
Abstract
Background
Ethnic differences in the age-of-onset of cardiovascular risk factors may necessitate ethnic-specific age thresholds to initiate cardiovascular risk screening. Recent European recommendations to modify cardiovascular risk estimates among certain ethnic groups may further increase this necessity.
Aims
To determine ethnic differences in the age to initiate cardiovascular risk screening, with and without implementation of ethnic-specific modification of estimated cardiovascular risk.
Methods
We included 18,031 participants of Dutch, South-Asian Surinamese, African Surinamese, Ghanaian, Turkish and Moroccan background from the HELIUS study (Amsterdam). Eligibility for cardiovascular risk screening was defined as being eligible for blood pressure-lowering treatment, based on a combination of systolic blood pressure, estimated cardiovascular risk, and ethnic-specific conversion of estimated cardiovascular risk as recommended by European cardiovascular disease prevention guidelines. Age-specific proportions of eligibility were determined and compared between ethnic groups via logistic regression analyses.
Results
Dutch men reached the specified threshold to initiate cardiovascular risk screening (according to Dutch guidelines) at an average age of 51.5 years. Among ethnic minority men, this age ranged from 39.8 to 52.4. Among Dutch women, the average age threshold was 53.4. Among ethnic minority women, this age ranged from 36.8 to 49.1. Age-adjusted odds of eligibility were significantly higher than in the Dutch among all subgroups, except among Moroccan men. Applying ethnic-specific conversion factors had minimal effect on the age to initiate screening in all subgroups.
Conclusions
Most ethnic minority groups become eligible for blood pressure-lowering treatment at a lower age and may therefore benefit from lower age-thresholds to initiate cardiovascular risk screening.
Introduction
Cardiovascular disease (CVD) prevention strategies have contributed to approximately half the decline in CVD mortality in western societies. 1 A key element of these prevention strategies is the initiation of preventive pharmacological treatment in individuals with a high estimated CVD risk.2–6
Cardiovascular risk and, consequently, eligibility for preventive treatment increase with age. 7 Therefore, guidelines often recommend an age threshold to initiate cardiovascular risk screening, in part to prevent unnecessary screening among individuals with a low probability to be eligible for preventive treatment.2–6 For example, in The Netherlands, guidelines recommend to withhold cardiovascular risk screening in absence of symptoms or complaints until the age of 50 years. 2
Relative to European host populations, certain ethnic minority groups show a younger onset of cardiovascular risk factors and a higher proportion eligible for preventive cardiovascular treatment at a similar age.8–11 Despite this, guidelines generally do not recommend initiation of CVD risk screening at a younger age for most ethnic minority groups.2–6
Recent recommendations from the European (EU) CVD prevention guideline may result in even greater discrepancies in the age threshold for eligibility for preventive cardiovascular treatment and, consequently, age-of-onset of cardiovascular risk screening. 3 In particular, in recognition that CVD incidence rates differ between ethnic groups even at similar estimated cardiovascular risk, the guideline has recommended to multiply estimated CVD risk by an ethnic-specific factor (e.g. 1.4 among first generation migrants from South Asia). 3 It is unknown how these ethnic-specific conversion factors may impact ethnic differences in the age at which individuals on average become eligible for treatment.
Thus, in this study, we aimed to assess ethnic differences in the proportion eligible for treatment as indicated by blood pressure (BP) treatment eligibility, determine whether ethnic-specific age-thresholds for cardiovascular risk screening may be warranted, and explore how the use of ethnic-specific conversion factors would affect the necessity of these ethnic-specific age-thresholds.
