
Abstract
Aims
Health literacy, the degree to which individuals understand and act upon health information, may have a pivotal role in the prevention of cardiovascular disease (CVD), with low health literacy potentially explaining poorer adherence to prevention guidelines. We investigated the associations between health literacy, ultrasound-detected carotid atherosclerosis and cardiovascular risk factors.
Methods
Baseline data (cross-sectional analysis) from a randomized controlled trial, integrated within the Västerbotten Intervention Program, Northern Sweden, was used. We included 3459 individuals, aged 40 or 50 years with ≥1 conventional risk factor or aged 60 years old. The participants underwent clinical examination, blood sampling, carotid ultrasound assessment of intima-media wall thickness (CIMT) and plaque formation, and answered a questionnaire on health literacy – the Brief Health Literacy Screen. The European Systematic Coronary Risk Evaluation and Framingham Risk Score were calculated.
Results
About 20% of the participants had low health literacy. Low health literacy was independently associated with the presence of ultrasound-detected carotid artery plaques after adjustment for age and education, odds ratio (95% confidence interval) 1.54 (1.28–1.85), demonstrating a similar level of risk as for smoking. Health literacy was associated with CIMT in men. Low health literacy was associated with higher CVD risk scores. Sensitivity analyses with low health literacy set to 9% or 30% of the study sample, respectively, yielded essentially the same results.
Conclusions
Low health literacy was independently associated with carotid artery plaques and a high level of CVD risk scores. Presenting health information in a fashion that is understood by all patients may improve preventive efforts.
Introduction
Health literacy, the degree to which individuals understand health information, may have a pivotal role in the prevention of cardiovascular disease (CVD). 1 A plausible mechanism may be that health literacy determines an individual's knowledge about health issues and his or her level of self-efficacy, essential factors for attaining a healthy lifestyle. 2 Health literacy is related to social inequalities and age, with older individuals generally having lower health literacy 3 and higher education or socioeconomic position indicating higher health literacy. A recent scientific statement from the American Heart Association found crucial gaps in the literature on health literacy and CVD, 4 and no study has yet addressed the issue of health literacy and subclinical atherosclerotic disease. Ultrasound-measured carotid artery plaques can independently predict CVD and may be seen as an early manifestation of the disease.5,6 CVD accounts for a high proportion of deaths due to non-communicable diseases and are, to a large extent, caused by individuals' lifestyle habits. 7 Reducing behavioral risk factors would substantially decrease the rate of CVD development. 8 Unfortunately, long-term change in lifestyle intervention trials has been weak. 9 Much emphasis in lifestyle trials has, to date, been focused on discussing details concerning different diets or training programs, while the only consistent finding for the lack of long-term change has been poor adherence. 10 Health literacy has repeatedly been associated with adherence to a healthier lifestyle.2,11–13
Our hypothesis is that low health literacy is associated with increased risk for CVD, presence of ultrasound-measured carotid artery plaques and increased carotid intima-media wall thickness (CIMT) among asymptomatic persons.
Methods
Design and study population
The study used baseline data (cross-sectional analysis) from the VIsualiZation of asymptomatic Atherosclerotic disease for optimum cardiovascular prevention (VIPVIZA), a randomized controlled trial (RCT) nested within the Västerbotten Intervention Program (VIP) in Northern Sweden. 14 The aim of the RCT is to explore the role that pictorial representation of silent carotid atherosclerosis may have on the way people act and the extent to which they adhere to behavioral and pharmacological preventive treatment. The VIP was initiated in the 1990s and has been described in detail elsewhere. 15 Participation rates in recent years have been 60–70%, with only small bias in social selection. 16
Subjects were invited to the VIPVIZA on the occasion of their participation in VIP (n = 4177) based on the following inclusion criteria: 1) 40 years of age and a history of CVD before the age of 60 among first-degree relative(s); 2) 50 years of age and at least one CVD risk factor (smoking, diabetes, hypertension, low-density lipo-protein (LDL) cholesterol ≥4.5 mmol/L, waist circumference ≥102 cm for men and ≥88 cm for women, history of CVD before the age of 60 among first-degree relative(s); or 3) 60 years of age. Individuals were excluded from the study and referred to the healthcare organization if a clinically significant stenosis ( ≥50% luminal narrowing) was detected by the ultra-sound examination (n = 22). Further details of the VIPVIZA trial have recently been published. 14 The subjects were enrolled between April 2013 and June 2016 (n = 3532). Seventy-three subjects (2%) had missing values in at least one of the main variables – health literacy and carotid artery plaques – and were excluded, thus leaving 3459 subjects (1632 men and 1827 women) in our study sample. All study participants provided written informed consent. VIPVIZA was approved by the Regional Ethical Review Board, Umeå University (Dnr 2011-445-31M, 2012-463-32M, 2013-373-32M).
