
Abstract
Background
The prevalence of undetected left ventricular diastolic dysfunction is high, especially in the elderly with comorbidities. Left ventricular diastolic dysfunction is a prognostic indicator of heart failure, in particularly of heart failure with preserved ejection fraction and of future cardiovascular and all-cause mortality. Therefore we aimed to develop sex-specific diagnostic models to enable the early identification of men and women at high-risk of left ventricular diastolic dysfunction with or without symptoms of heart failure who require more aggressive preventative strategies.
Design
Individual patient data from four primary care heart failure-screening studies were analysed (1371 participants, excluding patients classified as heart failure and left ventricular ejection fraction <50%).
Methods
Eleven candidate predictors were entered into logistic regression models to be associated with the presence of left ventricular diastolic dysfunction/heart failure with preserved ejection fraction in men and women separately. Internal-external cross-validation was performed to develop and validate the models.
Results
Increased age and β-blocker therapy remained as predictors in both the models for men and women. The model for men additionally consisted of increased body mass index, moderate to severe shortness of breath, increased pulse pressure and history of ischaemic heart disease. The models performed moderately and similarly well in men (c-statistics range 0.60–0.75) and women (c-statistics range 0.51–0.76) and the performance improved significantly following the addition of N-terminal pro b-type natriuretic peptide (c-statistics range 0.61–0.80 in women and 0.68–0.80 in men).
Conclusions
We provide an easy-to-use screening tool for use in the community, which can improve the early detection of left ventricular diastolic dysfunction/heart failure with preserved ejection fraction in high-risk men and women and optimise tailoring of preventive interventions.
Keywords
Introduction
Left ventricular diastolic dysfunction (LVDD), a functional cardiac abnormality, is characterised by the impairment of left ventricular (LV) relaxation and increased LV stiffness and is the dominant underlying feature of heart failure with preserved ejection fraction (HFpEF).
The prevalence of undetected LVDD is high in the community with estimates exceeding 30% in population-based studies among adults.1,2 Recognising LVDD is important as not only is it known to be independently associated with the development of heart failure (HF),3,4 but it is also known to be predictive of cardiovascular and all-cause mortality.5,6 Therefore early recognition and implementation of management strategies could potentially play a major role in improving prognosis. To assess LVDD, the latest European Society of Cardiology (ESC) guidelines suggest the use of various structural/functional echocardiographic measures including the left atrial volume index (LAVI), E/e′ and longitudinal strain. 6 However such measurements are not feasible in all community-dwelling men and women due to high costs and time pressures. Currently, there are models available for the prediction of all-type HF, highlighting the importance of history taking and physical examination as well the use of N-terminal pro b-type natriuretic peptide (NTproBNP). 7 A practical model to predict LVDD (with or without symptoms (HFpEF)) does not exist; previous studies that examined predictors of LVDD lacked clinical variables and only included echocardiographic parameters, and are therefore not applicable for use in the community as a risk assessment tool to assess who should undergo echocardiography or not.1,8
Previous HF-screening trials focused on a combination of high-risk patients from the community such as the St Vincent's Screening TO Prevent Heart Failure (STOP-HF) trial which included participants with at least one risk factor such as hypertension and hypercholesterolemia. 9 This trial demonstrated a reduction in newly diagnosed HF and LV dysfunction (both diastolic and systolic) following intervention with cooperative cardiological management and intensified use of renin-angiotensin blockers and β-blocker therapy. Therefore, given the relevance of screening high-risk populations, we aimed to develop and validate a risk prediction model for LVDD/HFpEF using four HF-screening studies performed in high-risk individuals from the community aged 60 or 65 years and over. Given that evidence is accumulating regarding determinants of LVDD/HFpEF differing according to sex, this was performed separately for men and women. With this information, preventative strategies within the community can be tailored towards these high-risk individuals.
Methods
Study population
Four previously published studies performed in a primary care setting among high-risk community people aged 60 or 65 years or older (STRETCH, TREE, UHFO-COPD, and UHFO-DM) were combined into one individual patient dataset (IPD).10–13 For a description of the four cohorts see Supplementary Material Figure 1. All of these studies had a common aim to screen for previously unknown, all-type HF. The studies consisted of older people with either (a) symptoms of shortness of breath on exertion, 10 (b) multimorbidity or polypharmacy, 11 (c) chronic pulmonary obstructive disease (COPD), 12 or type 2 diabetes (T2D). 13 Data in all cross-sectional diagnostic studies were collected from all participants using the same uniform case record form with questions regarding symptoms, drug use, medical history, evaluation of physical signs, additional investigations with electrocardiography, B-type natriuretic peptide testing and echocardiography.
