
Abstract
Background
The association between physical activity and atrial fibrillation remains controversial. Physical activity has been associated with a higher and lower atrial fibrillation risk. These inconsistent results might be related to the type of physical activity. We aimed to investigate the association of total and types of physical activity, including walking, cycling, domestic work, gardening and sports, with atrial fibrillation.
Design
Prospective cohort study.
Methods
Our study was performed in the Rotterdam Study, a prospective population-based cohort. We included 7018 participants aged 55 years and older with information on physical activity between 1997–2001. Cox proportional hazards models were used to examine the association of physical activity with atrial fibrillation risk. Models were adjusted for biological and behavioural risk factors and the remaining physical activity types. Physical activity was categorised in tertiles and the low group was used as reference.
Results
During 16.8 years of follow-up (median: 12.3 years, interquartile range: 8.7–15.9 years), 800 atrial fibrillation events occurred (11.4% of the study population). We observed no association between total physical activity and atrial fibrillation risk in any model. After adjustment for confounders, the hazard ratio and 95% confidence interval for the high physical activity category compared to the low physical activity category was: 0.71 (0.80–1.14) for total physical activity. We did not observe a significant association between any of the physical activity types with atrial fibrillation risk.
Conclusion
Our results suggest that physical activity is not associated with higher or lower risk of atrial fibrillation in older adults. Neither total physical activity nor any of the included physical activity types was associated with atrial fibrillation risk.
Introduction
Physical activity (PA) has been extensively proven to reduce the risk of cardiovascular disease (CVD) and all-cause mortality.1,2 However, it remains unclear whether all cardiovascular conditions, including atrial fibrillation (AF), the most common chronic cardiac arrhythmia with significant morbidity and mortality, 3 may benefit from PA. Prevalent and incident AF is associated with higher risk of myocardial infarction, heart failure and all-cause mortality.4,5 Therefore, to reduce the overall burden associated with CVDs in the general population, knowing more about potential factors associated with AF risk is important.
However, the relation between PA an AF remains controversial.6–8 Meta-analyses of mostly prospective cohort studies with ages of participants ranging from 40 up to 75 years found no significant association between leisure time PA and AF risk in pooled analyses.6,7 However, it has been hypothesised that the relation between PA and AF is U-shaped, with lower risk when exercising at moderate intensity or duration, but not when exercising vigorously.9–11 A recent review indicated that especially strenuous exercise is related to the development of AF in well-trained individuals. 12 As intensity is related to the type of PA, this implies that the association between PA and AF risk might be related to the type of PA in which adults engage in. Two studies have found that walking and cycling were inversely related to AF risk.9,13 In addition to these activities, older people engage in a number of other PA types, including gardening, domestic work or sports in general. These different PA types vary in intensity, frequency and duration, and might be differently associated with AF risk. For older people unable to engage in certain leisure-time activities, the health effects of other PA types might be informative and crucial in lowering their AF risk. Since overall PA levels tend to decrease with age, this is especially important. 14
Therefore, we aimed to examine the association between total PA and AF incidence in a population of older adults, aged 55 years and over. Furthermore, we assessed the independent association of different types of PA, including walking, gardening, domestic work, sports and cycling, with AF incidence.
Methods
Study population
This study was embedded within the Rotterdam Study (RS), a prospective population-based cohort study among subjects aged 55 years or older in the municipality of Rotterdam, The Netherlands. Between 1990–1993, the baseline examination of the original cohort was performed (RS-I). The RS was extended in 2000–2001 with 3011 participants who had either become 55 years old or had moved into the study district (RS-II). For this study, we used data from the participants attending the third examination of the original cohort (RS-I-3, between 1997–1999; n = 4797) and the participants attending the first examination of the extended cohort (RS-II-1, between 2000–2001; n = 3011). 15 Altogether, 7310 participants completed PA data collection. Subjects with prevalent AF were excluded (n = 205) (see Supplementary Material Figure 1). Following this, 54 subjects were excluded due to not providing, or having withdrawn, informed consent for collection of follow-up data. Thirty-three cases were removed because of unreliable PA values or missing follow-up data. A total of 7018 subjects were included in the analyses. Baseline information was collected by trained research assistants who interviewed the participants at home. All subjects gave written consent, and the study protocol was approved by the medical ethics committee according to the Wet Bevolkingsonderzoek ERGO (Population Study Act Rotterdam Study), executed by the Ministry of Health, Welfare and Sport of The Netherlands. Detailed information on the design of the Rotterdam Study can be found elsewhere. 15 Covariates were assessed when participants visited the study centre or were collected through home interviews. Information regarding the measurement of covariates is provided as online Supplementary Material.
