
Abstract
Background
The REACH-HF (Rehabilitation EnAblement in CHronic Heart Failure) trial found that the REACH-HF home-based cardiac rehabilitation intervention resulted in a clinically meaningful improvement in disease-specific health-related quality of life in patients with reduced ejection fraction heart failure (HFrEF). The aims of this study were to assess the long-term cost-effectiveness of the addition of REACH-HF intervention or home-based cardiac rehabilitation to usual care compared with usual care alone in patients with HFrEF.
Design and methods
A Markov model was developed using a patient lifetime horizon and integrating evidence from the REACH-HF trial, a systematic review/meta-analysis of randomised trials, estimates of mortality and hospital admission and UK costs at 2015/2016 prices. Taking a UK National Health and Personal Social Services perspective we report the incremental cost per quality-adjusted life-year (QALY) gained, assessing uncertainty using probabilistic and deterministic sensitivity analyses.
Results
In base case analysis, the REACH-HF intervention was associated with per patient mean QALY gain of 0.23 and an increased mean cost of £400 compared with usual care, resulting in a cost per QALY gained of £1720. Probabilistic sensitivity analysis indicated a 78% probability that REACH-HF is cost effective versus usual care at a threshold of £20,000 per QALY gained. Results were similar for home-based cardiac rehabilitation versus usual care. Sensitivity analyses indicate the findings to be robust to changes in model assumptions and parameters.
Conclusions
Our cost-utility analyses indicate that the addition of the REACH-HF intervention and home-based cardiac rehabilitation programmes are likely to be cost-effective treatment options versus usual care alone in patients with HFrEF.
Keywords
Introduction
Heart failure with reduced ejection fraction (HFrEF) represents a major health issue and is associated with considerable morbidity and mortality. Heart failure as primary diagnosis accounts for 1–2% of the annual healthcare budget in Europe and the USA. 1 The global economic burden of heart failure is estimated at $US108bn per annum with hospital admission being a key economic driver. 2
Systematic reviews and meta-analyses of cardiac rehabilitation for heart failure have shown improvements in health-related quality of life (HRQoL) and reductions in re-hospitalisations and demonstrated potential cost-effectiveness.3,4 This existing evidence is based solely on hospital (or centre)-based cardiac rehabilitation programmes and the economic evaluation data are limited in both quantity and quality.3,4
In spite of national and international guidelines recommending cardiac rehabilitation for heart failure,5–7 less than 20% of heart failure patients in the UK are referred to cardiac rehabilitation and less than 15% currently participate in cardiac rehabilitation,8–10 prompting calls for alternative more accessible models of cardiac rehabilitation provision.8 REACH-HF (Rehabilitation EnAblement in CHronic Heart Failure) is a home-based cardiac rehabilitation programme delivered over 12 weeks by a trained healthcare professional for patients and their caregivers. Uniquely the REACH-HF intervention has been co-developed with patients, caregivers and clinicians to include core components of comprehensive cardiac rehabilitation, that is, education and psychological support, in addition to exercise training. 11 The REACH-HF randomised controlled trial compared the addition of REACH-HF intervention with usual care with usual care alone in patients with HFrEF across four UK sites. 12 At 12 months, the trial found that the REACH-HF intervention led to a statistically significant and clinically meaningful improvement in HRQoL with a reduction in total Minnesota Living with Heart Failure Questionnaire score of –5.7 points (95% confidence interval (CI): –10.6 to –0.7) and a non-significant reduction in the number of patients experiencing one or more hospital admissions (odds ratio: 0.56, 95% CI: 0.13 to 2.33). 13 Having estimated the average cost of REACH-HF delivery at £418 per patient, 13 we sought to assess whether the REACH-HF intervention is likely to be cost-effective for healthcare payers over the long-term.