Outcome, diagnostic predictors and model development
The outcome of HF or no HF, was established by an expert panel as described previously.10–13 In cases with HF, the panel chose between HFpEF, heart failure with reduced ejection fraction (HFrEF), and isolated right-sided HF, primarily based on ejection fraction (cut-point 45%) and estimated pulmonary artery pressures. Natriuretic peptide measurements were used as an inclusion criterion for echocardiography in the STRETCH cohort, applying a cut-off point of NTproBNP level above 125 pg/ml (≈15 pmol/l). 6 The panel also assessed NTproBNP levels in the TREE cohort prior to diagnosis. The panels were not privy to the NTproBNP levels in the UHFO-COPD and UHFO-DM cohorts, thereby preventing incorporation bias for this variable in these two cohorts. 14 The reproducibility of this panel consensus method has been shown to be high (mean inter-agreement with re-evaluation of a random sample of 10% of the cases; K = 0.84 (Rutten K = 0.90, Mourik K = 0.74, van Riet K = 0.89, Boonman K = 0.82)). Only patients who underwent Tissue Doppler imaging (TDi) were selected for the current study (Supplementary Material Figure 1). All studies measured the early diastolic lengthening velocities (e′) at the septal and lateral side and took the average, except the UHFO-DM study which only examined the septal side. We redefined patients with HF according to the recent 2016 ESC guidelines on HF into HFrEF, heart failure with midrange ejection fraction (HFmrEF) and HFpEF using the cut-points of left ventricular ejection fraction (LVEF) of 40% and 50%. According to this definition, patients diagnosed with HFrEF (n = 36, HF symptoms and LVEF <40%) and HFmrEF (n = 52, HF symptoms LVEF 40–49%) were removed, leaving 1371 patients in the current study.
Structural and functional abnormalities seen in LVDD were assessed non-invasively by echocardiography including measurements with TDi. LVDD was defined in line with the recommendations from the 2012 and 2016 ESC guidelines on HF,
6
and also published by Paulus et al.
15
as E/e′ above 13 or an E/e′ between 8–13 with at least one or more of the following:
– LAVI > 34 ml/m2 – Left ventricular mass index (LVMI) > 115 mg/m2 for males or >95 mg/m2 for females – Atrial fibrillation (AF) on the electrocardiogram (ECG) – NTproBNP level>125 pg/ml.
Those defined as having LVDD, therefore, have a LVEF ≥ 50% and contain asymptomatic participants as well as individuals with HF symptoms and thus may also be identified as HFpEF. The outcome was subsequently defined as those who fulfilled the criteria for LVDD (including those with symptoms of HF and thus HFpEF according to an expert panel) versus those without LVDD (and in view of the exclusion criteria) without LVSD/HFrEF/HFmrEF).
We evaluated, in a multivariable manner, 11 potential diagnostic predictors from previous literature, known to predict, at least univariably, diastolic dysfunction.1,5,8,16,17 These were; age, a history of ischaemic heart disease (IHD), AF, hypertension, T2D, angina pectoris, shortness of breath at least when walking at a normal pace (MRC ≥ 3), ankle oedema, pulse pressure, body mass index (BMI), and the use of β-blocker therapy.
Data analysis
We aimed to derive four diagnostic models: first, a clinical model for men and women separately with all the aforementioned variables and excluding NTproBNP, and a second, extended model, again separately for men and women, including all independent variables with the addition of NTproBNP. From the candidate diagnostic predictors, we selected those that were important in predicting the presence of LVDD/HFpEF in men and women separately following the Akaike information criteria (AIC) in a multivariable logistic regression model. NTproBNP was log-transformed for all analyses.
A summary of the missing values is displayed in Supplementary Material Table 2. Missing values in each dataset set were imputed five times separately for men and women using the MICE algorithm in R. 18
In all analyses a linear relationship between the outcome LVDD/HFpEF and the continuous predictors age, BMI and log NTproBNP value was assumed and checked. There was no collinearity between variables. Data was analysed using R version 3.3.2. 19
The internal-external cross validation (IECV) method was used for model development and validation. This method was recently recommended by Steyerberg and Harrell for use when combining individual patient data from multiple studies. 20 Further details can be found in the Supplementary Material.
The performance of the models was quantified by examining discrimination and calibration.
A risk score was constructed for both men and women separately from the final models, multiplying the shrunken coefficients by two and then rounding to the nearest integer. A dummy variable was added representing whether a participant came from the TREE cohort, the highest risk population, i.e. with three or more chronic or vitality threatening diseases and/or using five or more prescribed drugs daily during the past year in people aged 65 years, to account for differences in prevalence and therefore baseline risk of LVDD/HFpEF. The risk of LVDD/HFpEF was then calibrated using logistic regression modelling according to the scores, resulting in a corresponding risk for each score, which was presented graphically. The total range of scores was divided by three to create different risk groups; mild, moderate and high. The participants were then allocated a particular group depending on their summed score.
Results
Baseline patient characteristics of the 1371 elderly participants divided over each cohort and stratified by sex.