Measurements
Biomedical and self-reported variables from the VIP
Blood samples for the measurement of lipids and glucose were drawn at the baseline VIP visit, as well as measurements of waist circumference, height, body weight, systolic and diastolic blood pressure. Participants completed a general questionnaire containing questions of a psychological, social and biomedical nature pertaining to CVD. 15 Education was classified into low (compulsory school education), medium (upper secondary education) and high (university/academics). Smoking was classified as being a current smoker (daily or occasional) or non-smoker (never or former).
Health literacy
Health literacy is defined as basic health literacy – that is, to read and understand written medical information. 17 Before the ultrasound examination, the participants answered a slightly modified version, based on prior measurement studies (personal communication), of the Three-item Brief Health Literacy Screen (BHLS) in which the three questions were formulated as the following statements18,19: “I feel confident filling out medical forms by myself (for example, with questions about diseases I have suffered from or medication I take)”; “I often ask for help reading information from the health care”; and “I often have problems learning about my medical condition because of difficulties reading information from the health care”. The statements were answered on a seven-point Likert scale, with strongly disagreeing at one end and strongly agreeing at the other. The points were then summed to make a health literacy score ranging from 3 to 21 points. Low health literacy was defined as having 17 points or less and high health literacy as 18 to 21 points (Supplementary Figure 1).
Ultrasound measurements of carotid artery plaques and CIMT
Ultrasound examinations were performed according to a standardized protocol 20 by trained sonographers. A portable ultrasound instrument with real-time automatic CIMT measurements was used (CardioHealth Station®, Panasonic Healthcare Corporation of North America, Newark, NJ, USA). 21 CIMT was measured in the left and right common carotid arteries at predefined angles of insonation. 22 For the measurement of CIMT, the highest of the mean values, irrespective of side and angle, was used. Presence of atherosclerotic plaque was recorded on both sides according to the Mannheim consensus. 20 In this study, having plaque was defined as having plaque on either one or both sides.
Cardiovascular risk scores
The Framingham Risk Score (FRS) 23 and the European Systematic Coronary Risk Evaluation (SCORE) 24 are two commonly used gender-specific algorithms for assessing the individual absolute 10-year cardiovascular risk in percentage terms, where FRS predicts CVD morbidity and mortality and SCORE predicts CVD mortality. Both FRS and SCORE use age in their algorithms as well as important known cardiovascular risk factors, such as smoking, blood lipids and blood pressure.
Statistical methods
Distributions of continuous and categorical variables were tested with independent t-tests and Chi-Square tests, respectively. Pearson (Spearman for education) correlation coefficients were used to assess relations between health literacy and age, education, cardiovascular risk factors and outcomes. Differences between the health literacy groups in continuous outcome variables (i.e. FRS and SCORE) were tested in linear regression models. Differences between the health literacy groups in categorical outcome variables, such as presence or absence of carotid artery plaques, or belonging to quartiles of age- and sex-adjusted CIMT, were tested in logistic regression models. Sensitivity analyses, testing the robustness of the health literacy variable on the association with carotid artery plaques, were performed. SPSS statistics version 25 was used and a p-value <0.05 was considered as significant.
Results
Baseline characteristics among those with high and low health literacy (HL) in the whole study population and by gender, presented as mean (SD) or proportion (%).
