
Abstract
Background
Patients who survive after an aneurysmal subarachnoid haemorrhage (ASAH) have an increased incidence of cardiovascular events compared with the general population. We assessed whether troponin elevation after aneurysm occlusion, as marker of myocardial injury, can predict long-term cardiac events.
Methods
We analysed a prospectively collected cohort of 159 patients with ASAH and early aneurysm occlusion, in whom routine post-intervention troponin I (TnI) measurements were performed. With competing risk regression modelling we estimated the association between TnI elevation after aneurysm occlusion and major adverse cardiac events within one year. Secondary outcome measures were all-cause mortality and neurological condition within one year. The predictive value of post-intervention TnI was compared with the predictive value of pre-intervention characteristics using c-statistics and the integrated discrimination improvement index.
Results
Subdistribution hazard ratios for TnI elevation and major adverse cardiac events at one year were 1.05 (95% confidence interval (CI) 1.03–1.07) per 10 ng/l increase in TnI and 7.91 (95% CI 1.46–43.0) for any TnI elevation. After adjustment for pre-intervention variables, the subdistribution hazard ratios were 1.47 (95% CI 0.81–2.67) per 10 ng/l and 9.00 (95% CI 1.62–50.1) for any elevation. The c-statistic was 0.71 for TnI elevation as a continuous measure and 0.69 for any TnI elevation. The integrated discrimination improvement index showed a minimum improvement in prediction of 0.08 (interquartile range 0.06 to 0.09) for TnI as a continuous measure and 0.003 (interquartile range −0.004 to 0.01) for any TnI elevation, when compared with pre-intervention characteristics.
Conclusion
TnI elevation after occlusion of a ruptured intracranial aneurysm predicts the occurrence of a major adverse cardiac event within one year after ASAH.
Introduction
Patients who have survived an episode of aneurysmal subarachnoid haemorrhage (ASAH) and in whom the aneurysm has been occluded, have an overall increased long-term mortality rate and an increased incidence of cardiovascular events compared with age- and sex-matched groups.1,2
In the hours to days after an ASAH, excessive sympathetic activation can cause neurogenic stress cardiomyopathy, 3 which is displayed by an increased cardiac troponin as a biomarker of cardiac injury. 4 In up to half of all ASAH patients, elevated troponins are reported 4 and several studies have shown the prognostic relevance of elevated troponin early after admission for poor neurological outcome and mortality.4–6 ASAH patients have lower peak troponin levels as compared with patients with acute coronary syndromes, 5 suggesting that most have so-called contraction band necrosis, instead of myocardial ischaemia.4,5 Interestingly, a second increase in troponin levels was observed on day 3 after the ictus, 5 which may reflect myocardial injury during interventions to occlude the aneurysm. Studies among patients undergoing non-cardiac surgery have suggested that perioperative myocardial injury is a predictor of future major adverse cardiac events (MACEs).7,8 Therefore, our aim was to assess the pattern of pre- and post-intervention troponin levels, to study the association between post-intervention troponin elevation and MACEs and to investigate whether troponin elevation after early occlusion of the ruptured aneurysm would be a good predictor of MACE within the first year after an ASAH.
Methods
Patients
For the current study we included patients who had received general anaesthesia for early neurosurgical clipping or endovascular coiling of a ruptured intracranial aneurysm and in whom routine troponin I (TnI) measurements were performed. The preferred treatment modality was chosen on a multidisciplinary level and irrespective of the research question of this study. Patients were retrospectively collected from two different prospective cohorts (see Supplementary Material Figure 1). The first cohort consisted of patients who underwent early aneurysm occlusion with either clipping or coiling at our hospital between November 2005 and February 2008. TnI was measured daily until eight days after presentation. 9 The second group of our patients was retrieved from a database including patients aged 60 years or older who had undergone non-cardiac surgery at our hospital and in whom TnI was measured routinely on post-intervention days 1, 2 and 3. 8 From this database we selected all patients who had undergone early clipping between March 2011 and November 2014; patients who had undergone coiling were not part of this database. After selecting eligible patients from both cohorts, we excluded patients who had undergone a re-operation within three days, to make sure the peak TnI value within three days could be assigned to the first procedure. In both cohorts, further follow-up of elevated TnI levels was left to the discretion of the treating physician.