We report the results of a model-based cost-effectiveness analysis that extrapolates the findings of the REACH-HF trial to estimate the long-term cost-effectiveness of REACH-HF intervention. We also report the long-term cost-effectiveness of home-based cardiac rehabilitation based on a meta-analysis of randomised trials.
Methods
This analysis was reported in accord with the Consolidated Health Economic Evaluation Reporting Standards statement 14 and the reference case of the UK National Institute for Health and Care Excellence (NICE). 15 The analyses were conducted from the perspective of the UK National Health Service (NHS) and Personal Social Services. We estimated the cost-effectiveness of REACH-HF plus usual care versus usual care alone and home-based cardiac rehabilitation plus usual care versus usual care alone, based on the estimated incremental cost per quality-adjusted life-year (QALY) – a cost-utility analysis.
Study population
Data were used from the REACH HF trial 13 where participants with HFrEF were recruited from primary and secondary care in four UK centres during 2015–2016 and were randomly assigned to the REACH-HF intervention plus usual care or usual care alone (current standard therapy in the UK for most patients with heart failure). 12 In the UK, only a minority of patients with heart failure receive cardiac rehabilitation and usual care in this trial was a no cardiac rehabilitation approach that included medical management according to national and local guidelines, including specialist heart failure nurse care. 13 Details of the REACH-HF intervention are presented elsewhere.12,13
Model structure
Consistent with the economic evaluation literature in heart failure, 16 a Markov cohort model (Supplementary Material Figure 1 online) was developed that captured the impact on hospital admissions, and a related increase in the mortality rate, for people with heart failure. In this case a cohort Markov model was considered appropriate since this estimates the average effect of the intervention on morbidity, mortality, cost and HRQoL. The model uses a lifetime horizon (follows patients from a starting age of 78 to age 100 years) and costs and QALYs were discounted at 3.5%. 15