Physical activity assessment
PA levels were assessed with an adapted version of the Zutphen Physical Activity Questionnaire. 16 The original questionnaire has been validated with a test-retest reliability of 0.93 and a correlation with doubly labelled water of 0.61. 17 The questionnaire contains questions regarding the average weekly duration in walking, cycling, sports, gardening and hobbies over the past year. Questions on domestic work were added to obtain a more reliable estimate of the PA level in this age group. Detailed information on the collection of PA can be found elsewhere. 18
We used the metabolic equivalent of task (MET) to quantify the intensity of an activity according to the 2011 updated version of the Compendium of Physical Activities. 19 Sports that were mentioned in the questionnaire that were not in this compendium were not used in the analyses (n = 33). Finally, we calculated METċhoursċweek-1 in total PA (i.e. the sum of cycling, walking, sports, domestic work and gardening) and in every type of PA (cycling, walking, sports, domestic work, gardening).
Clinical outcome
The main outcome measure under study was AF. Data on clinical outcomes were collected through an automated follow-up system involving digital linkage of the study database to medical records maintained by general practitioners working in the research area. Trained research assistants collected notes, outpatient clinic reports, hospital discharge letters and electrocardiograms (ECGs). AF was coded as an event when it had been diagnosed with a 12-lead ECG. Research physicians independently adjudicated all data on potential events. Medical specialists reviewed potential cases as a final decision. Follow-up was complete until 1 January 2014.
Statistical analysis
Due to their non-normal distribution, all five PA types and total PA were categorised into tertiles. Total PA, walking and domestic work were divided into three categories of equal size by the 33rd and 66th percentiles of MET·h·week−1. Since a large proportion of the participants did not participate in sports, gardening and cycling, the bottom category for these types was no participation and the remaining two categories were created by using the median. 18 We assessed the association of total PA and all types of PA with incident AF with Cox proportional hazards, after confirming that the assumption for proportional hazards was met. The underlying timescale in these models was follow-up time, defined as the time between PA assessment and the first fatal or nonfatal AF event, death, or censoring at 1 January 2014. Additionally, we applied natural cubic splines to test for non-linearity of the survival models, 20 but we found no evidence for a non-linear association between PA and AF risk.
To minimise confounding, covariates were added separately in different models. Model 1 was adjusted for age and sex. Model 2 was the model additionally adjusted for behavioural risk factors, including smoking, prevalent CVD, alcohol consumption, diet quality and education. For the PA types, model 2 was also adjusted for the MET·h·week−1 in all other PA types. The decision to include confounders in the multivariable regression models was based on previous literature or >10% change of the effect estimate in the crude model.6,7 PA variables were entered as categorical variables (tertiles) in the separate models.
In sensitivity analyses, to examine the effect of biological risk factors, we repeated our analyses in a model additionally adjusted for body mass index (BMI), total and high-density lipoprotein (HDL)-cholesterol, diabetes, lipid-reducing agents, systolic and diastolic blood pressure, anti-thrombotic agents and angiotensin-converting enzyme (ACE)-inhibitor use. We also performed stratified analyses by sex and age (below 65 years and 65 years and above). Furthermore, to see whether our results would be driven by CVD, we performed an additional analysis by excluding participants with prevalent CVD (n in analysis = 5997), and we performed an analysis excluding participants who developed coronary heart disease in the follow-up period (n in analysis = 5887). Since we did not obtain occupational PA data, we analysed our data in non-workers (n in analysis = 6197). Finally, because of high risk of mortality in this population, we evaluated the association in a competing risk analysis, using the method proposed by Fine and Gray. 21
Our data contained missing values for diet (28.7%), systolic and diastolic blood pressure (10.2%), BMI (10.6%), total cholesterol (13.2%) and HDL-cholesterol (14.2%). Other covariates had <10% missing data. Missing variables were calculated by IBM statistics with the multiple imputation (n = 5 imputations) function based on the distribution of existing data. All analyses were conducted using SPSS software version 24 (IBM SPSS Statistics for Windows, Armonk, New York, USA) and R (3.0.1).