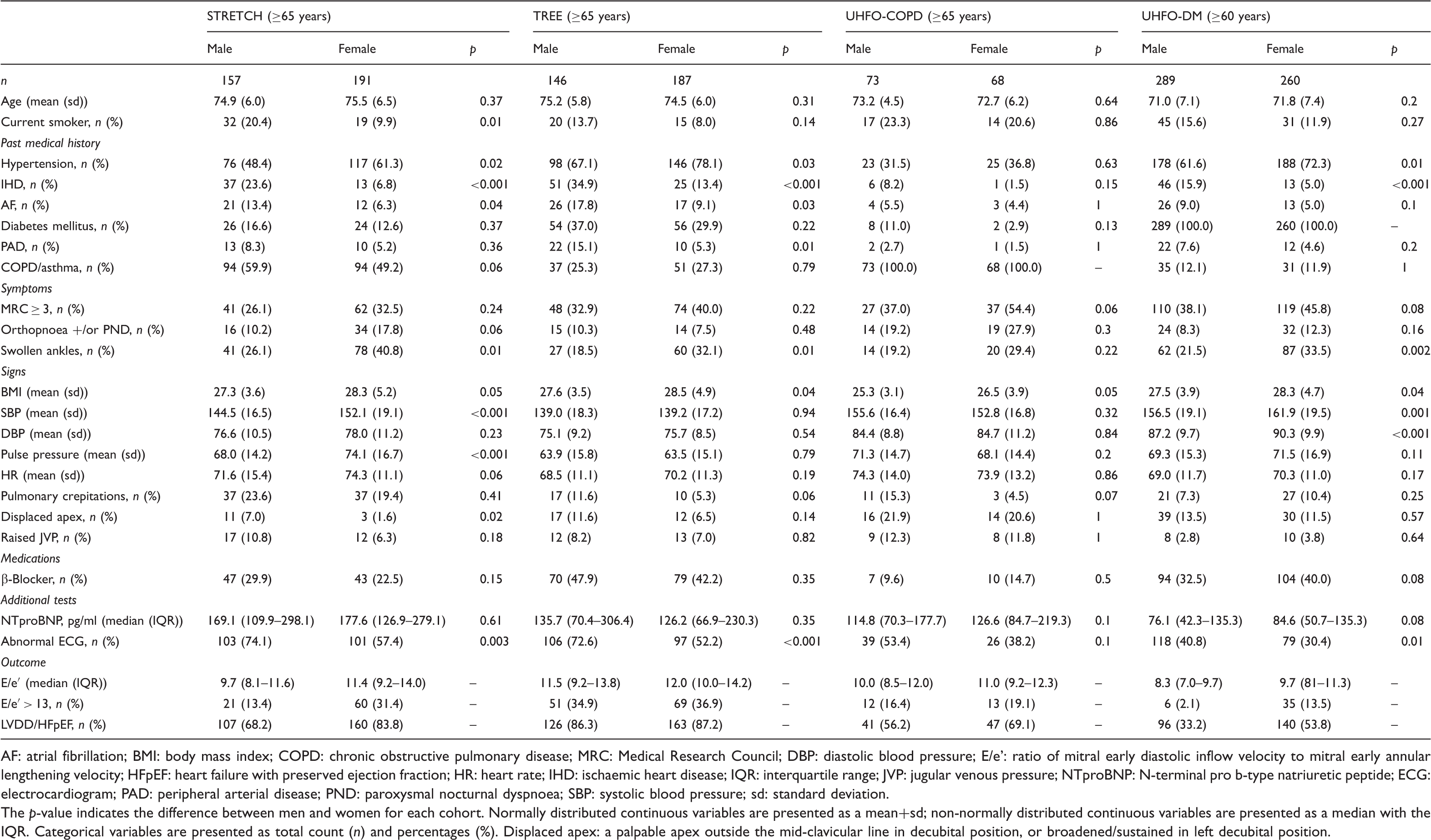
AF: atrial fibrillation; BMI: body mass index; COPD: chronic obstructive pulmonary disease; MRC: Medical Research Council; DBP: diastolic blood pressure; E/e’: ratio of mitral early diastolic inflow velocity to mitral early annular lengthening velocity; HFpEF: heart failure with preserved ejection fraction; HR: heart rate; IHD: ischaemic heart disease; IQR: interquartile range; JVP: jugular venous pressure; NTproBNP: N-terminal pro b-type natriuretic peptide; ECG: electrocardiogram; PAD: peripheral arterial disease; PND: paroxysmal nocturnal dyspnoea; SBP: systolic blood pressure; sd: standard deviation.
The p-value indicates the difference between men and women for each cohort. Normally distributed continuous variables are presented as a mean+sd; non-normally distributed continuous variables are presented as a median with the IQR. Categorical variables are presented as total count (n) and percentages (%). Displaced apex: a palpable apex outside the mid-clavicular line in decubital position, or broadened/sustained in left decubital position.
Selection of clinical predictors from the 11 candidate predictors for men and women.