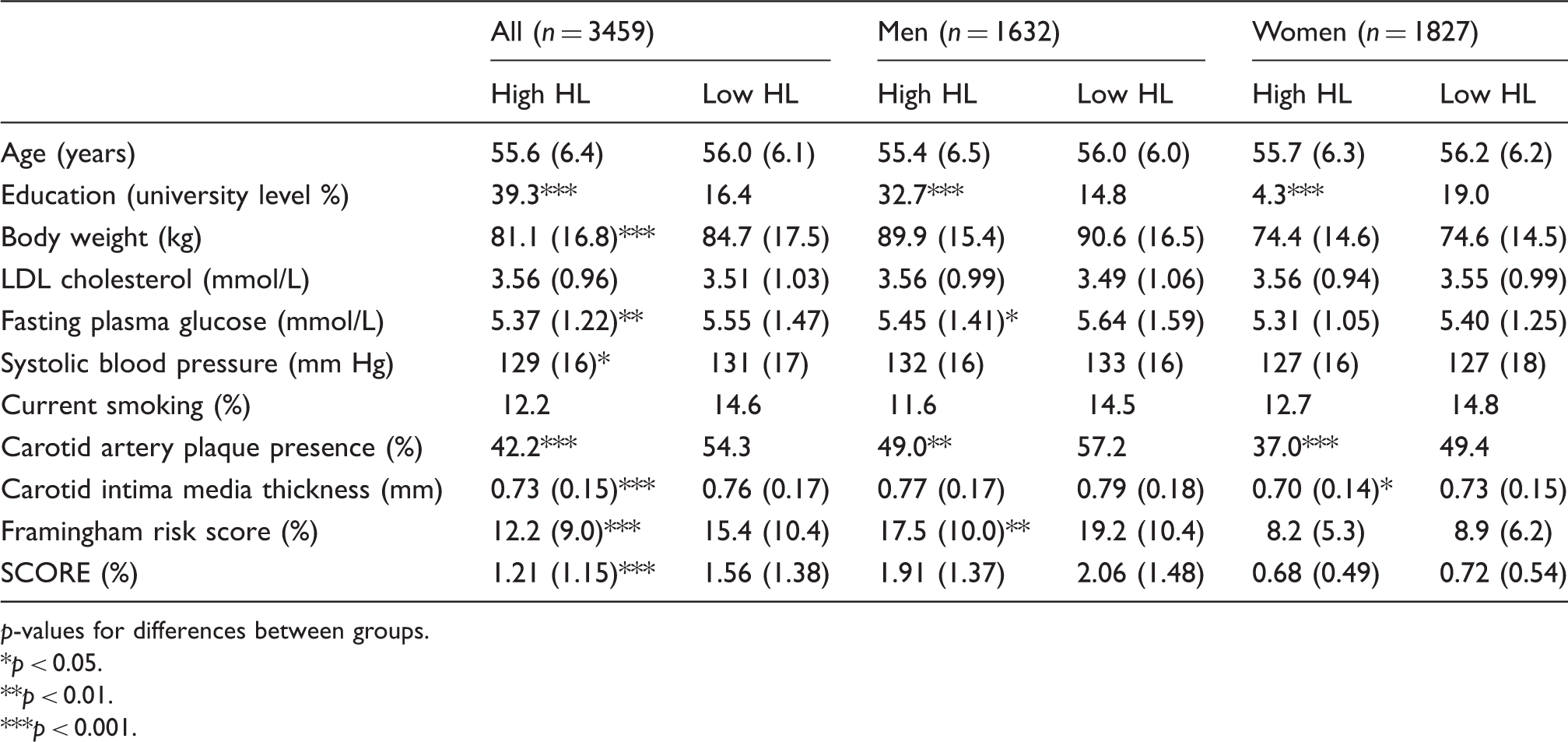
p-values for differences between groups.
p < 0.05.
p < 0.01.
p < 0.001.
The correlation between health literacy, age, education, cardiovascular risk factors and outcomes (CIMT, FRS, SCORE).