Results
Baseline participant characteristics by tertile of total physical activity (PA), Rotterdam Study, 1997–2012.
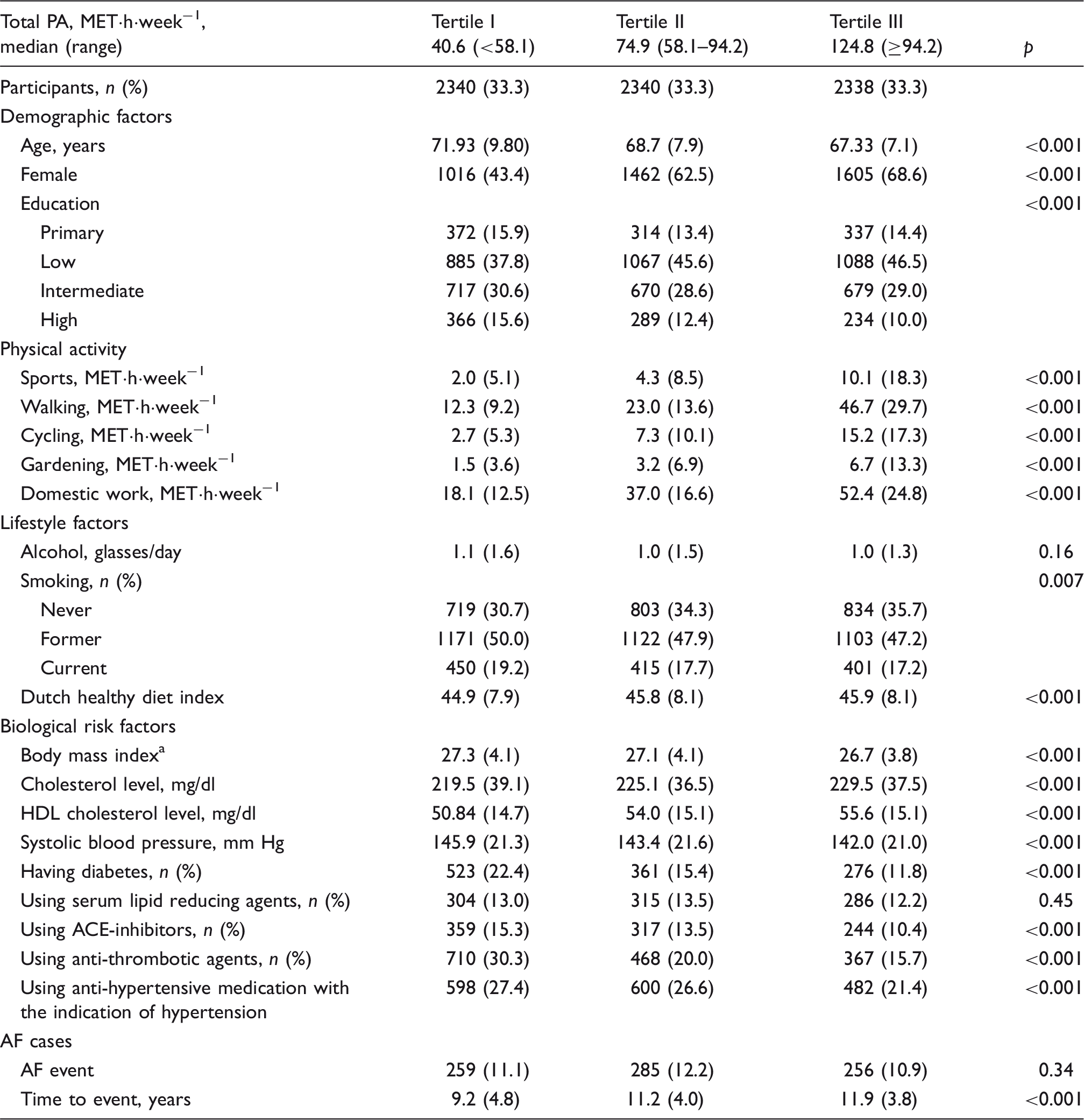
ACE: angiotensin converting enzyme; AF: atrial fibrillation; HDL: high density lipoprotein; MET: metabolic equivalent of task; SD: standard deviation.
Data are presented as mean (SD), unless otherwise stated.
Weight (kg)/height (m) 2
Association between total physical activity (PA) and different types of PA and atrial fibrillation (AF), Rotterdam Study, 1997–2012.