The model consisted of three primary health states: (1) heart failure with no heart failure-related hospital admission, (2) heart failure with heart failure-related hospital admission, and (3) death. The model uses a one-month cycle length, in order to capture the effects of hospital admission events which are short term events but may recur several times in a year. Tunnel states are used in the model to reflect an increased mortality risk in the period (1–38 months) after hospital admission/discharge. Patients begin in a stable heart failure health state (heart failure with no heart failure-related hospitalisation). From this state, patients can either remain in the same state, or experience a heart failure-related hospitalisation or death. If the patients experience a heart failure-related hospitalisation, they automatically progress to the first of 38 post-hospitalisation tunnel states, where they will progress one state each month until month 38 post-hospitalisation, when they will return to the heart failure with no heart failure-related hospitalisation state. During the tunnel states, patients can also experience an additional hospitalisation or death at any time. The model was developed in Microsoft Excel and programmed in Visual Basic for Applications.
Model inputs
Model parameters and assumptions.
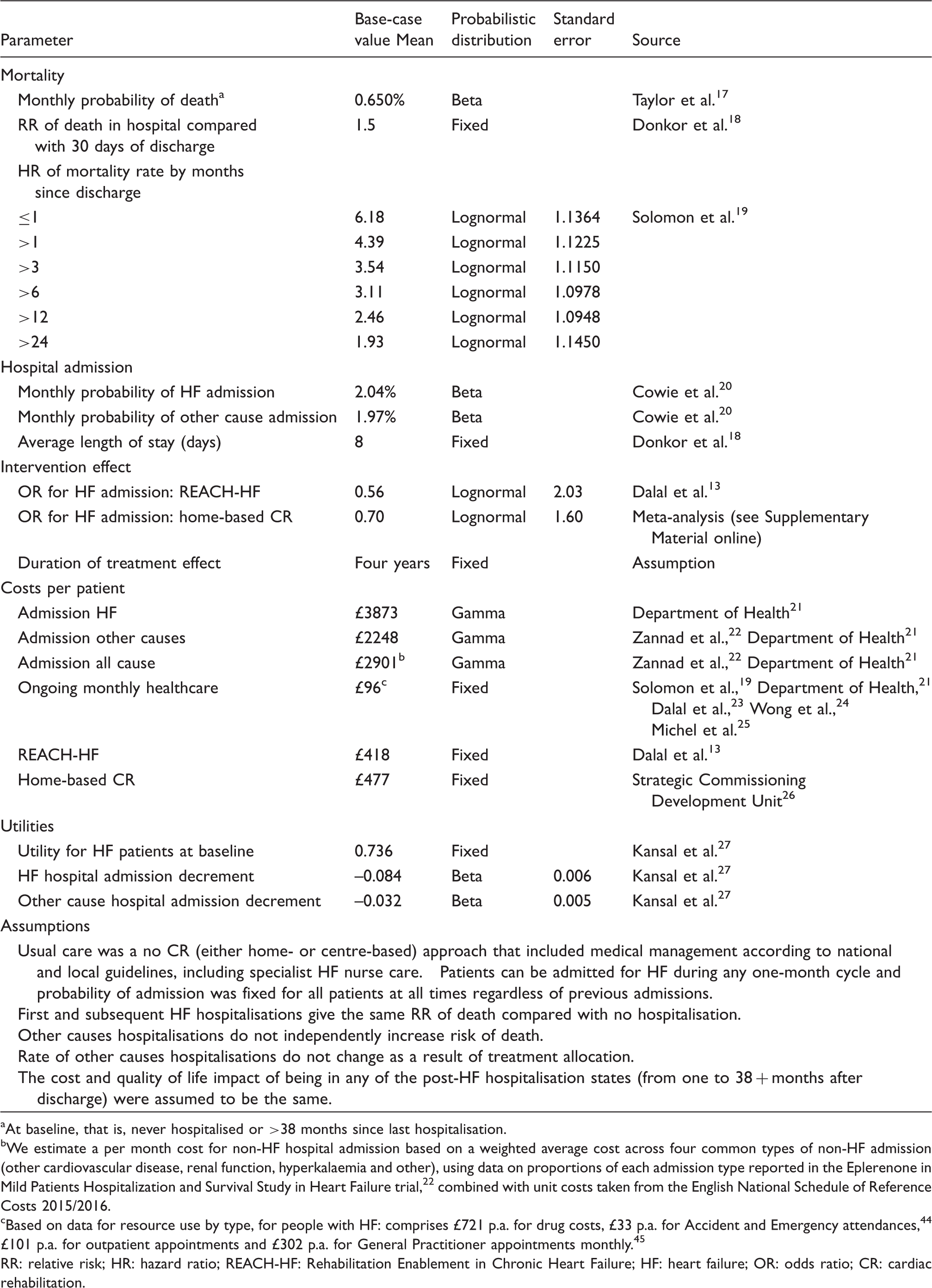
At baseline, that is, never hospitalised or >38 months since last hospitalisation.
We estimate a per month cost for non-HF hospital admission based on a weighted average cost across four common types of non-HF admission (other cardiovascular disease, renal function, hyperkalaemia and other), using data on proportions of each admission type reported in the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure trial, 22 combined with unit costs taken from the English National Schedule of Reference Costs 2015/2016.
Based on data for resource use by type, for people with HF: comprises £721 p.a. for drug costs, £33 p.a. for Accident and Emergency attendances, 44 £101 p.a. for outpatient appointments and £302 p.a. for General Practitioner appointments monthly. 45 RR: relative risk; HR: hazard ratio; REACH-HF: Rehabilitation Enablement in Chronic Heart Failure; HF: heart failure; OR: odds ratio; CR: cardiac rehabilitation.