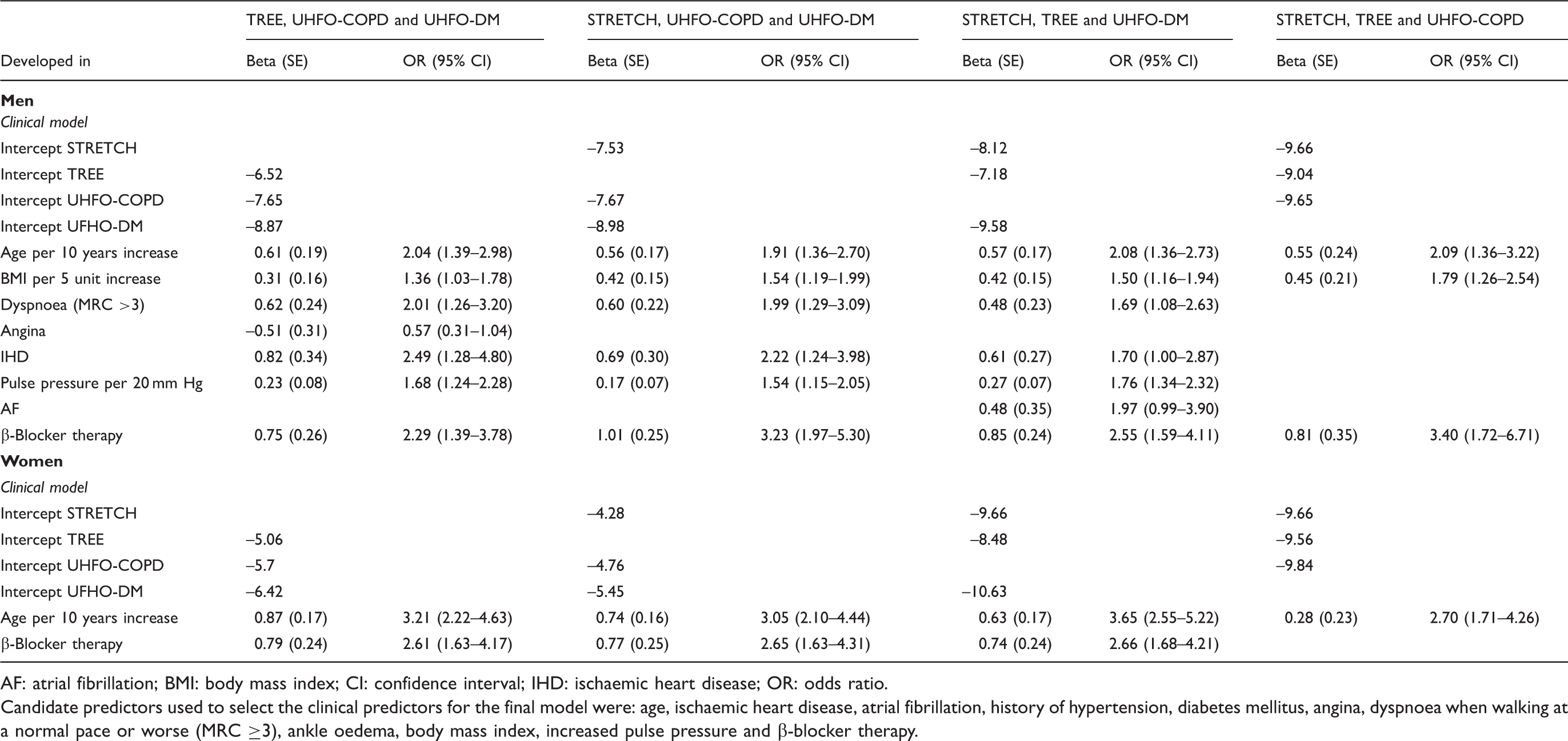
AF: atrial fibrillation; BMI: body mass index; CI: confidence interval; IHD: ischaemic heart disease; OR: odds ratio.
Candidate predictors used to select the clinical predictors for the final model were: age, ischaemic heart disease, atrial fibrillation, history of hypertension, diabetes mellitus, angina, dyspnoea when walking at a normal pace or worse (MRC ≥3), ankle oedema, body mass index, increased pulse pressure and β-blocker therapy.
Discrimination of the models was similar between men and women. Discrimination of the male model (consisting of increased age, increased BMI, shortness of breath when walking at a normal pace or worse (MRC ≥3), increased pulse pressure, a history of IHD and β-blocker therapy) ranged at cross-validation from area under the curve (AUC) 0.60–0.75 (Supplementary Material Table 4). Discrimination of the female model (consisting of only age and β-blocker therapy) ranged at cross-validation from AUC 0.51–0.76. The addition of NTproBNP to the models improved the performance in both men and women with AUCs in men ranging from 0.68–0.80 and in women from 0.61–0.80. Calibration of the models, as displayed by the observed/expected (OE) ratios (Supplementary Material Table 4) and visualised with calibration plots (Supplementary Material Figure 2) was better in women than men but improved in both men and women following the addition of NTproBNP to the models.