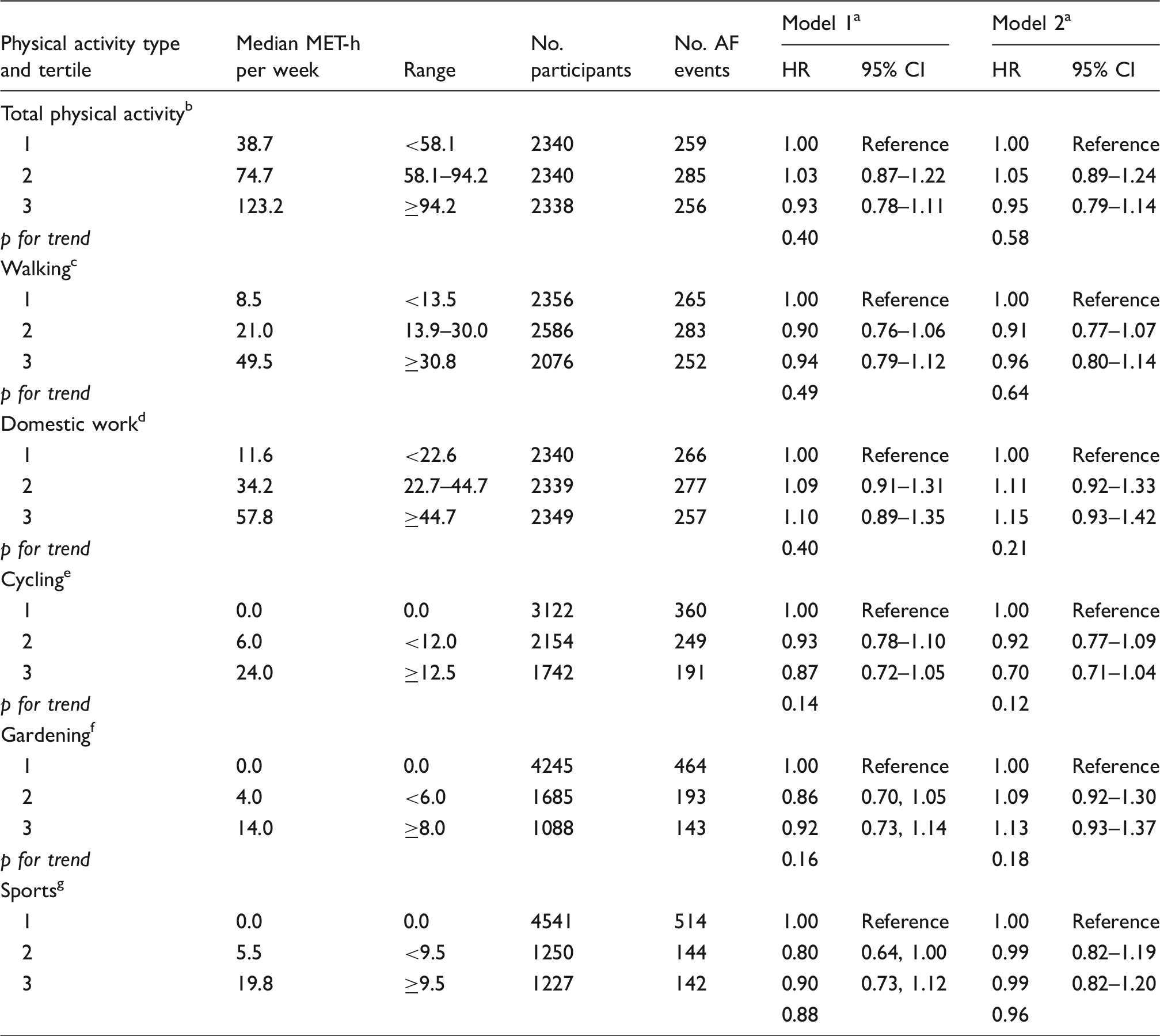
CI: confidence interval; HR: hazard ratio; MET: metabolic equivalent of task.
Model 1 was adjusted for age and sex. Model 2 was additionally adjusted for all other PA types, smoking, previous cardiovascular disease, alcohol consumption, diet, education.
Total PA is composed of all PA types and thus of different METs. In this regard, the median levels of total PA across categories are equivalent to 1.5, 2.8 and 4.5 h per day of moderate PA equivalent of 4 METs.