Cardiac rehabilitation effectiveness
We used data from REACH-HF trial for the difference in risk of hospital admission (odds ratio: 0.56, 95% CI: 0.13 to 2.33). 13 We also undertook a meta-analysis that combined REACH-HF trial data with two other randomised trials of home-based cardiac rehabilitation versus no cardiac rehabilitation usual care28,29 to estimate the pooled risk of hospital admission following home-based cardiac rehabilitation compared with usual care (odds ratio: 0.70, 95% CI: 0.27 to 1.60) (see Supplementary Material Figure 1 for meta-analysis forest plot and methodology). This reduction in risk was assumed to last for four years from the start of the model, after which hospital admission rates are assumed to return to baseline. We assessed the impact on estimates of cost-effectiveness of variations in this assumption using sensitivity analyses.
Hospital admissions
We applied hospital admission data for heart failure-specific admissions from a UK cohort study reflective of a UK primary care setting, with patients experiencing both first and subsequent hospital admissions 20 (see Table 1). In sensitivity analyses, we tested the robustness of model outcomes to changes in hospital admission rates, using data from the UK Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS) trial, 22 which provided a lower estimate of admission rates (10% heart failure-related admissions; 20% all cause admissions per annum) and a meta-analysis of randomised trials 30 reporting relatively high admission rates (34% heart failure-related admissions; 85% all cause admission per annum). We used the same admission rate for all patients in the model irrespective of age and previous admissions.
Mortality
Survival parameters in the model are based on a recently published analysis of UK mortality rates in The Health Improvement Network (THIN) dataset, 1998–2012, 17 a retrospective cohort of 54,313 heart failure patients aged over 45 years. In a sensitivity analysis, we applied the overall survival reported by Mohiuddin et al. 31 for patients in another large UK cohort, who had already experienced a hospital admission for heart failure and therefore are expected to have a worse prognosis. This study showed increased risk for time since admission in people 0–1 months, 1–3 months, 3–6 months, 6–12 months, 12–24 months and 24–38 months after admission. The reported hazard ratios were applied in the model.
Mortality rates have been shown to vary with hospital admission and after discharge both in trials 19 and in the wider UK heart failure population, 18 with those in hospital and closer to discharge having higher death rates. Following the approach of Thokala et al., 32 we reflected this in the model using the hazard ratio for all-cause mortality reported by Solomon et al. 19 for patients within 1–>24 months from discharge for their heart failure hospital admission. For hospital mortality, we derived a hazard ratio for survival for patients in hospital compared with within 30 days of discharge from the UK Heart Failure Audit, 18 which reports outcomes from data on more than 73% of all English and Welsh heart failure admissions. We calibrated the baseline mortality rate so that the overall survival curves generated by the model matched the survival curves based on parameters taken from the THIN analysis. 30 We conservatively assumed that the hazard ratio of death for subsequent hospital admissions was the same as for the first hospital admission. We assumed that survival followed an exponential curve, which has previously been shown to provide a good fit in this population.31,33
Costs
Costs were included in pounds sterling using the 2015/2016 price year. The following costs were considered: (i) home-based cardiac rehabilitation, (ii) costs associated with heart failure hospital admission, (iii) costs associated with other cause hospital admission, and (iv) primary and secondary usual health care costs (excluding hospital admission) associated with heart failure (see Table 1). For intervention cost we use the UK NHS tariff for cardiac rehabilitation of £477/patient) 26 and the estimated cost for delivery of the REACH-HF intervention of £418/patient. 13 This cost was applied to all patients at the start of the model. Ongoing costs for usual care for heart failure, primary care, secondary care, Accident & Emergency department attendances and drug costs are included for time spent in the heart failure non-hospital admission state (£815/patient per year), informed by UK national data for heart failure and the THIN dataset, a large UK heart failure cohort study. 17
The cost for hospital admission is based on data from the English NHS National Schedule of Reference Costs 2015/2016; 26 for heart failure hospital admission we use a weighted average cost of a single hospital stay for the health resource groups EB03A to D. The cost of non-heart failure hospital admissions is a background cost in each cycle of the model, where patients are alive with heart failure. We discounted costs and QALYs at an annual rate of 3.5% in accord with the NICE reference case. 15
Health state values
We calculated QALYs by multiplying the health value for the state by the time spent in that state. We use data from the Systolic Heart failure treatment with the inhibitor ivabradine Trial (SHIFT) to inform health state values, applying a health state value of 0.736 for the heart failure health state, and a reduction (decrement) of 0.084 where people experience a heart failure-related hospital admission. 27 For non-heart failure hospital admissions, we apply a decrement of 0.032 for events. The impact of hospital events on health state values is applied for the one-month cycle of hospital admission after which individuals were assumed to return to baseline values. Data from the SHIFT trial were considered to be the most appropriate for our model given the reporting of EQ-5D data for the heart failure state and separately for a heart failure-specific hospital admission.