Methods
The HELIUS (Healthy Life in an Urban Setting) study is a large-scale cohort study on health and health care utilization among different ethnic groups living in Amsterdam, The Netherlands. The aims and design of the HELIUS study have been published. 12 In brief, baseline data-collection took place from 2011 to 2015. Participants between 18 and 70 years of age living in Amsterdam were randomly sampled, stratified by ethnicity, via the municipality register of Amsterdam. A total of 90,019 subjects received a written invitation. Approximately 55% were contacted, either by regular mail or after an additional home visit by an ethnically matched interviewer. Of those, 24,789 agreed to participate (participation rate of 50%). 12 Baseline data by both questionnaire and physical examination were obtained among 22,165 participants of Dutch, Surinamese, Ghanaian, Turkish and Moroccan ethnic origin. Questionnaires were filled out at home before the physical examination, and were available in Dutch, English or Turkish. If necessary, participants were offered assistance from a trained ethnically matched same-sex interviewer, speaking the preferred language of the participant. The study protocols were approved by the AMC Ethical Review Board, and all participants provided written informed consent.
Ethnicity
Participants’ ethnicity was defined according to the country of birth of the participant as well as that of his/her parents. 13 Specifically, a participant was considered to be of non-Dutch ethnic origin if he/she was born abroad and has at least one parent born abroad (first generation), or he/she was born in The Netherlands but both his/her parents were born abroad (second generation). Participants of Surinamese ethnic origin were further classified according to self-reported ethnic origin.
Cardiovascular risk factors
Participants were asked not to smoke or eat prior to the physical examination. All participants were asked to bring their prescribed medications to the research location, which were categorized using the Anatomical Therapeutic Chemical (ATC) classification system. BP-lowering medication included centrally acting anti-hypertensives (ATC code C02), diuretics (ATC code C03), beta-blockers (ATC code C07), calcium channel blockers (ATC code C08) and agents acting on the renin–angiotensin–aldosterone system (ATC code C09). Lipid-lowering medication was classified as ATC code C10. Glucose-lowering medication was classified as ATC code A10.
Smoking status, physical activity, presence of prior CVD and family history of CVD were assessed via questionnaire. BP was measured using a validated automated digital BP device (WatchBP Home; Microlife AG) on the left arm in a seated position after the person had been seated for at least 5 min. For body mass index (BMI), weight was measured in light clothing only on a Seca 877 scale to the nearest 0.1 kg and height was measured without shoes with a portable stadiometer (Seca 217) to the nearest 0.1 cm. BP and BMI measurements were performed twice and the mean of the two measurements was used in the analyses, with at least 15 s between BP measurements. Participants were considered to have diabetes if they reported a diabetes diagnosis, used glucose-lowering medication and/or in the case of a fasting glucose ≥7.0 mmol/l. Fasting blood samples were drawn after an overnight fast, and glucose, total cholesterol (TC) and high-density lipoprotein (HDL) cholesterol were determined by enzymatic colorimetric spectrophotometry, and serum creatinine was determined. Participants were asked to bring an early morning urine sample. Urinary albumin concentration (in mg/l) was measured by an immunochemical turbidimetric method (Roche Diagnostics). Estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI equation.
Estimation of cardiovascular risk
Ten-year risk of cardiovascular morbidity or mortality was estimated using the cardiovascular risk algorithm which is currently used in Dutch primary care. 2 This algorithm is derived from the SCORE algorithm for low risk countries and estimates the 10-year risk of fatal and non-fatal CVD based on age, sex, systolic BP (SBP), TC/HDL ratio and smoking status.2,7 Furthermore, the algorithm adds 15 years to the calendar age of patients with diabetes. 2 It can be used among patients who are between 40 and 70 years of age (25–55 for patients with diabetes) without prior CVD. Those below the age threshold were classified as low risk (i.e. below 10% and therefore only eligible in the case of an SBP of at least 180 mmHg), and those above the age threshold were classified as high risk (i.e. above 20% and, therefore, eligible in the case of an SBP above 140 mmHg).