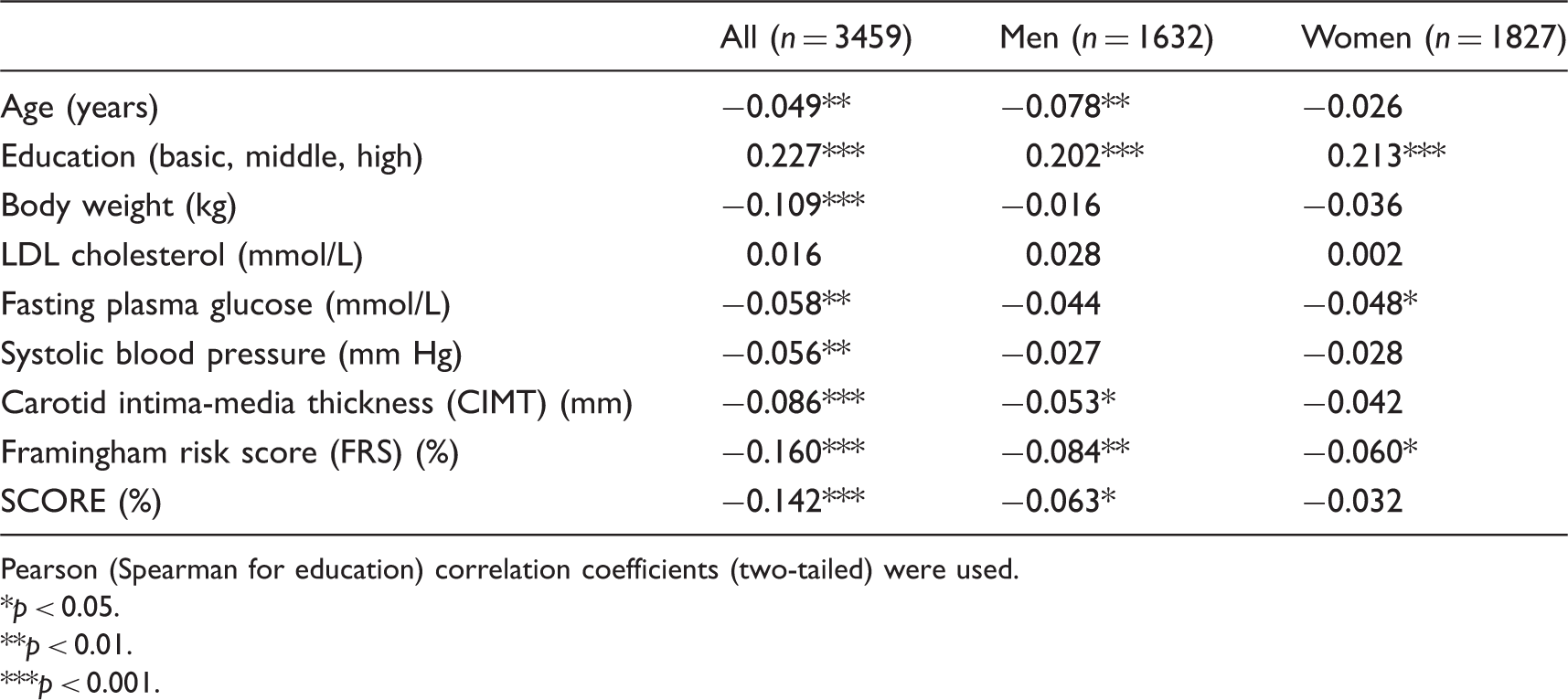
Pearson (Spearman for education) correlation coefficients (two-tailed) were used.
p < 0.05.
p < 0.01.
p < 0.001.
Logistic regression with presence of carotid artery plaques as outcome assessed against health literacy in comparison with cardiovascular risk factors as predictor variables after adjustment for age and education.