Analysis
We present deterministic estimates of the cost per QALY gained and use probabilistic sensitivity analysis and the incremental net monetary benefit (iNMB) approach34,35 to address uncertainty around the results. The iNMB approach uses parameters representing the maximum amount that the Payer (i.e. NHS) is ‘willing to pay’ to gain one QALY. We conservatively used the lower NICE threshold value of £20,000 per QALY gained in calculating iNMB. 15 An iNMB value > 0 would indicate that the intervention (home based cardiac rehabilitation) is cost-effective. The cost-effectiveness acceptability curve demonstrates how the willingness-to-pay threshold affects the probability that the intervention is considered cost-effective. 35 Monte Carlo simulation was used to draw a randomly selected estimate of each model parameter from the distributions described in Table 1 and to calculate the iNMB. Beta distributions represent the uncertainty in the probability parameters (mortality, hospital admission) and parameters for health state values because these values are typically bounded at zero and one. Log-normal distributions were used to estimate uncertainty in hazard rates and ratios. We used 5000 iterations to empirically estimate the uncertainty surrounding the mean iNMB.
The key element of structural uncertainty identified was heart failure-related mortality rates during admission and after discharge from hospital. This mechanism allows any reductions in admission rate brought about by the intervention to reduce overall mortality in the cohort, with related cost savings and QALY gains estimated. To test how sensitive the results are to the inclusion of this element of model structure we included a sensitivity analysis which uses a base mortality rate (from the THIN cohort 17 ) for all patients at all times, regardless of hospital admission (SA1).
In addition, we included further deterministic analyses to test how sensitive the results were to the choice of parameter as follows: the lowest hospital admission rate from trials identified as sources of heart failure-specific admission (0.88% probability of admission per month, based on the EMPHASIS trial 22 (SA2); the higher hospital admission rate from a large meta-analysis of trials (2.83% probability of admission per month 30 (SA3); survival based on previously-admitted patients in the large combined data in Hospital Episode Statistics and Office of National Statistics dataset 31 (SA4); lower mean intervention cost of £204/patient, based on the lower bound of the 95% CI around estimated cost for REACH-HF intervention (SA5); higher mean intervention cost of £730, based on the upper bound of the 95% CI around estimated cost for the REACH-HF intervention; 13 and assumption for home-based cardiac rehabilitation effect duration, at two years (SA7).
Results
Base-case analysis
REACH-HF intervention
Results of cost-effectiveness analyses: REACH-HF intervention and home-based CR versus usual care.
