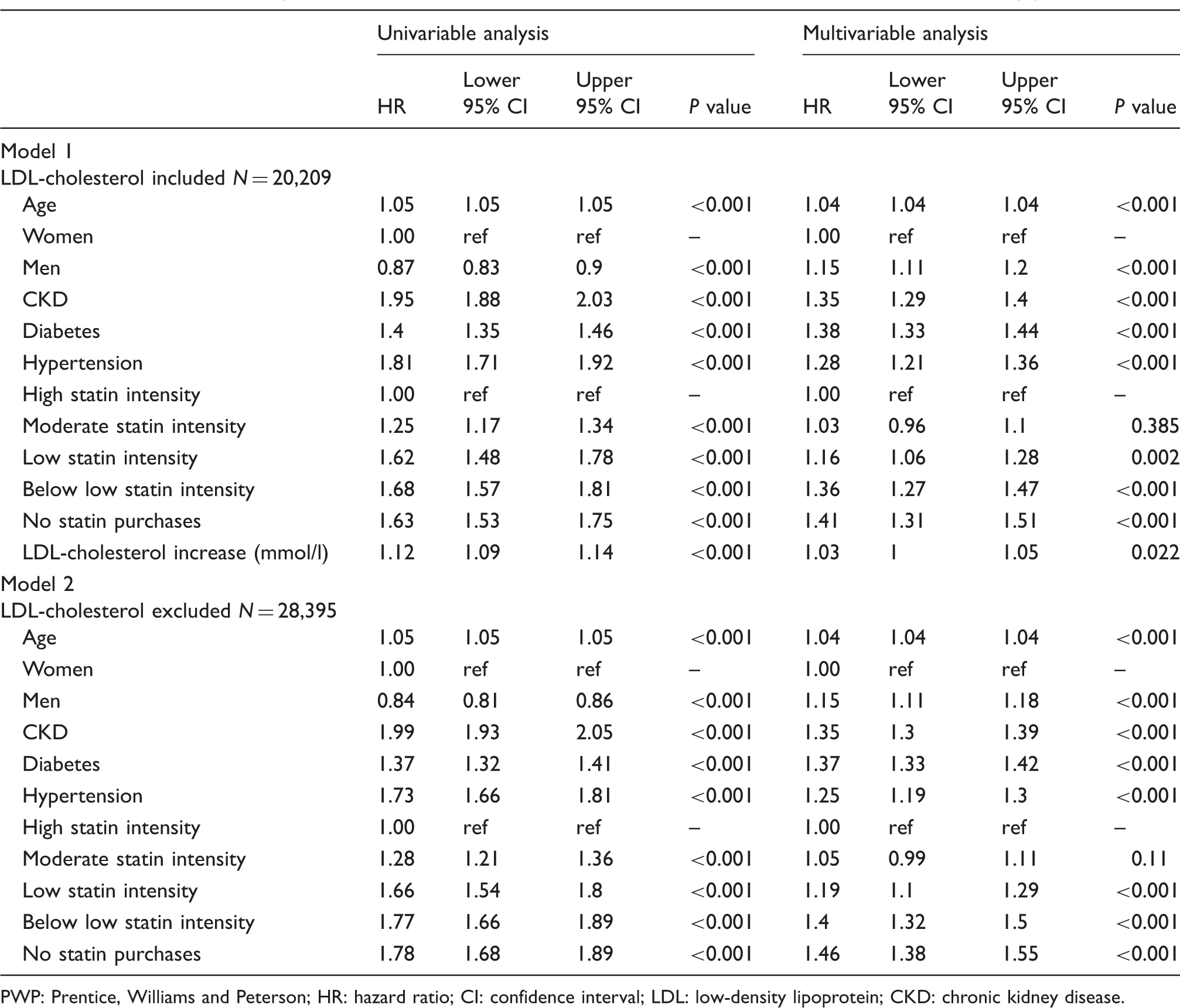
PWP: Prentice, Williams and Peterson; HR: hazard ratio; CI: confidence interval; LDL: low-density lipoprotein; CKD: chronic kidney disease.
The further analyses focused on describing statin intensities and LDL-cholesterol concentrations during cardiovascular prevention. Statin intensities, according to purchase data, before and after the index event are presented in Figure 3. High intensity statin use reached a peak at 6 months after the index event; however, there was a decrease in purchases at high and moderate intensity after that, with infrequent users increasing over time. Notably, in patients alive at 2.7 years (1000 days) after the index event, 25% of the cohort had never purchased any statins (Figure 3). The proportions were 13% for cardiac events (MI, coronary bypass surgery, angioplasty) and 32% for IS; 32% for TIA; 22% for UAP; and 41% for other events (peripheral angioplasty, non-traumatic amputation of part of lower limb, ruptured aneurysm of abdominal aorta).