The local medical ethics committee (Medical Research Ethics Committee, University Medical Centre Utrecht, 16-441/C) waived the need for informed consent. This study was conducted in adherence to the STROBE statement for observational research. 10
Troponin values
Different TnI assays were used over the years (see Supplementary Material Figure 1). In our analyses, we used the clinical cutoff values as used at our institution within the respective time periods, instead of the 99th percentile upper reference limit, 11 since clinical decisions were based upon these cutoff values. TnI values were collected from the day of admission until post-intervention day 3 and the highest TnI value within three days after the intervention was selected. Two different definitions of troponin elevation were used: an absolute increase above the cutoff value (continuous measure) and presence of any post-intervention TnI elevation above the cutoff value (dichotomized measure).
Outcomes
The primary outcome was MACE at one year, defined as myocardial infarction, need for revascularization or cardiac death. All-cause mortality within one year was a secondary outcome measure, as was neurological outcome at three months, defined by the Glasgow Outcome Scale. 12 Last, we included residence at one year to reflect neurologic outcome, defined as: 1) residing at home, 2) residing in a nursing home or rehabilitation centre or 3) deceased.
Other risk factors
Comparison between patients with and without post-intervention troponin measurement.
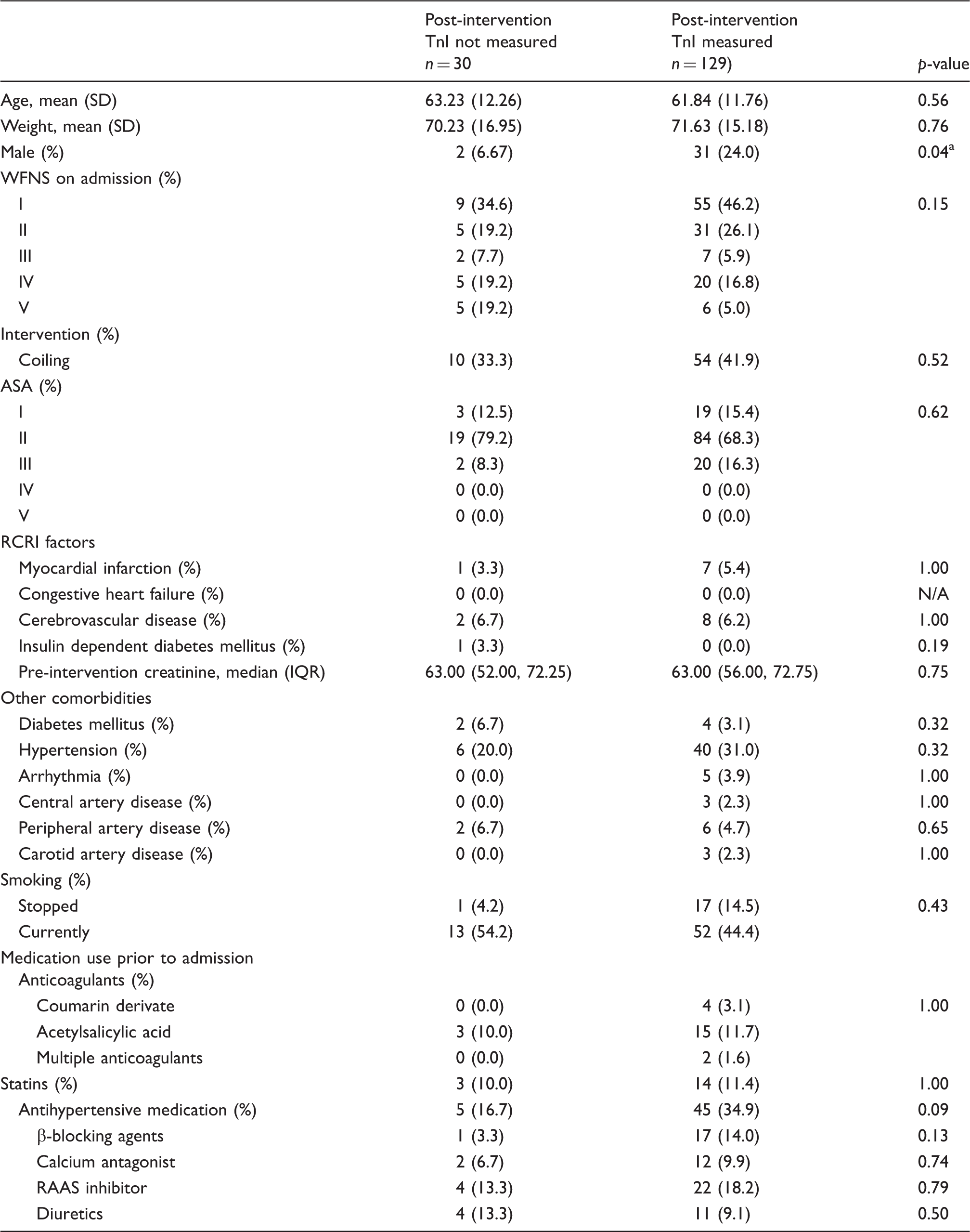
Statistically significant at a level of significance of p < 0.05.