Treatment indication
Similar to most other CVD prevention guidelines, CVD prevention guidelines in The Netherlands recommend to initiate BP-lowering medication among individuals with hypertension only when these individuals also show a high overall cardiovascular risk. Thus, in accordance with the 2012 cardiovascular risk prevention guidelines in The Netherlands we defined treatment indications for BP-lowering medication as a SBP above 140 mmHg combined with either an estimated cardiovascular risk of at least 20% or an estimated cardiovascular risk between 10% and 20% combined with sufficient additional cardiovascular risk factors (as described below). 2 Alternatively, an isolated SBP of at least 180 mmHg (i.e. grade 3 hypertension) was also considered to be an indication for BP-lowering treatment, regardless of estimated cardiovascular risk, in accordance with the guideline. 2
The presence of sufficient additional cardiovascular risk factors was defined as having at least two additional mild CVD risk factors or one additional severe cardiovascular risk factor. Mild cardiovascular risk factors included not achieving at least 30 min of moderate to intensive physical activity per day for five days per week (estimated by the SQUASH questionnaire), BMI of 30–35 kg/m2, eGFR of 30–60 ml/min per 1.73 m2 for those below the age of 65 and 30–45 ml/min per 1.73 m2 for those above the age of 65. Severe cardiovascular risk factors included a BMI above 35 kg/m2, eGFR below 30 ml/min per 1.73 m2, family history of a major cardiovascular event before the age of 60 (e.g. myocardial infarction or stroke), transient ischaemic attack, bypass or percutaneous coronary intervention on arteries of either the heart or lower limbs, or unexplained sudden death among a first degree relative before the age of 60, and, among patients with self-reported diabetes, the presence of metabolic syndrome as defined by the NCEP ATP-III criteria or the presence of microalbuminuria defined as albumin ≥ 20 mg/l in a morning urine sample.
In accordance with recommendations from the EU guideline for CVD prevention, ‘EU treatment indications’ will be determined by multiplying estimated cardiovascular risk by an ethnic-specific conversion factor. These factors are 1.4 among South-Asian Surinamese, 1.3 among African Surinamese and Ghanaian, 0.9 among Moroccans and 0.7 among Turkish participants. 3
Study population
From the total sample of 22,165 participants, 18,780 were potentially eligible based on reporting no prior CVD. We excluded participants with a Javanese Surinamese (n = 208), ‘other/unknown Surinamese’ (n = 223) or unknown/other ethnic background (n = 42) due to low statistical power. Next, we excluded participants based on missing data regarding cardiovascular risk (i.e. BP, smoking status, lipid profile, fasting glucose, and/or prior CVD; n = 276). Finally we excluded second generation migrants because current EU guidelines recommend ethnic-specific conversion factors only among first generation migrants (n = 3293). This resulted in a total study sample of 14,738 participants.
Statistical analysis
All analyses were stratified by ethnic background and sex. Distributions of baseline characteristics were calculated and compared between ethnic groups via chi-squared analysis or analysis of variance. The proportion of individuals eligible for treatment according to the 2012 Dutch guideline recommendations and EU recommendations of ethnic-specific risk factors was calculated both overall and stratified by age using five-year intervals.
We then estimated at what age the different subgroups reached a similar proportion of eligibility for BP-lowering treatment. To do so, we first determined to what absolute proportion of Dutch residents CVD guidelines would recommend CVD risk screening. According to these guidelines, screening should be initiated from 50 years of age among Dutch male smokers. For this, we determined the proportion eligible for BP-lowering treatment in this group via binary logistic regression analysis, using age as a continuous independent variable and indication for BP-lowering treatment (yes/no) as the dependent variable, and found that this absolute proportion was 10.77%. Using this as our reference, we then used binary logistic regression analysis to estimate at what age the participants (overall, so smokers and non-smokers combined, but stratified for sex) reach a proportion eligible for BP-lowering treatment of 10.77%. We stratified for sex and ethnic background. These analyses were conducted both according to the Dutch guideline and after implementing ethnic-specific conversion factors as recommended by EU CVD prevention guidelines. In addition, to examine whether the age to initiate cardiovascular risk screening differs significantly between ethnic minority groups and the Dutch, we determined whether, after adjustment for age, ethnic minority groups differed in the proportion eligible for BP-lowering treatment relative to the Dutch.