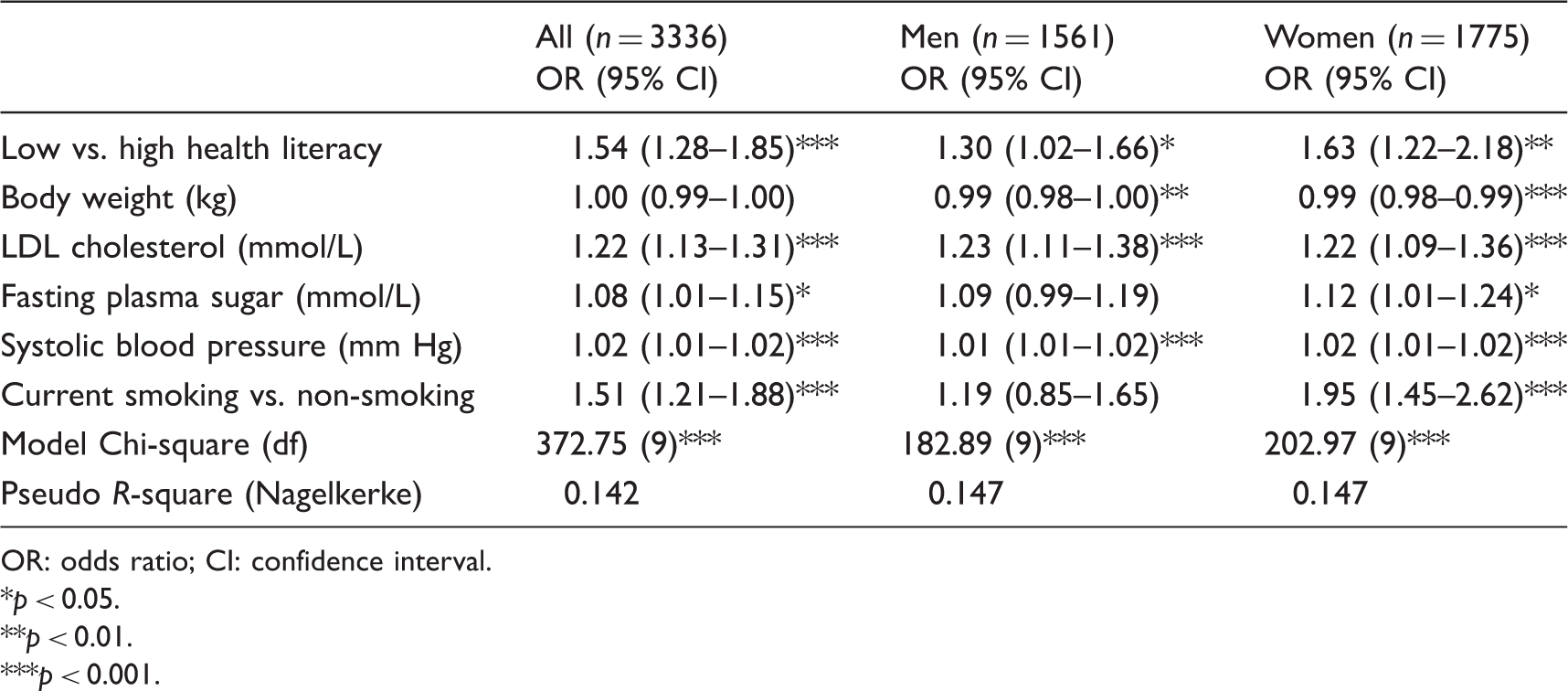
OR: odds ratio; CI: confidence interval.
p < 0.05.
p < 0.01.
p < 0.001.
Logistic regression with carotid intima-media wall thickness (CIMT) categorized as the highest quartile of age- and sex-adjusted maximum mean of CIMT versus the other quartiles as outcome assessed against health literacy in comparison with other cardiovascular risk factors as predictor variables after adjustment for age and education.