TnI: troponin I; SD: standard deviation; WFNS: World Federation of Neurological Surgeons Grading System for aneurysmal subarachnoid haemorrhage; ASA: American Society of Anesthesiologists Physical Status Classification; RCRI: Revised Cardiac Risk Index; N/A: not applicable; IQR: interquartile range; RAAS: renin–angiotensin–aldosterone system
Data were extracted from two databases: the ASAH registration database, which contains data from admission until three months after the ictus, and a separate database containing long-term follow-up data, collected by means of annually distributed standardized surveys. Additional data on pre-intervention risk factors were derived from the hospital-wide data warehouse.
Missing values
As complete case analyses are known to lead to biased effect estimates, missing values were handled using multiple imputation after confirming that data were indeed missing at random. 17 For this, we compared baseline characteristics and outcomes for patients in whom a post-intervention TnI was measured with those in whom it was not. We used the mice package in R, creating 35 imputation sets.18,19 Analyses were conducted in each of these datasets; subsequently estimates were pooled using Rubin’s rule.20–22
Statistical analysis
Routine TnI measurements prior to the intervention were obtained only between November 2005 and February 2008. Therefore, these values were only used to inspect the pattern of TnI elevation by using boxplots, including all values from the day of admission until three days after the intervention.
Descriptive statistics for baseline characteristics were obtained by stacking the imputation sets. Patients with and without any post-intervention TnI elevation were compared with respect to the baseline characteristics using a χ 2 test, Fisher’s exact test, independent t test or Mann–Whitney U test as appropriate.
To determine the association between post-intervention TnI values and MACE at one year and to adjust this association for the competing risk of all-cause death, a univariable competing risks regression analysis was done using the method of Fine and Gray. 23 From this analysis we extracted the subdistribution hazard ratio, where patients remain in the risk set after experiencing a competing event, which is most suitable for prediction research. 23 For all-cause mortality after one year a Cox proportional hazards analysis was conducted.
Subsequently, the regression analyses were repeated with adjustment for risk factors that had a known association with TnI elevation after ASAH in the literature, namely age and WFNS score on admission.4,6 The proportional hazard assumption was tested by inspecting the Kaplan–Meier curve and by plotting the scaled Schoenfeld Residuals of the included variables versus time and testing the slopes. 23
Cumulative incidences were calculated, taking competing risks into account. Finally, we compared the predictive value of the above defined pre-intervention risk factors with TnI alone. The predictive value was expressed using the c-statistic, again adjusted for competing risks. 24
Additionally, the integrated discrimination improvement index (IDI) was used to further determine the predictive accuracy of TnI by comparing the predictive value of TnI alone with that of several pre-intervention patient characteristics separately.25,26 The IDI was expressed as the median and the interquartile range (IQR) of all indices obtained from the 35 imputed datasets.
Separate analyses were done for TnI elevation as a continuous and as a dichotomous measure.
Throughout the analyses, a p-value < 0.05 was considered to be significant and 95% confidence intervals (CIs) or IQRs were reported where applicable. The statistical analyses were performed with R (Version 3.3.1 – © 2016-06-21, for Macintosh, R, Inc., Vienna, Austria). 22
Results
The study included 159 patients. In 30 patients (18.9%), no post-intervention TnI values were available, while in 41 patients (25.8%) no data were present on MACEs within one year (see Supplementary Material Table 2 for an overview of missing data). To determine whether values were missing at random, patients in whom troponin was measured, were compared with those in whom it was not. MACEs occurred in five out of 118 patients (4.2%) with an available post-intervention TnI value and in one out of 41 patients (2.4%) without a post-intervention TnI value (p = 1.00). There were small differences in baseline characteristics in patients with and without available post-intervention TnI values (Table 1), indicating that missingness was not completely at random, thus supporting the need for multiple imputation.
During admission, 11 patients (6.9%) died after aneurysm occlusion and five (3.1%) experienced a MACE. Within the first year, 26 patients (16.4%) had died and seven patients (4.4%) had a MACE.