As a sensitivity analysis, we repeated our analyses among those participants eligible for CVD risk estimation using the Dutch SCORE algorithm only (i.e. those aged 40–70 or, among those with diabetes, those aged 25–55). In addition, in some countries, individuals with diabetes are regarded as high CVD risk individuals, regardless of estimated CVD risk. 3 Thus, for these countries, the ethnic-specific conversion factors recommendations would not be applicable to individuals with diabetes. Therefore, we checked whether our results would differ when participants with diabetes were excluded.
Results
General characteristics of the study population, by ethnicity and sex.
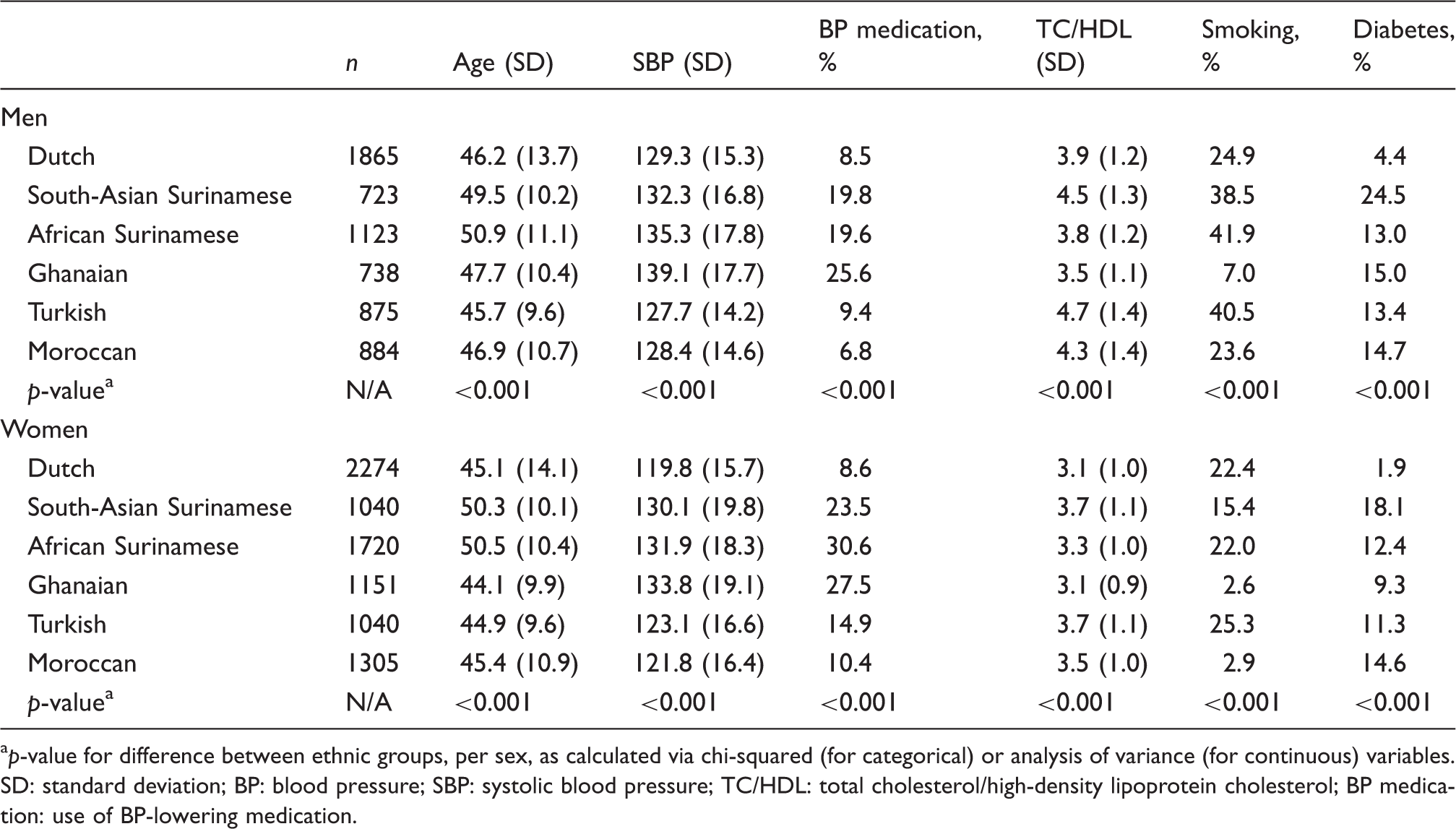
p-value for difference between ethnic groups, per sex, as calculated via chi-squared (for categorical) or analysis of variance (for continuous) variables.