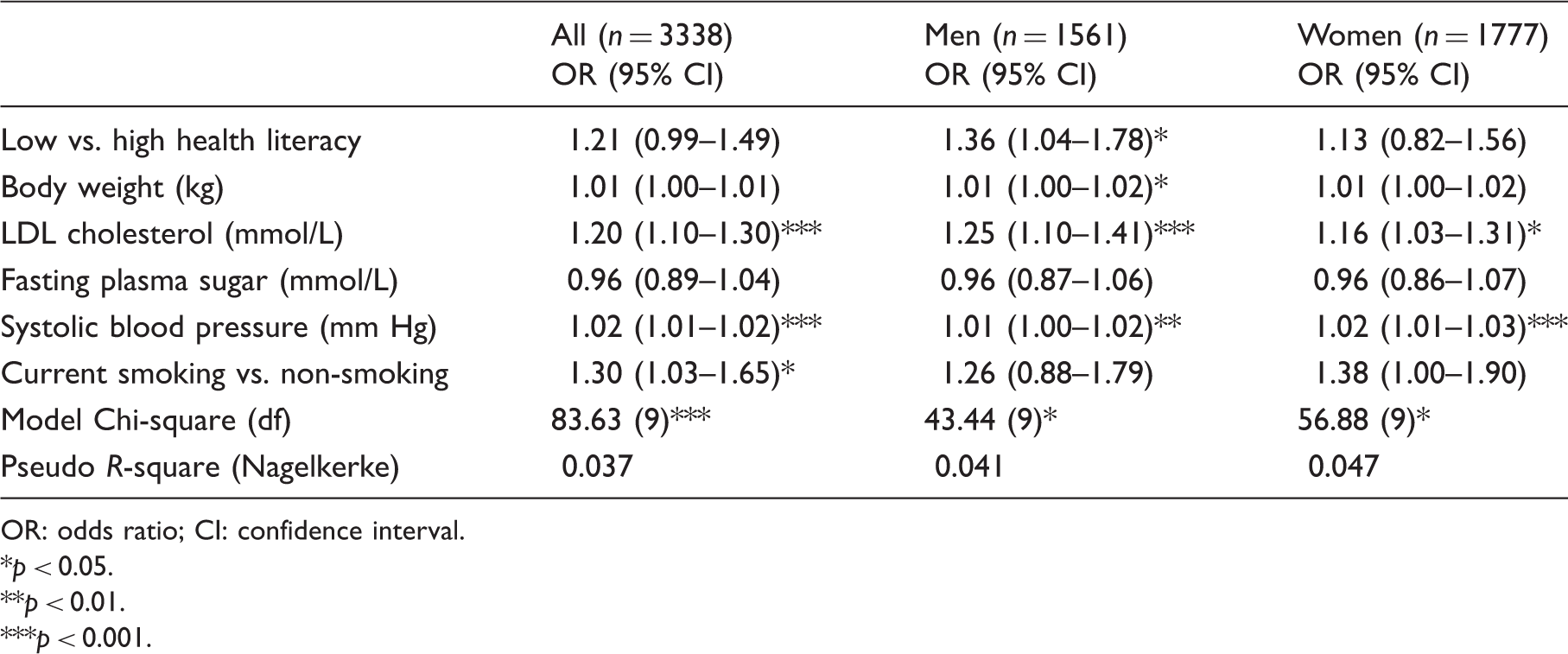
OR: odds ratio; CI: confidence interval.
p < 0.05.
p < 0.01.
p < 0.001.
In the linear regression models, health literacy (low vs. high), after adjustment for education, was assessed against FRS or SCORE as outcome. In the population as a whole, low health literacy was associated with an increase in FRS of 2.33 (95% CI) 1.54–3.11, p < 0.001, and an increase in SCORE of 0.28, (95% CI) 0.18–0.38 (p < 0.001). Low health literacy was also associated with FRS in men with a borderline significant risk increase of 1.13 (95% CI) 0.002–2.27 (p = 0.05). SCORE was not associated with health literacy in either men or women (data not presented).
In the sensitivity analyses, setting the proportion of low health literacy in the study sample to 9% and 30% (instead of 20%), respectively, gave essentially the same results in the full logistic regression model with carotid artery plaque as the outcome (data not presented).
Discussion
The study reports an association between low health literacy and increased risk of having ultrasound-detected carotid artery plaques. The finding held in both men and women after adjustment for potential confounders, such as age and education, and in competition with other known cardiovascular risk factors. The increased risk (54%) for carotid artery plaques was on the same level as being a smoker instead of a non-smoker (51%). Using CIMT as outcome replicated the independent inverse association for men, but not for women or the population as a whole. This lack of significant association between health literacy and CIMT may partly be explained by the generally high health literacy in women (compared with men; cf. Supplementary Figure 1). Thus, if you have a sufficiently high level of health literacy (even if low compared with other women) it may still buffer against the risk factors. In the population as a whole, and in men for FRS, health literacy was associated with cardiovascular risk when measured by FRS and SCORE after adjustment for education. There was a gender difference in the magnitude of CVD risk scores, with men having at least twice the risk scores of women. Possibly the lower CVD risk in women may be an effect of their higher health literacy, and may also explain the gender difference we saw in the association between health literacy and CIMT. Health literacy was not associated with SCORE in either gender individually.