The corresponding bootstrap corrected c-statistic of the final model for all four cohorts combined in men was 0.66 (95% confidence interval (CI) 0.62–0.69) for the clinical model and 0.80 (95% CI 0.77–0.84) for the extended model with the addition of NTproBNP. For women, the corresponding bootstrap corrected c-statistic of the final model was 0.58 (95% CI 0.54–0.62) for the clinical model and 0.78 (95% CI 0.74–0.81) for the extended model with the addition of NTproBNP.
Clinical scoring rule for (a) men and (b) women with and without N-terminal pro b-type natriuretic peptide (NTproBNP).
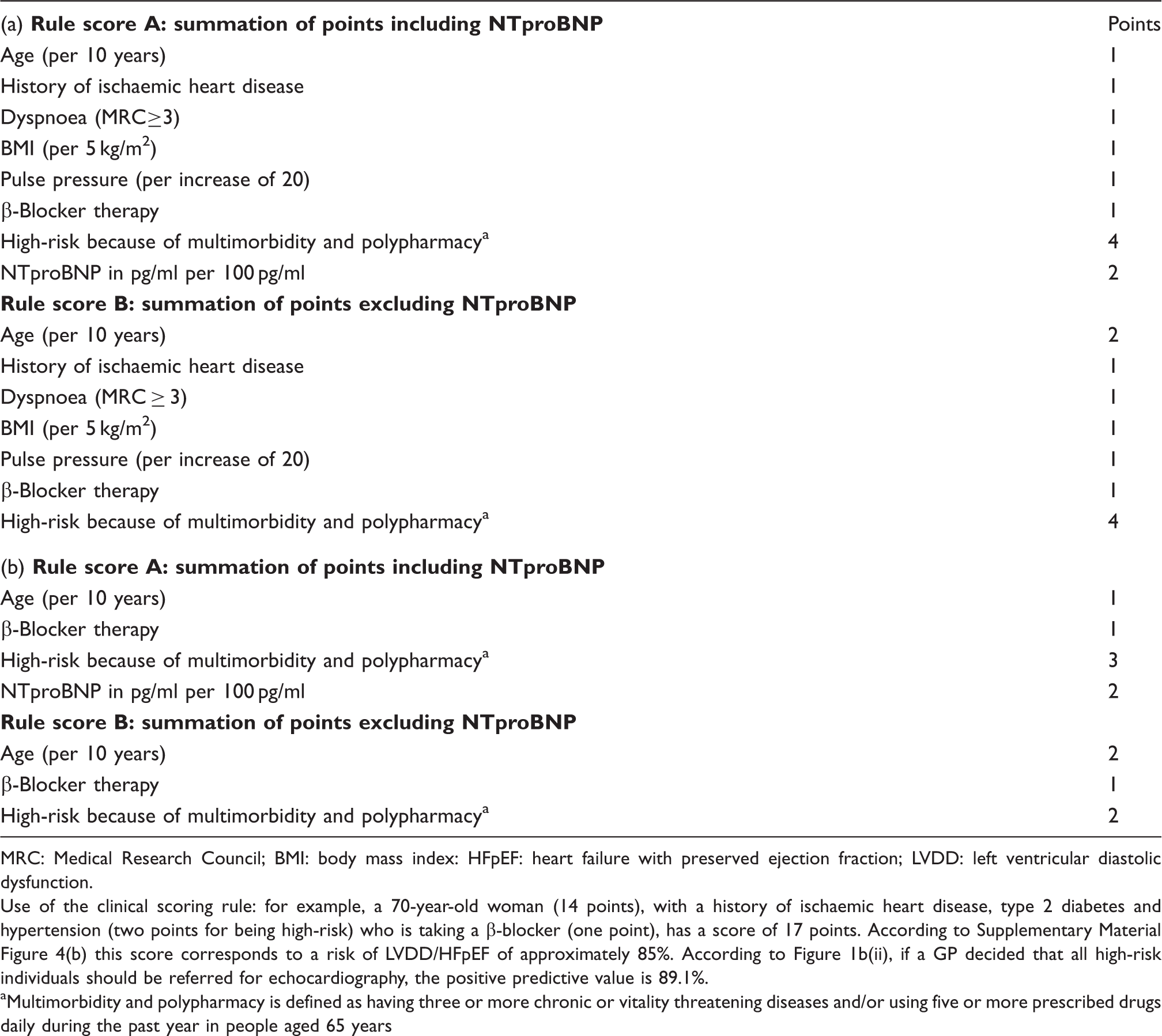
MRC: Medical Research Council; BMI: body mass index: HFpEF: heart failure with preserved ejection fraction; LVDD: left ventricular diastolic dysfunction.
Use of the clinical scoring rule: for example, a 70-year-old woman (14 points), with a history of ischaemic heart disease, type 2 diabetes and hypertension (two points for being high-risk) who is taking a β-blocker (one point), has a score of 17 points. According to Supplementary Material Figure 4(b) this score corresponds to a risk of LVDD/HFpEF of approximately 85%. According to Figure 1b(ii), if a GP decided that all high-risk individuals should be referred for echocardiography, the positive predictive value is 89.1%.