SD: standard deviation; BP: blood pressure; SBP: systolic blood pressure; TC/HDL: total cholesterol/high-density lipoprotein cholesterol; BP medication: use of BP-lowering medication.
Proportion eligible for blood pressure lowering treatment and age (95% confidence interval) at which the proportion of participants eligible for blood pressure lowering treatment reaches screening thresholds, by ethnicity and sex.
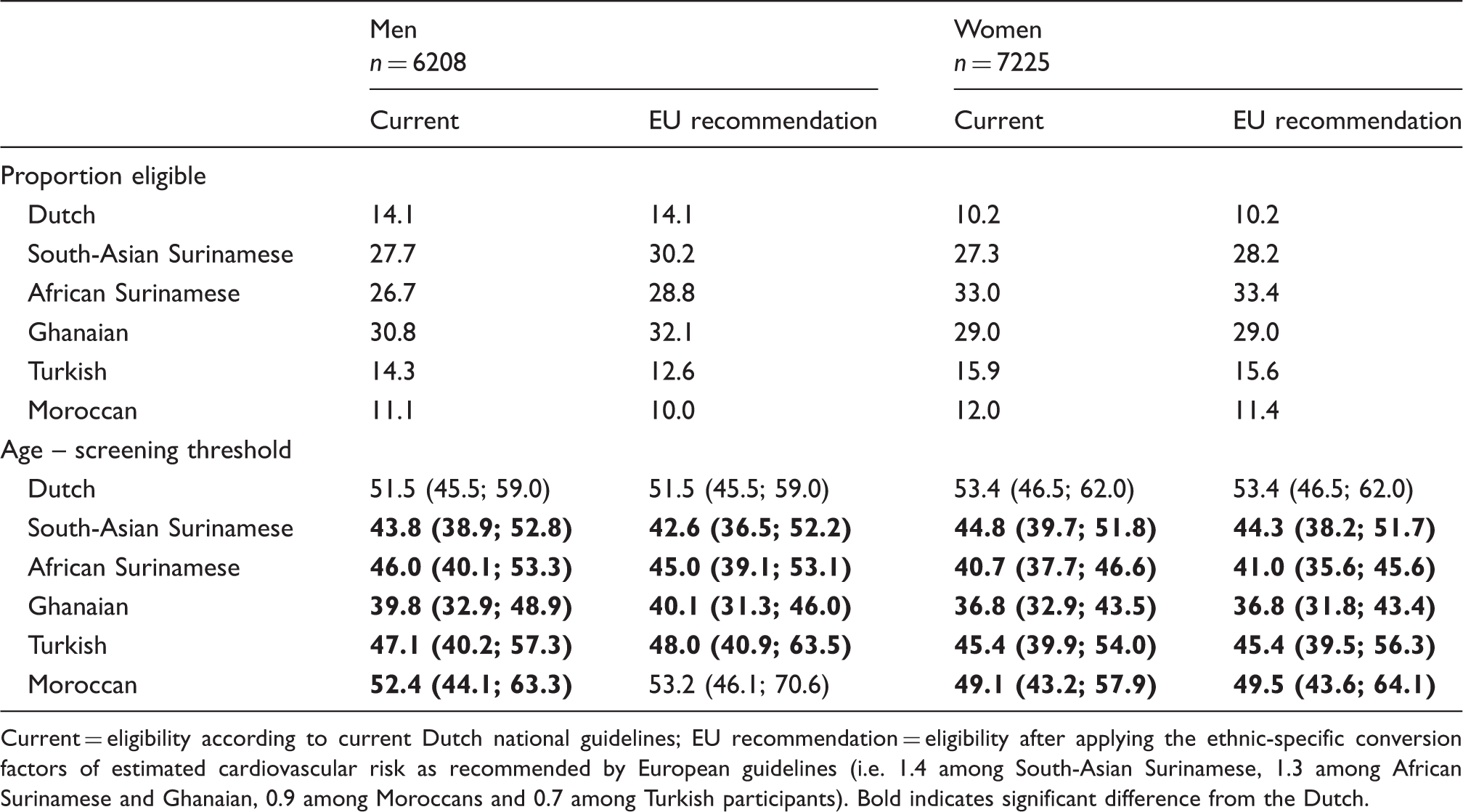
Current = eligibility according to current Dutch national guidelines; EU recommendation = eligibility after applying the ethnic-specific conversion factors of estimated cardiovascular risk as recommended by European guidelines (i.e. 1.4 among South-Asian Surinamese, 1.3 among African Surinamese and Ghanaian, 0.9 among Moroccans and 0.7 among Turkish participants). Bold indicates significant difference from the Dutch.
Next, we estimated at what age the different ethnic groups reach a similar proportion of eligibility for BP-lowering treatment as our reference category (i.e. 10.77%). Among men, this age ranged from 43.8 years among Ghanaians to 52.4 years among Moroccans versus 51.5 among the Dutch (Table 2). The age threshold for initiation of screening was largely similar when EU conversion factors were applied. Moreover, these ages as estimated by logistic regression analyses corresponded to the age categories in which the proportion of participants eligible for BP-lowering treatment exceeded the reference value of 10.77% (Supplementary Material Table S1 online). Among women, the estimated age at which an eligibility proportion of 10.77% was reached ranged from 36.8 years among Ghanaians to 