Proportion of patients using different statin intensities before and after the incident (index = 0) cardiovascular event. Time is in days.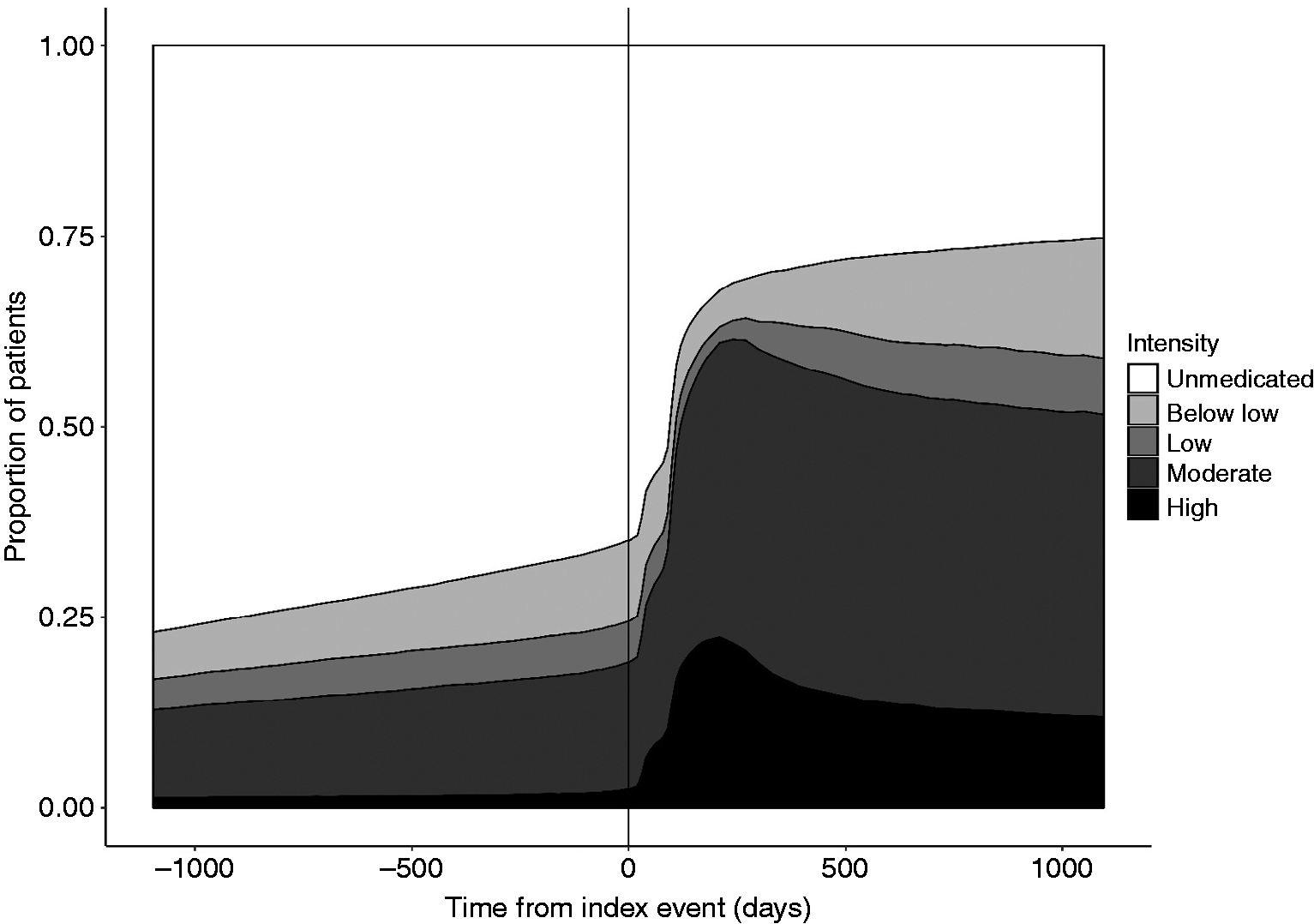
The proportion of patients in cardiovascular prevention reaching LDL-cholesterol concentrations below 1.8 mmol/l was 18% in the whole population and 20% in patients with a cardiac event as their index event (Figure 4). At a population level LDL-cholesterol concentration remained very stable after the index event, and the proportion of patients in the LDL-cholesterol categories virtually unaffected.