Multimorbidity and polypharmacy is defined as having three or more chronic or vitality threatening diseases and/or using five or more prescribed drugs daily during the past year in people aged 65 years
The performance of the female model using the additional male specific predictors in addition to age and β-blocker therapy (increased BMI, shortness of breath when walking at a normal pace or worse (MRC ≥ 3), increased pulse pressure, a history of IHD), as assessed by the bootstrap corrected c-statistic was 0.60 (95% CI 0.56–0.63) and with the addition of NTproBNP 0.78 (95% CI 0.74–0.81). Hence adding the additional predictors did not improve the performance significantly. The performance of male model using only the predictors remaining in the female model which were also present in the male model (age and β-blocker therapy) i.e. excluding the additional male-specific predictors, was 0.62 (95% CI 0.59–0.66) and with the addition of NTproBNP 0.80 (95% CI 0.76–0.83).
Using the risk scores to categorise men and women into low, moderate and high-risk categories (Figure 1), we show that with a cut-point of 22 or above, 34.7% of men are at high-risk of having LVDD/HFEF and thus should undergo echocardiography. Of these men, 88.8% will actually have confirmed LVDD/HFpEF. With a cut-point of above 14, 21.4% of women are categorised as being at high-risk of having LVDD/HFpEF, so should also undergo echocardiography. Of these women, 97.4% will have confirmed LVDD/HFpEF.
Application of the clinical prediction rule for (a) men and (b) women with (i) and without (ii) N-terminal pro b-type natriuretic peptide (NTproBNP). HF: heart failure; HFpEF: heart failure with preserved ejection fraction; LVDD: left ventricular diastolic dysfunction.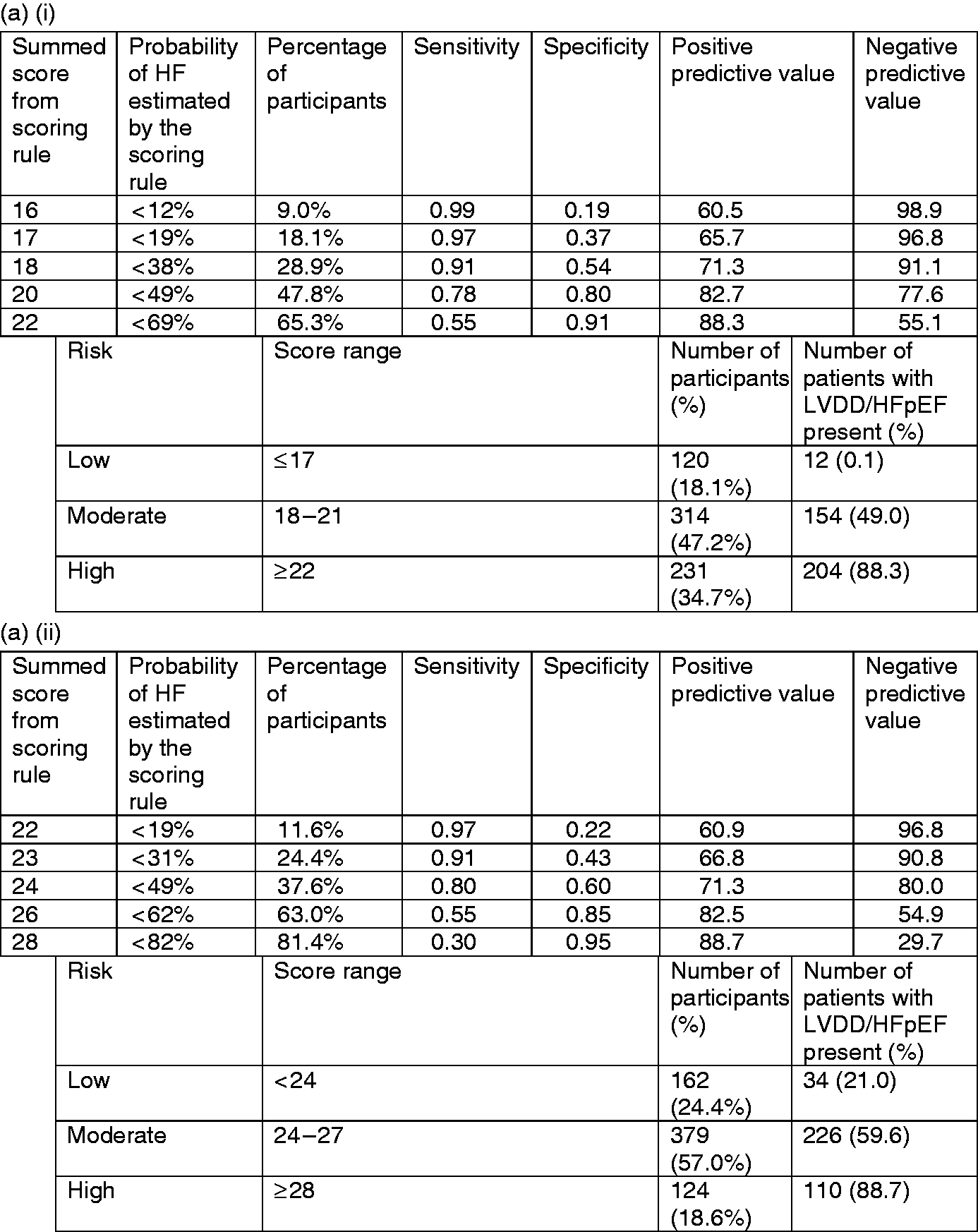
Discussion
We developed and validated the first sex-specific models for the prediction of LVDD/HFpEF among high-risk men and women over the age of 60 or 65 in four opportunistic HF screening cohorts in the community. The multivariable logistic models performed similarly in men and women and both sexes shared overlapping predictors, albeit with the model in women only containing two of the six independent predictors making up the male model (increased age and β-blocker therapy). The male model also consisted of history of IHD, shortness of breath when walking at a normal pace or worse (MRC ≥ 3), increased pulse pressure and increased BMI. Nevertheless, after applying the male model in females and visa versa, it is evident that age, β-blocker therapy and NTproBNP are the most important predictors in both men and women for predicting LVDD/HFpEF. The model accurately categorises 88.3% of high-risk men and 94.4% of high-risk women, according to the constructed risk scores, as having confirmed LVDD/HFpEF on echocardiography.