49.1 among Moroccans versus 53.4 years among the Dutch. Similar to men, the age threshold to initiate screening did not differ strongly after applying EU conversion factors, and these ages as estimated by logistic regression analyses corresponded to the age categories in which the proportion of participants were eligible for BP-lowering treatment exceeded the reference value of 10.77% (Supplementary Table S2). Moreover, among all ethnic minority groups, age-adjusted odds of being eligible for BP-lowering treatment were higher than in the Dutch, except among Moroccan men (Supplementary Table S3).
Finally, as a sensitivity analysis, we repeated our analysis after excluding participants who were not eligible for cardiovascular risk estimation according to EU CVD prevention guidelines, based on age or diabetes status (Supplementary Table S4). Results from these analyses were similar to results from our main analyses, showing substantial ethnic differences in the age of initiation of cardiovascular risk screening, with minimal effect of implementing EU guideline recommendations. Exclusion based on each criterion separately did not appreciably affect our findings (data not shown).
Discussion
Key findings
Eligibility for BP-lowering treatment is generally reached at a younger age among ethnic minority groups than among the Dutch. Based on thresholds as used in Dutch CVD prevention guidelines, ethnic minority groups reach screening thresholds at an age that is 5–10 years lower than in the Dutch. Recent EU recommendations to multiply estimated CVD risk with an ethnic-specific factor among first generation migrants minimally affected the estimates.