Proportion of patients reaching low-density lipoprotein (LDL) cholesterol concentration targets of 3 mmol/l or greater (white); 2.6–3 mmol/l (light grey); 1.8–2.6 mmol/l (dark grey) and less than 1.8 mmol/l (black) in the whole cohort (a); and in patients with a cardiac index event (b). Proportions before the index are presented in the bar, and during cardiovascular prevention in the right panel as a proportion of patients at risk, as a function of days from the index.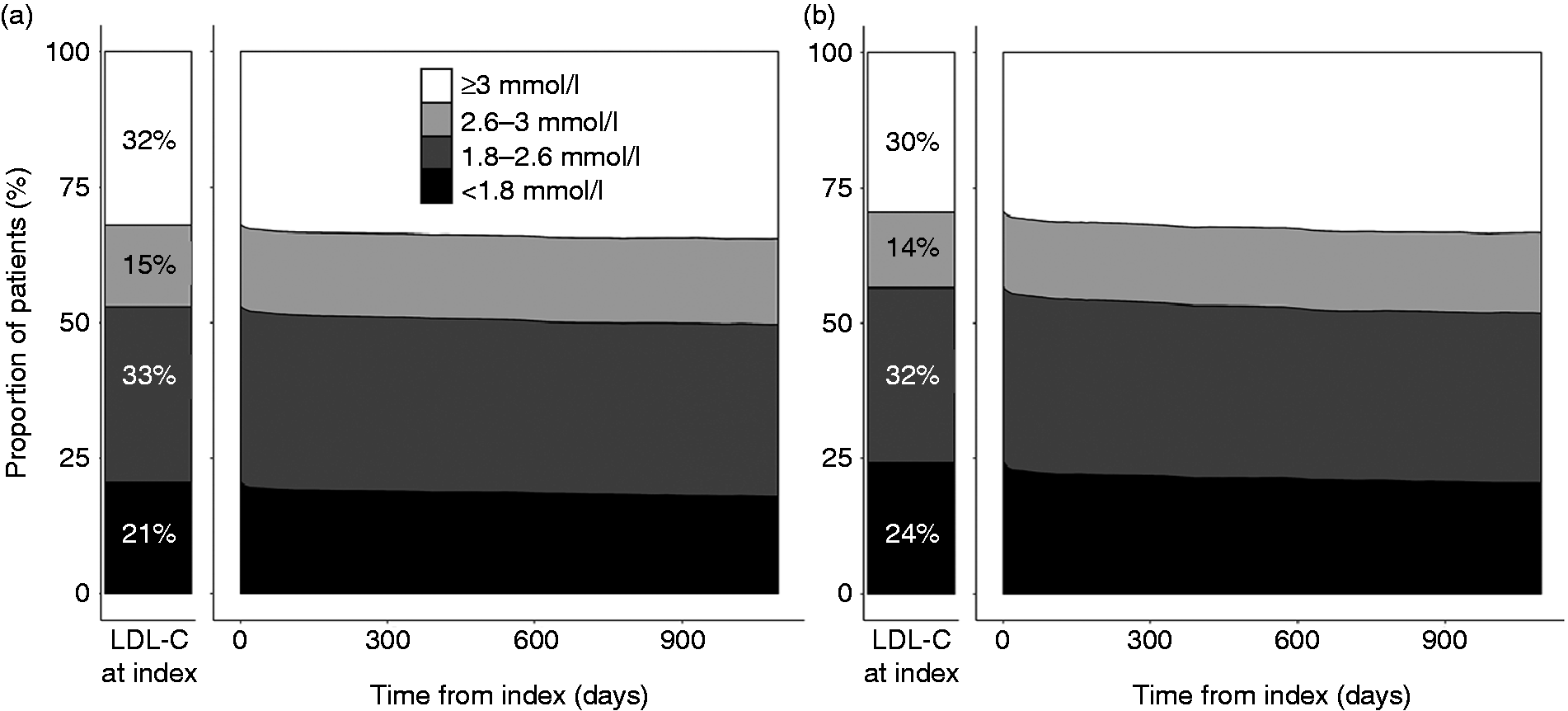
Discussion
Cardiovascular patients are generally at high risk after their first event and we show that 50% of patients were predicted to have a new event within the following 7 years. There was a wide interindividual variation in the risk, each new event increased the probability of new events; the median time between events decreased from 7 to one year for the second and fifth event. Similarly, the event rate increased from 12 to 43/100 patient-years for the corresponding events, and the recurrence rate was most pronounced within the first years following the previous event. These findings support the view that the patients with repetitive cardiovascular events should be the focus of intensified preventive measures.