Baseline characteristics.
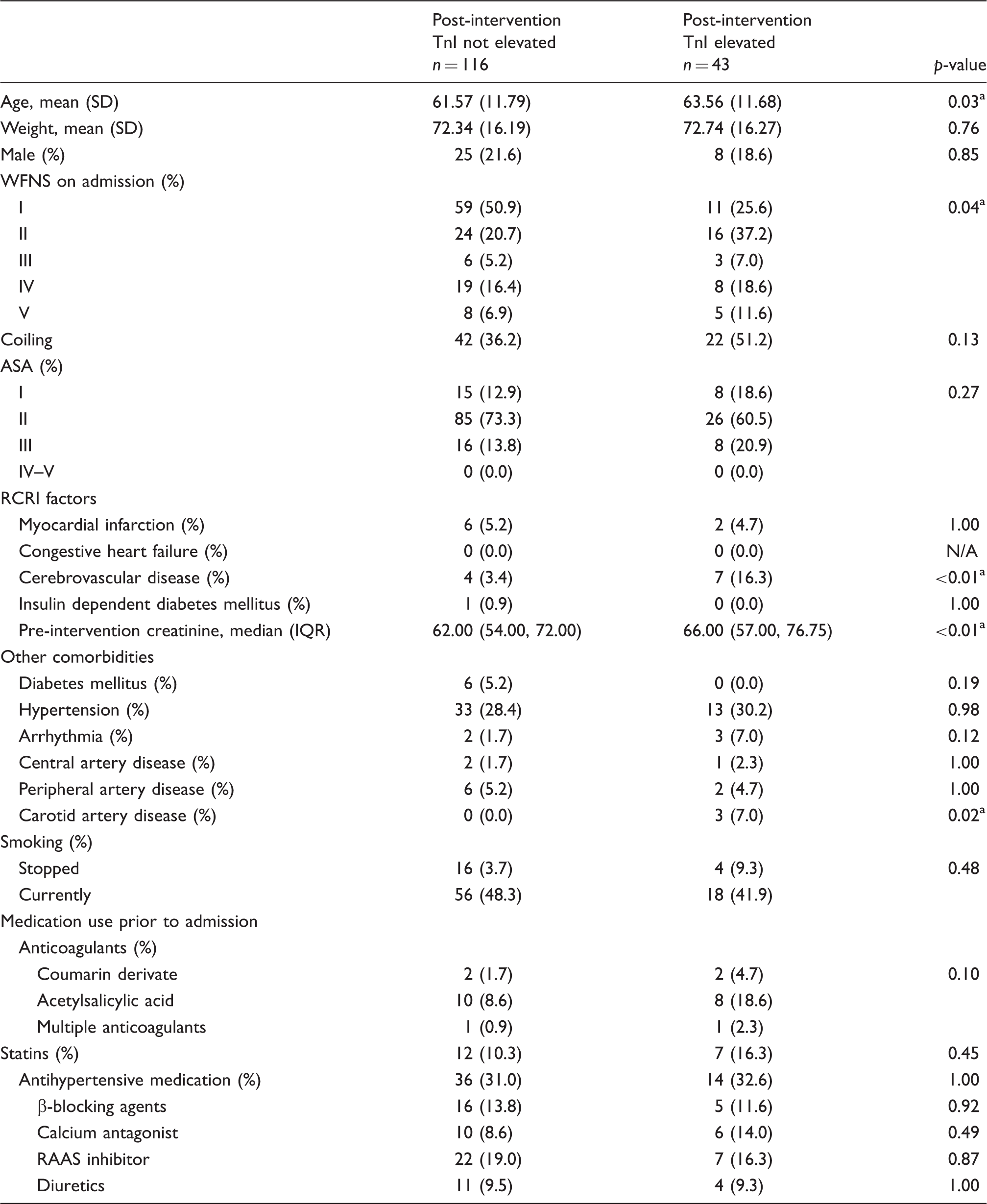
Statistically significant at a level of significance of p < 0.05.