Evaluation of potential limitations
The response rates of the HELIUS study may have resulted in some selection bias. Non-response analyses based on socioeconomic status (SES) found no indication that this was the case, but it is unclear whether some selection-bias did occur based on other variables, including cardiovascular risk factors. 12 Furthermore, BP was measured on only one occasion. This may have resulted in some artificial differences in the eligibility for BP-lowering treatment due to ethnic variation in the white coat effect. 14
Eligibility for cardiovascular risk screening was for a section of the respondents determined on the basis of current treatment, as those already receiving treatment are considered to be eligible for treatment. This may have introduced bias. For example, current medication was based on self-report and whether participants brought their active medication to the physical examination site. The accuracy of determining current medication may have differed between ethnic groups, for example due to ethnic differences in therapy adherence and tendency to bring and present all their active medication during the physical examination. 15 If the propensity to do so was lower among ethnic minority groups, the eligibility for BP-lowering medication may have been underestimated, and ethnic differences (compared with Dutch) in eligibility/age thresholds may have been underestimated. Moreover, bias may also be introduced if individuals are treated before having an indication (as this would overestimate eligibility for treatment according to the 2012 Dutch guideline). We have no indication that this would have occurred frequently.
We compared ethnic differences in the age threshold for initiation of cardiovascular risk screening, using the risk of 50-year-old smoking Dutch men as a reference, as recommended by the Dutch CVD prevention guidelines. 2 This reference may differ from reference categories as described by cardiovascular guidelines from other countries and continents.3,4,6 The choice of the reference category may change the estimated age at which different ethnic groups become eligible for screening. However, the observed ethnic differences in this age are likely to remain.
In accordance with clinical practice in The Netherlands, we classified cardiovascular risk status according to overall CVD risk.2,3 In contrast, EU guidelines recommend to estimate fatal rather than total cardiovascular risk. Repeating our analyses using fatal and applying CVD risk categories as mentioned in EU guidelines (i.e. low-moderate (<5%), high (5–10%) and very high (>10%) resulted in similar ethnic differences in the age threshold for initiation of cardiovascular risk screening, with minimal effect of applying ethnic-specific conversion of estimated CVD risk (data not shown). In addition, in contrast to the guidelines from some countries, we applied SCORE to (young) individuals with diabetes. Excluding individuals with diabetes resulted in a slightly (e.g. two years) older estimated age to initiate cardiovascular risk screening, with similar ethnic disparities.
Finally, although we applied the SCORE algorithm to different ethnic groups (in accordance to current clinical practice), SCORE is validated mainly among Caucasian majority populations. Estimates suggest that CVD risk may be underestimated among ethnic minority groups. 3 If so, the age thresholds among ethnic minority groups may need to be lower (younger) than estimated in this study.
General discussion of key findings
The proportion eligible for BP-lowering treatment differs considerably between ethnic groups. This is in accordance with earlier studies regarding age-adjusted ethnic differences in hypertension or eligibility for BP-lowering treatment.16–18 These studies identified many factors contributing to the ethnic differences in hypertension, such as SES and smoking rates.16–19 In the current study we did not explore these factors.
Most ethnic groups reached eligibility thresholds to initiate cardiovascular risk screening at a substantially lower age than the Dutch, which was related to both the younger onset of hypertension (including SBP ≥180 mmHg) and the higher estimated cardiovascular risk among ethnic minority groups at younger age. Considering the younger onset of cardiovascular risk among ethnic minority groups, general (i.e. non-ethnic-specific) age thresholds for screening result in a particularly long exposure to cardiovascular risk among these groups. This is likely to contribute to ethnic differences in CVD, as prolonged exposure to hypertension increases cardiovascular risk.20,21 Ethnic-specific age thresholds to initiate screening may be required to reduce these differences.
A high proportion of participants below the age of 50 with an indication for BP-lowering treatment were receiving such treatment, particularly among women and among men in high-risk ethnic groups, suggesting that screening occurs below the age of 50, despite CVD guideline recommendations (Supplementary Table S5).2,22 This early screening may be based in part on awareness of the young onset of hypertension, or on a familial history of high cardiovascular risk. Incorporating family history in this manner is important, especially considering that the cardiovascular disease risk associated with hypertension may be greater among those with a family history of CVD.2,22,23 However, it is unclear whether family history alone is sufficient to ensure timely screening and intervention among individuals with a young onset of cardiovascular risk.