Most earlier studies assessing recurrent cardiovascular risk have been relatively short and included only the second cardiovascular event as the endpoint, showing that the first year after an incident event is associated with the highest hazard rate for a consecutive event.11,12,15,16 A register-based Swedish study recently reported on an event rate of 11.9/100 patient-years for recurrent cardiac composite endpoints (MI, IS, or cardiovascular death) after incident MI, and 12.3 after IS, which is in line with our study, in which the event rate between the index and the second event was 12.0/100 patient-years. 10 However, our observations provide a new perspective in individual risk assessment, showing that the event rate is not stable for all patients but increases 1.5–1.9-fold after consecutive events.
The second main finding was the underuse of statins and poor adherence that was associated with a higher risk of future events, presenting another goal for improvement in cardiovascular preventive measures. Poor adherence has been reported in other studies,17,18 even if there are successful examples of reduced mortality associated with patient motivation and follow-up. 19 Six months after the index cardiovascular event, 22% of the overall cohort and 32% of those with a cardiac event had purchased statins corresponding to high intensity statin use, as recommended. 5 Notably, 65% of patients had no statin purchases at the time of the index event, and a quarter of the cohort never purchased statins during follow-up. In patients purchasing statins, high intensity statin use peaked at 6 months from the index but declined during the follow-up. In the multivariable analysis high intensity statin use was associated with a reduced risk of consecutive events, highlighting the importance of patient motivation and follow-up.
At a population level the proportion of patients in the different LDL-cholesterol categories remained stable after the first event, with 18% of all patients meeting the recommended LDL-cholesterol concentration, even if interindividual variation was large and the univariate model showed a 12% risk reduction in consecutive events for a 1 mmol/l LDL-cholesterol decrease. The HR of LDL-cholesterol reduction was lower in the multivariable model. LDL-cholesterol and statin intensities have a high degree of correlation, which may explain the finding. Furthermore, LDL-cholesterol measurements were infrequent, probably leading to statin purchases predicting consecutive events more accurately. Adding LDL-cholesterol to the multivariable model decreased the patient numbers; however, the predictive factors remained the same, meaning that patients with LDL-cholesterol available are comparable regarding the assessed factors to the total cohort and not subject to selection bias due to, for example, a larger comorbidity burden. The proportion of patients reaching LDL-cholesterol less than 1.8 mmol/l is in line with a multicountry survey in which 29% of patients reached LDL-cholesterol less than 1.8 mmol/l after the first event. 20 The LDL-cholesterol outcomes underline the underuse of lipid medication and the need for improved cardiovascular preventive care to reduce recurrence risk.
This study adds to the scientific knowledge on event recurrence from a large robust dataset of cardiovascular prevention patients and their outcomes including further cardiovascular events, LDL-cholesterol concentrations and lipid-lowering therapy. There are some limitations typically associated with retrospective database analyses, and those associated with cohort selection. These include the risk that some information may not have been consistently recorded for all patients, potentially impacting on the population size and other outcomes. Moreover, the study could not assess what proportion of patients have received a statin prescription but never purchased the statins, nor were other cardiovascular preventive medications available for assessment. However, there was a clear trend that the adherence to statin medication decreased over time evidenced by an increase in the proportion of patients with infrequent statin purchases.
To conclude, we provide new insight on the cardiovascular prevention risk, demonstrating that new cardiovascular events occur at accelerated event rates. Irrespective of other risk factors, patients in cardiovascular prevention benefitted from high intensity statin use. The usage of lipid-lowering medication and cardiovascular prevention follow-up needs more attention as many patients do not reach their LDL-cholesterol goal and adherence to medication decreases over time.
Footnotes
Acknowledgement
Juha-Matti Varjonen at Auria Clinicial Informatics is acknowledged for data extraction.
Author contribution
MIL, IT, SB and MP contributed to the conception and study design, data acquisition and analysis, interpretation of results, and manuscript writing or revision. JP and KEJA contributed to data interpretation and critically revised manuscript. All authors gave final approval for manuscript submission and are accountable for all aspects of the work, ensuring integrity and accuracy of the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MIL and IT are employed by Medaffcon Oy. SB and JP are employees of Amgen. KEJA received research grants from the Finnish Foundation for Cardiovascular Research; lecture fees from Bayer, Boston Scientific, Pfizer and Novartis; is a member of the advisory boards for Bayer, Pfizer and AstraZeneca. MP received consulting fees from Boehringer Ingelheim and has been a member of advisory boards for Amgen and AstraZeneca.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Amgen, Finland.