Age is a well-known determinant of LVDD/HFpEF and also of all-type HF, 16 being previously found to be a predictor of all-type HF in the community using the same four community cohorts used in this study. 21 Echocardiographic parameters used to define LVDD are affected by the effect of ageing on myocardial stiffness. 22 Also, increased BMI and IHD have previously been shown to be independent predictors of LVDD.23,24 Interestingly, we showed that these variables remained as independent predictors in a reduced model with backward regression only in men. β-Blocker therapy remained an independent predictor in both men and women. We subsequently evaluated a model containing only hypertension, angina, AF, history of IHD, as possible indications for β-blocker therapy use in addition to β-blocker therapy, and still showed an independent association between β-blocker therapy and LVDD/HFpEF in both men (OR 2.45 (95% CI 1.64–3.66)) and women (OR 1.74 (95% CI 1.14–2.64)), although these values were lower than with univariable analysis (OR 3.32 (95% CI 2.33–4.75) in men, OR 2.17 (95% CI 1.48–3.18) in women). However, whether the use of β-blockers is related to LVDD/HFpEF or their use is merely representative of the many indications including a history of IHD, angina pectoris, AF and other tachycardias, and hypertension, remains unclear.
The addition of NTproBNP to the models significantly improved the performance of the models in both men and women. This highlights the importance of NTproBNP, not only in diagnosing HFpEF but also for LVDD and, as previously shown, for all-type HF.6,7
We present the first models of their kind. We have previously presented a model to identify high-risk men and women of having all-type HF in the same studied community. 21 However this and other screening studies have not looked at LVDD/HFpEF in men and women separately from the community. Previous models also lacked external validation and incorporated echocardiographic parameters into the models and thus, because of logistic reasons and the costs involved, cannot be used in the community.1,8 A study by Ho et al. compared the prediction of HFrEF and HFpEF and found that increased age, increased BMI, antihypertensive treatment, and IHD were independent predictors of HFpEF in multivariable analyses in four combined general population studies. 17 Increased age, sex, increased systolic blood pressure, increased BMI, smoking status, antihypertensive treatment, LV hypertrophy, left bundle branch block, T2D, and previous myocardial infarction were predictive of HFrEF. It is not known how the antihypertensive treatment was defined and whether or not it included β-blocker therapy. They applied 45% as a cut-point between HFrEF and HFpEF, thus not considering HFmrEF. Although not clear, the authors may have analysed HFpEF vs no HF plus HFrEF, and HFrEF vs no HF plus HFpEF. It is important to highlight that we evaluated LVDD/HFpEF vs no LVDD/HFpEF in a population excluding LVSD/HFrEF and HFmrEF. Despite the differences in methodology, the results of the study by Ho et al. do show an overlap with our results concerning antihypertensive treatment as an independent predictor of LVDD/HFpEF in both men and women.