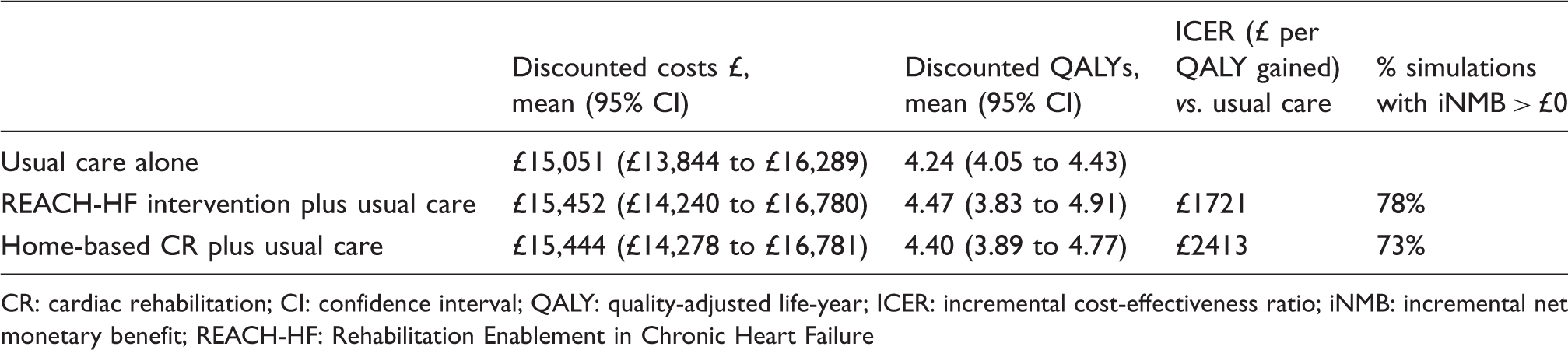
CR: cardiac rehabilitation; CI: confidence interval; QALY: quality-adjusted life-year; ICER: incremental cost-effectiveness ratio; iNMB: incremental net monetary benefit; REACH-HF: Rehabilitation Enablement in Chronic Heart Failure
Home-based cardiac rehabilitation
The estimated mean gain in QALYs for home-based cardiac rehabilitation compared with usual care was 0.16, and the estimated mean incremental cost is £383/patient over the lifetime, giving an estimated incremental cost ratio of per £2413 per QALY (Table 2). There was 73% probability that home-based cardiac rehabilitation was cost-effective compared with usual care, at £20,000/QALY gained (Supplementary Figure 3(b)).
Sensitivity analyses
Sensitivity analyses (Supplementary Table 1(a) and (b)) indicate the base-case analyses to be robust and not sensitive to changes in key structural assumptions in the modelling framework or key input parameters (i.e. mortality effect of hospital admission, probability of hospital admission, probability of mortality, home-based cardiac rehabilitation, duration of treatment effect) for both REACH-HF and home-based cardiac rehabilitation. Removing the increase in risk of mortality after hospital admission (SA1) resulted in home-based cardiac rehabilitation dominating usual care, with a reduction in costs (cost saving) and no difference in QALYs. In this scenario, although QALY gains are reduced, the costs associated with home-based cardiac rehabilitation also reduce due to the absence of an extended period of life expectancy and the absence of the additional costs associated with extending lives in the home-based cardiac rehabilitation group.
Discussion
Our estimates suggest that the addition of REACH-HF intervention home-based cardiac rehabilitation to usual care was cost-effective compared with usual care alone in patients with HFrEF at a cost of £1721/QALY and a 78% likelihood of being cost-effective at the willingness to pay threshold of £20,000 per QALY gained used by policymakers in UK and many developed health-care economies.15,36 Our cost-effectiveness estimates for other home-based cardiac rehabilitation programmes were similar. Our results were mainly driven by a reduction in heart failure-related hospitalisations with cardiac rehabilitation.