We found that multiplying SCORE by ethnic-specific factors between 0.7 (Turkish) and 1.4 (South-Asian Surinamese) resulted in a difference in eligibility between −1.1% and 2.5% among ethnic minority men and −0.4% to 0.9% among ethnic minority women. These differences are smaller than initially expected and show that, in most participants, a change in estimated cardiovascular risk does not affect eligibility for treatment, either because (1) the change in estimated cardiovascular risk does not result in a change in cardiovascular risk category or (2) a change in cardiovascular risk did occur, but the individual already had an indication for treatment, or was not hypertensive.
Moreover, applying ethnic-specific conversion factors did not substantially reduce ethnic differences in eligibility for BP-lowering treatment, or the age to initiate cardiovascular risk screening. Thus, multiplying SCORE (or other measures of cardiovascular risk) by a simple constant factor (ratio) may not be sufficient to reduce ethnic differences in cardiovascular risk. This might be taken to imply that more sophisticated methods may be necessary to accurately estimate cardiovascular risk among different ethnic groups (e.g. by taking into account the duration of exposure to cardiovascular risk factors, thereby taking into account ethnic differences in the age-of-onset of cardiovascular risk factors).20,21,24
In this study, we used The Netherlands as a European example to show how ethnic groups may differ in the age to initiate CVD risk screening. Earlier work has shown that ethnic differences in cardiovascular risk factors in The Netherlands are comparable to ethnic differences in other countries, although the magnitude of differences may vary between countries. 25 More studies are required to determine the magnitude of ethnic differences in age-adjusted eligibility for screening in other countries, taking into account the national guidelines of those countries.
In this study, we focused mainly on BP-lowering treatment. Similar to BP-lowering treatment, ethnic groups may also differ in prevalence and age-of-onset of dyslipidaemia, and consequently the age at which screening thresholds for dyslipidaemia may be reached.9,11 This is also important considering the dose-dependent association of cumulative exposure to dyslipidaemia with cardiovascular risk. 24 Considering that the 2012 Dutch guideline and clinical practice are somewhat conservative compared with EU recommendations, we recommend such studies to investigate ethnic differences in the proportion eligible for lipid-lowering therapy, based on clinical settings that better reflect current EU recommendations.2,3
Conclusion
Ethnic minority groups generally become eligible for BP-lowering treatment at a younger age than the Dutch. Recent recommendations to implement ethnic-specific conversion factors for estimated cardiovascular disease risk do not seem to affect these ethnic differences. Based on our findings, the age threshold to initiate cardiovascular risk screening may need to be tailored to specific ethnic groups.
Supplemental Material
Supplemental material for Eligibility for cardiovascular risk screening among different ethnic groups: The HELIUS study
Supplemental Material for Eligibility for cardiovascular risk screening among different ethnic groups: The HELIUS study by Wilco Perini, Marieke B Snijder, Charles Agyemang, Ron JG Peters, Anton E Kunst and Irene GM van Valkengoed in European Journal of Preventive Cardiology
Footnotes
Author contribution
WP and IGMV contributed to the conception of the work, all authors contributed to the design of the work. MBS and RJGP contributed to the acquisition of the work, all authors contributed to the analysis and interpretation of the work. WP drafted the manuscript, MBS, CA, RJGP, AEK and IGMV critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
We are most grateful to the participants of the HELIUS study and the management team, research nurses, interviewers, research assistants and other staff who have taken part in gathering the data of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the HELIUS study is conducted by the Academic Medical Centre Amsterdam and the Public Health Service of Amsterdam. Both organizations provided core support for HELIUS. The HELIUS study is also funded by the Dutch Heart Foundation, The Netherlands Organization for Health Research and Development (ZonMw), European Union (FP-7) and the European Fund for the Integration of non-EU immigrants (EIF).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.