Walking is equivalent to 3.0 METs. The median levels of walking across categories are therefore equivalent to 26, 60 and 141 min per day of walking.
Average domestic work is equivalent to 3.5 METs. 15 The median levels of domestic work across categories are therefore equivalent to 32, 88 and 146 min per day of domestic work.
Cycling is equivalent to 4.0 METs. The median levels of cycling across categories are therefore equivalent to 0, 13 and 51 min per day of cycling.
Gardening is equivalent to 4.0 METs. The median levels of gardening across categories are therefore equivalent to 0, 9 and 30 min per day of gardening.
Average sports is equivalent to 5.5 METs. The median levels of sports across categories are therefore equivalent to 0, 9 and 31 min per day of sports.
For all five PA types, we did not observe a significant association with AF risk in the crude model, or in model 2, adjusted for behavioural risk factors (Table 2). Furthermore, we did not observe a significant trend across categories in any of the analyses. For example, the HRs (95% CI) for the high category of walking and cycling were 1.00 (0.84–1.20) and 0.92 (0.76–1.12), respectively, compared to the low categories, with p values for trend 0.98 and 0.43, respectively.
In sensitivity analyses adjusted for biological risk factors, our associations were similar to the main results (Supplementary Material Table 1). Our sensitivity analyses split by age and sex showed some differences in HRs between the groups, but the results remained non-significant (Supplementary Material Tables 2 and 3). Moreover, excluding employed participants, excluding participants who previously were diagnosed with CVD or excluding participants with incident CHD did not change the results meaningfully (Supplementary Material Tables 4–6). In the analyses using the competing risk approach, we noticed that higher levels of PA were associated with a higher risk of developing AF. This was the result of the lower risk of mortality in the higher PA groups (Supplementary Material Table 7 and Supplementary Material Figure 2).
Discussion
In this population-based study of adults aged 55 years and over, we found no evidence for an association between PA and AF risk over 16.8 years of follow-up. Total PA was not associated with an increased or decreased AF risk and we did not observe an association for any of the PA types with AF.
Our findings are in concordance with several meta-analyses, which do not support an association between moderate or vigorous leisure-time PA and AF risk.6–8 On the other hand, our results contradict a number of recent cohort studies, reporting that moderate intensity PA or leisure-time PA is associated with a lower risk of AF.9,13,22 One study found a J-shaped association, with lower AF risk for moderate PA levels (i.e. ≥4 h of weekly exercise), and increasing AF risk when exercising at vigorous intensity or longer duration. 22 Other studies observed a U-shaped association, with the lowest risk for participants exercising at moderate intensity.9,10,13,23 Among elderly participants, higher levels of walking,9,13 cycling 13 and general leisure time PA9,24 have been shown to be associated with lower AF risk. The fact that we did not observe a beneficial association between PA and AF risk in the current population might be related to the relatively high burden of cardiovascular risk factors observed in our participants, including a high BMI and a high proportion of participants with diabetes. Moreover, the widely varying categorising of PA might affect the comparability between studies. For example, in one study both walking distance and walking pace were assessed, 24 whereas only information on walking duration was obtained in the current study. Subsequently, the different results between studies might be explained by this methodological difference. For example, in our study two persons can both report one hour of walking per week, but one person might walk four kilometres within this time frame, whereas another walked six kilometres. In this case, the discriminative power of our walking estimate might be too low to find an association with AF risk. Future studies on the association between walking and AF should therefore collect information on walking duration, walking pace and walking distance, to get a more complete overview of the PA pattern.
Furthermore, the fact that we did not find an association between any PA variable and AF might also be explained by the relatively high PA levels of our population. Participants in the low group of total PA engaged in a median level of 38.7 MET·h·week−1 of PA, corresponding to 1.4 h/day of moderate intensity PA of four METs. Considering the fact that the greatest health effects are usually gained at low levels of PA,13, 25 it is possible that the participants in the low group of PA in the current study were already sufficiently active and where therefore not at higher risk of developing AF. This hypothesis is supported by the relatively low percentage of AF cases in the current study (11.4%), compared to the 19% of AF incidence in a similar study population. 9 Moreover, active individuals might be more health conscious and therefore more often evaluated for cardiac arrhythmias. 7 In comparison to individuals who engage in less PA, this subgroup might thus have higher rates of AF diagnoses. Subsequently, this could bias the association between PA and AF.