Two recent systematic reviews of cost-effectiveness of cardiac rehabilitation have been published.4,37 Based on the results of these reviews, this is the first published full economic evaluation of a specific home-based programme (REACH-HF) and home-based cardiac rehabilitation programmes more broadly in patients with heart failure. However, our findings are consistent with previously economic evaluations in heart failure comparing centre-based cardiac rehabilitation with no-cardiac rehabilitation control. Using extrapolated outcome survival data from a single centre randomised controlled trial, Georgiou and colleagues reported an incremental cost-effectiveness ratio of US$2500 per life-year gained for an exercise training programme at a 10-year time horizon based on the US healthcare perspective. 38 Using a variety of modelling assumptions and data at 2.5 years' follow-up from the large HF-ACTION trial undertaken across 82 centres across the USA, Canada and France, Reed et al. estimated that the cost-effectiveness of exercise training could vary from dominant (cost saving and more QALYs gained) to US$43,141/QALY. 39 Based on data from an exercise-based cardiac rehabilitation programme in Colombia, using modelling, Rincón et al. estimated an incremental cost per QALY of US$1065/QALY at five years. 40 Finally, a Markov model-based analysis by Kühr et al. reported a cost per QALY of 29,498 international dollars for a hypothetical cohort of heart failure patients attending an outpatient cardiac rehabilitation programme from the perspective of the Brazilian Public Healthcare System over a 10-year time horizon. 41 Notwithstanding the challenge of directly comparing costs across international jurisdictions and whilst these incremental cost effectiveness ratios vary in their magnitude, they have broadly been interpreted by study authors as demonstrating cardiac rehabilitation to be a cost-effective strategy in patients with HFrEF.
Although not recruiting heart failure patients, the recently published FIT@Home study also showed that home-based cardiac rehabilitation can be a cost-effective strategy. 42 This study randomised 90 low to moderate risk patients following an acute coronary syndrome or revascularisation to three months of either home-based training with telemonitoring guidance or centre-based training. Average healthcare costs were lower in the home-based group (€437 per patient) and had probability of being cost-effective of 97% and 75% at willingness-to-pay of €0 and €100,000 per QALY, respectively.
Strengths and limitations
This study uses cost and outcome data from a high quality multicentre randomised controlled trial of REACH-HF in patients with HFrEF with multiple comorbidities reflective of the clinical setting. 13 The use of Markov modelling overcomes the limitations of a within trial economic evaluation, allowing the modelling of costs and outcomes over the longer term of patient lifetime and the assessment of the long-term cost effectiveness beyond the trial period. The use of longer time-horizons is also more compatible with the chronic nature of heart failure and in accord with NICE methodology guidance. 15 We use high quality data on mortality from a large cohort study consistent with the setting for our economic analysis. Given the variation of hospital admission data, we use a UK dataset in our base-case analysis. However, use was made of alternative data sources in sensitivity analyses.
A key limitation was that the REACH-HF trial was not powered to detect differences in hospitalisations between arms. However, we sought to overcome this by undertaking a meta-analysis where we included data from two other randomised trials that tested different versions of home-based cardiac rehabilitation. Furthermore, our probabilistic sensitivity analysis explicitly took account of the uncertainty in the data inputs to the model. Nevertheless, future trials of cardiac rehabilitation need to consistently collect and report the outcome of patient hospitalisation. We used a simple Markov modelling approach, and whilst this approach is consistent with the wider literature on economic models in heart failure, we acknowledge it assumes no additional impact from multiple admissions. Whereas in real life patients may suffer from worsening HRQoL after further subsequent hospital stays, this conservative assumption may have led us to underestimate the cost-effectiveness of REACH-HF and home-based cardiac rehabilitation. We use heart failure-related hospital admissions as the main event of interest in the assessment of home-based cardiac rehabilitation. The absence of any specific modelling of effects on other (non-heart failure specific) cause of hospital admissions may be a limitation of the modelling, although is also likely due to a conservative assumption as cardiac rehabilitation may positively impact on the risk of admissions due to other cardiovascular related events, such as myocardial infarction or stroke.