Community cohorts provide a wealth of patient information. Increasing the number of health care checks in primary care, taking into account any barriers in the way of patient access, can help identify men and women at risk of developing diseases such as LVDD/HFpEF. 25 With applying state-of-the art regression analysis we present models that have been externally validated representing the ‘real world’ population as our cohorts involve older men and women from the community who have a variety of different risk profiles, which is representative of the patients attending general practitioner clinics at high-risk of LVDD/HFpEF. Once patients have been identified at risk of having LVDD, management including treatment and preventative strategies can be implemented such as risk factor management such as adequate management of diabetes, hypertension and cardiac ischaemia, as recommended by the guidelines to prevent progression of the disease and to prevent LVDD from entering into the symptomatic phase, i.e. HFpEF. 6 These models can also be used to help identify low risk patients who do not require echocardiography limiting unnecessary cardiology and echocardiography referrals, reducing health-care costs and reducing demands on resources. Treatment with spironolactone has shown promise in reducing cardiovascular events in patients with HFpEF in the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial post-hoc analysis results of the American sub-set population, and in those with elevated natriuretic peptide levels.26,27 Thus, it is not only extremely helpful in relieving symptoms in these patients suffering from congestion, which is one of the primary goals of such patients, but it may also help improve outcomes. Other drugs such as empagliflozin show potential but the effect on cardiovascular outcomes will be determined in the near future following results of clinical trials. Therefore our models will be able to identify patients who would benefit from not only risk factor control and symptomatic relief with diuretics, but will also improve morbidity and prognosis of these patients. 28
Strengths and limitations
Our study consists of cohorts from the general population and are applicable to primary care settings. By excluding LVSD/HFmrEF/HFrEF instead of combining them with no HF we provide better predictions as we are able to discriminate between subjects with HFpEF and no HF. However an outcome ideally consisting of three categories; no HF, HFrEF and HFmrEF, and HFpEF would likely lead to a more informed clinical applicability. A limitation of our study is that participants of the STRETCH study only underwent echocardiography examination if they had an abnormal ECG and/or an NTproBNP >125 pg/ml. This criterion may have resulted in missing some participants with LVDD/HFpEF that were erroneously considered to have no structural or functional cardiac abnormalities. The prevalence estimate in that study may therefore be a little bit too high, but this is unlikely to affect the modelling and the related ORs, especially not when combining this study with the other three studies without such an exclusion criterion. Another limitation is that E/e′ was used to diagnose diastolic dysfunction although evidence backing up the use of resting E/e′ for left ventricular filling pressure remains limited. 29 Incorporation bias has been mentioned previously, as the expert panel on two out of the four cohorts were aware of the NTproBNP results when deciding on the diagnosis. It is important to realise that incorporation bias is inevitable in diagnostic modelling studies. 14 However, avoiding the use of the NTproBNP results in the panel diagnosis may lead to a worse problem; misclassification of patients. 14 It is also important to note that in our study the information obtained from echocardiography was not used in the formulation of the prediction models. Trials previously focusing on at-risk cohorts, such as the STOP-HF trial have found a reduction in HF onset therefore our high-risk cohorts provide a valid basis to screen for HF/LVDD. However, it is important to note that translation of such risk management strategies into routine primary care practices may be challenging.
In summary, we developed and externally validated sex-specific models for the prediction of LVDD/HFpEF in community-based high-risk older men and women. This unique early detection model will help to optimise tailoring of the required preventative interventions for LVDD/HFpEF.
Supplemental Material
Supplemental material for Opportunistic screening models for high-risk men and women to detect diastolic dysfunction and heart failure with preserved ejection fraction in the community
Supplemental Material for Opportunistic screening models for high-risk men and women to detect diastolic dysfunction and heart failure with preserved ejection fraction in the community by Aisha Gohar, Rogier F Kievit, Gideon B Valstar, Arno W Hoes, Evelien E Van Riet, Yvonne van Mourik, Loes C Bertens, Leandra J Boonman-Winter, Michiel L Bots, Hester M Den Ruijter and Frans H Rutten on behalf of the Queen of Hearts and the RECONNECT consortia in European Journal of Preventive Cardiology
Footnotes
Acknowledgements
A comprehensive list of investigators involved in the Queen of Hearts Consortium can be found at the following URL: http://www.queen-of-hearts.eu. A comprehensive list of investigators involved in the RECONNECT Consortium can be found at the following URL: ![]() .
.
Author contribution
AG, AWH, MLB, EEvR, YvM, LJBW and FHR contributed to the conception and design of the work. AWH, MLB, EEvR, YvM, LCB, LJBW, HMDR and FHR contributed to the acquisition, analysis, or interpretation of data for the work. AG drafted the manuscript. RFK, GBV, AWH, MLB, EEvR, YvM, LCB, LJBW, HMDR and FHR critically revised the manuscript. All authors gave final approval and agree to be accountable for aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All four studies were investigator-driven research projects, and Roche diagnostics was not involved in the design, execution or analysis of the study. None of the authors received personal payment from any industrial partner.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the Queen of Hearts Consortium and has been supported by a grant from the Netherlands Heart Foundation: 2013/T084. The individual studies used in this article were supported by unrestricted grants from Netherlands Heart Foundation (Nederlandse Hartstichting) (2009B048) (STRETCH), ZonMw grant no. 311040302 (TREE), the Netherlands Organisation for Scientific Research (NWO) (904-61-144) (UHFO-COPD), Fonds Nuts Ohra zorgsubsidies’ (grant no. 0702086) (UHFO-DM). Roche diagnostics delivered the NTproBNP assays for all four studies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.