There have been several proposed mechanisms for the association between PA and either higher or lower AF risk. The proposed mechanism behind the association between PA and lower AF risk is that PA can have a beneficial effect on several AF risk factors, including improving the management of hypertension and diabetes mellitus,26,27 assisting in weight management 28 and improving cardiac structure and function.29,30 Conversely, PA might increase AF risk when individuals engage in frequent exercise (i.e. 5–7 times per week) and with high intensity. 31 This might be especially the case for vigorous exercise in younger adulthood. 11 Pathophysiological pathways for the increased AF risk following vigorous exercise are left atrial enlargement, left ventricular hypertrophy, left ventricular dilation, inflammatory changes and an increase in parasympathetic tone.13,32,33 Moreover, atrial fibrosis has also been suggested to contribute to exercise-induced AF. 12 It could be hypothesised that some participants in the current study were very active in young adulthood and this might have contributed to a higher AF risk in later life.31,34 In this case, our associations might be affected by residual confounding by previous PA levels.
An interesting finding in the current study was observed in our sensitivity analyses including the competing risk of mortality. In these analyses we observed a higher risk of AF for participants included in the medium group of total PA. This finding can be explained by the lower risk of mortality in these participants. As result of the lower mortality risk, these participants were at risk to develop AF for a longer period of time, and therefore their lifetime risk of AF was greater. However, this does not indicate that older adults should be discouraged to engage in high levels of PA, as the AF risk in the lowest PA group was only lower because these participants died earlier.
Our study contains several strengths, including the large sample size of elderly adults, a long follow-up period of almost 17 years, and the prospective population-based design. Furthermore, by confirming the AF diagnoses through ECG, and by independent judging all cases by two medical doctors and an expert in the field, we obtained an accurate measure of AF cases in our population. By adding different types of PA, we were able to independently study their association with AF. Moreover, in studying this association, we adjusted for several factors which minimised the chance of finding a confounded result.
However, we also need to acknowledge some limitations. We measured PA with a self-reported questionnaire. Our questionnaire has been shown to be valid and reliable, 17 but recall bias and social desirable answers cannot be excluded. However, the use of questionnaire data on PA is essential when examining types of PA. Further, in the current study we used the Compendium of Physical Activities to assign MET-values to activities in the questionnaire. 19 While assigning these values, we carefully considered the age of our study population. However, this might not have captured the energy expenditure of older adults accurately. Furthermore, since only duration of performed PA was obtained, this might also have given rise to heterogeneity with regard to the intensity in which participants engaged in the different PA types. This might have led to misclassification of participants with either higher or lower intensity levels than our assigned values. Since this misclassification was non-differential, this could have biased our estimates towards the null hypothesis. Also, PA was assessed only once in our study, which could have resulted in missing PA changes in participants, which could have altered their AF risk during follow-up as compared to their baseline activity profile. Further, AF has a tendency to be asymptomatic. We cannot rule out that some of our non-cases were in fact ‘silent’ AF cases leading to an underestimation of total AF cases.
In conclusion, our results suggest no association between PA and AF risk in older adults. Neither total PA nor any of the included PA types was associated with an increased or decreased AF risk in any of the analyses.
Footnotes
Acknowledgements
The dedication, commitment and contribution of inhabitants, general practitioners and pharmacists of the Ommoord district to the Rotterdam Study are gratefully acknowledged.
Author contribution
The contributions of the authors were as follows: MA, CMK and OHF had the original idea for the study. MA and CMK jointly participated in its design, performed the statistical analysis, interpreted the data, drafted and critically revised the article. MAI, JAJDS, MK, FJAvR and OHF revised the manuscript critically for important intellectual content. OHF provided supervision. All authors read and approved the final article. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Rotterdam Study is funded by Erasmus MC and Erasmus University, Rotterdam, the Netherlands; the Netherlands Organisation for Scientific Research (NWO); the Netherlands Organisation for the Health Research and Development (ZonMw); the Research Institute for Diseases in the Elderly (RIDE); the Ministry of Education, Culture and Science; the Ministry for Health, Welfare and Sports; the European Commission (DG XII); and the Municipality of Rotterdam. MK is supported by NWO VENI grant (VENI, 91616079). OHF works in ErasmusAGE, a centre for aging research across the life course funded by Nestlé Nutrition (Nestec Ltd) and Metagenics Inc. Nestlé Nutrition (Nestec Ltd) and Metagenics Inc. had no role in design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.