Clinical implications
This cost-utility analysis indicates that the REACH-HF intervention and home-based cardiac rehabilitation programmes are likely to be cost-effective for patients for HFrEF. These economic results have considerable policy relevance given current low levels of uptake of cardiac rehabilitation for heart failure across international healthcare systems. 43 In order to improve cardiac rehabilitation participation there have been calls for the development of cardiac rehabilitation programmes that provide an alternative to supervised outpatient programmes, such as home-based programmes.8,9,23 The results of this analysis are therefore timely and show that home-based cardiac rehabilitation programmes provide a cost-effective alternative use of healthcare resources. The systematic review of home versus centre-based cardiac rehabilitation by Wong et al. concluded that as costs and outcomes of home-based versus supervised centre-based CR were no different, the choice of the mode of delivery (home- versus centre-based) should be left to healthcare providers and patients. 24 This is further reinforced by the recently updated UK clinical guidelines for the management of heart failure, that patients should be offered CR ‘in a format and setting (at home, in the community or in the hospital) that is easily accessible for the person’. 7
Conclusion
Over the lifetime of the HFrEF patient, our cost-utility analyses suggest that REACH-HF and home-based cardiac rehabilitation are cost-effective treatment options in the setting of the UK health service. These findings should encourage healthcare providers and purchasers to fund home-based cardiac rehabilitation programmes to improve access and promote participation in cardiac rehabilitation for people with heart failure and thereby improve the HRQoL and morbidity of this population.
Supplemental Material
Supplemental material for The cost effectiveness of REACH-HF and home-based cardiac rehabilitation compared with the usual medical care for heart failure with reduced ejection fraction: A decision model-based analysis
Supplemental Material for The cost effectiveness of REACH-HF and home-based cardiac rehabilitation compared with the usual medical care for heart failure with reduced ejection fraction: A decision model-based analysis by Rod S Taylor, Susannah Sadler, Hasnain M Dalal, Fiona C Warren, Kate Jolly, Russell C Davis, Patrick Doherty, Jackie Miles, Colin Greaves, Jennifer Wingham, Melvyn Hillsdon, Charles Abraham, Julia Frost, Sally Singh, Christopher Hayward, Victoria Eyre, Kevin Paul, Chim C Lang and Karen Smith in European Journal of Preventive Cardiology
Footnotes
Author contribution
HMD, RST, KJ, RCD, PD, JM, JW, NB, CG, CA and SSi obtained the funding for the study. SSa undertook the economic modelling analysis, RST undertook the meta-analysis, and both jointly drafted the manuscript. All authors commented on the manuscript and agreed the final version.
Acknowledgements
The following are these authors’ current affiliations: RST: Institute of Health and Well Being, School of Medicine, Dentistry & Nursing, University of Glasgow, UK; CG: School of Sport, Exercise and Rehabilitation Sciences, University of Birmingham, Edgbaston, UK; CA: School of Psychological Sciences, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Parkville, Australia. We thank all REACH-HF study participants, facilitators, clinicians, researchers and administrators who contributed data or their expert opinion and advice to the study in Birmingham, Cornwall, Exeter, Gwent, York, Heart Manual Department NHS Lothian (Carolyn Deighan, Louise Taylor and Jenny Elliott), Peninsula Clinical Trials Unit, Royal Cornwall Hospitals Trust (Research, Development and Innovation and Clinical Chemistry departments), PPI Advisory Group (Kevin Paul (Chair)), Programme Steering Committee (Martin Cowie (Chair), Graham Dunn, Suzanna Hardman, Roger Boyle, and Liz Clark), Data Monitoring Committee (Ann Dorthe-Zwisler (Chair), Alan Montgomery and Gill Furze), and independent adjudicators (Iain Squire, Sern Lim and Paco Leyva).
Declaration of conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the United Kingdom’s National Institute for Health Research (NIHR) Programme Grants for Applied Research (grant number RP-PG-1210-12004). RST and Britten are part-funded by the National Institute for Health Research (NIHR) Collaboration for Peninsula Leadership in Applied Health Research and Care. KJ is part-funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) West Midlands. SSi is supported by NIHR CLARCH East Midlands. The funders’ peer-review process informed the trial protocol. The sponsor of the trial had no role in trial design, data collection, data analysis, data interpretation, or writing of the report. The views expressed in this publication are those of the authors and not necessarily of the NIHR or United Kingdom’s Department of Health and Social Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.