There are crucial gaps in the knowledge of health literacy and CVD, as recently stated by the American Heart Association, 4 which found no earlier studies addressing the issue of health literacy and subclinical atherosclerotic disease. One study found health literacy to be associated with adherence to taking prescribed medications, 25 and another study showed an inverse association with 30-day re-admission after suffering acute coronary syndromes. 26 A few studies were found on health literacy and conventional cardiovascular risk factors. 4
VIP is a large population-based cohort for which previous reports have shown little evidence of selection bias. 16 A high participation rate (84.6%) among those eligible for the VIPVIZA study indicates that the present cohort is generalizable to a population at low/intermediate risk of CVD. The three-item BHLS has been used earlier as a health literacy screening tool,18,19,27 and has shown strong correlation to more extensive health literacy measures such as the Short Test of Functional Health Literacy in Adults and the Rapid Estimate of Adult Literacy in Medicine, at least when it comes to screening for low health literacy.18,19 It uses self-reported data, and is quick, easy and inexpensive to administer – characteristics that are well suited for screening of large study populations. Furthermore, self-reported tests are less likely to induce anxiety and shame when compared with performance-based (objective) tests. 28 On the other hand, self-assessment instruments are inclined to induce self-report bias. The use of a Swedish translation of BHLS, as well as the homogenous distribution of health literacy in our population sample, must be seen as limitations of the study. The distribution was skewed towards the high health literacy side (Supplementary Figure 1), a kind of distribution expected in populations of high educational level. The robustness of classifying low and high health literacy was tested in two sensitivity analyses and found to be sufficient. The proportion with low health literacy was set to 9% and 30%, respectively, rendering about the same results for the association between health literacy and carotid artery plaques. Another limitation of this study is the use of cross-sectional analysis (only baseline data), making inferences of causality impossible. The low prevalence of smoking in the study population may have underestimated the impact smoking has on our outcome variables.
An important goal for healthcare providers, not least from an ethical point of view, must be to present health information in a fashion that all patients understand and are able to act upon. Our study indicates that this could also be an important step in preventing CVD.
In summary, health literacy, the degree to which we understand and act upon health information, was in our study population independently and inversely associated with having carotid artery plaques and increased risk for CVD.
Supplemental Material
CPR882821 Supplemental Material - Supplemental material for Health literacy is independently and inversely associated with carotid artery plaques and cardiovascular risk
Supplemental material, CPR882821 Supplemental Material for Health literacy is independently and inversely associated with carotid artery plaques and cardiovascular risk by Bernt Lindahl, Margareta Norberg, Helene Johansson, Kristina Lindvall, Nawi Ng, Maria Nordin, Steven Nordin, Ulf Näslund, Amanda Persson, Davide Vanoli and Peter J Schulz in European Journal of Preventive Cardiology
Footnotes
Acknowledgements
Carola Sundholm and Maria Backlund, research nurses, and the ultrasound technicians at the Department of Clinical Physiology, Heart Centre, and the database manager Wolfgang Lohr are strongly acknowledged for their great work throughout the study, and Rachel Nicoll, PhD, for her language review.
Author contribution
BL, MN, HJ, KL, NN, MN, SN, UN, VD and PS contributed to conception and design. BL, MN, NN, UN, AP, DV and PS analyzed and interpreted data. BL and NN performed statistical analysis. BL, MN and PS drafted the manuscript. All authors critically revised the manuscript, gave final approval and agreed to take responsibility for the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by non-profit organizations, with major funding from the Västerbotten County Council (Central ALF, Dnr ALFVLL-298001), the Swedish Research Council (Dnr 521-2013-2708), the Heart and Lung Foundation (Dnr 20150369, 20170481) and the Swedish Society of Medicine. VIPVIZA was also funded by the Heart Foundation in Northern Sweden, STROKE – the national association, the Foundation for Stroke Research in Northern Sweden, The Swedish Insurance Society
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.