TnI: troponin I; SD: standard deviation; WFNS: World Federation of Neurological Surgeons Grading System for aneurysmal subarachnoid haemorrhage; ASA: American Society of Anesthesiologists Physical Status Classification; RCRI: Revised Cardiac Risk Index; N/A: not applicable; IQR: interquartile range; RAAS: renin–angiotensin–aldosterone system
At group level there seemed to be a renewed increase in median TnI starting at day 4 after admission, while, on average, the aneurysm was occluded at 2.5 days after admission (Figure 1). From 33 patients we had both pre-intervention and post-intervention TnI values. Twelve patients showed an increase in TnI after the intervention, but in only six patients did this value pass the cutoff value for an elevated TnI. Only one of these patients was diagnosed with a myocardial infarction.
Boxplots showing the distribution of troponin I (TnI) levels per day after admission.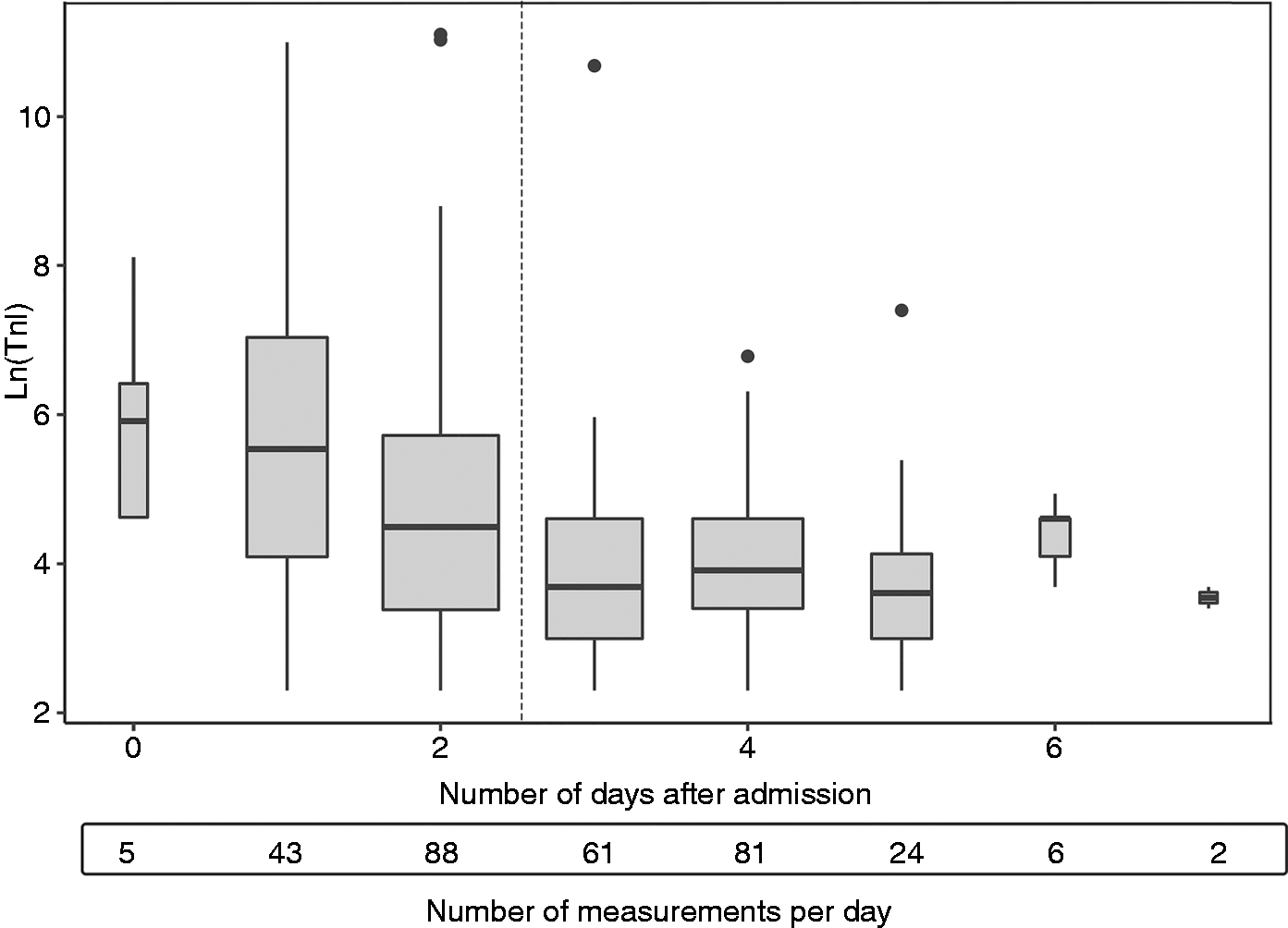
TnI elevation and clinical outcomes.
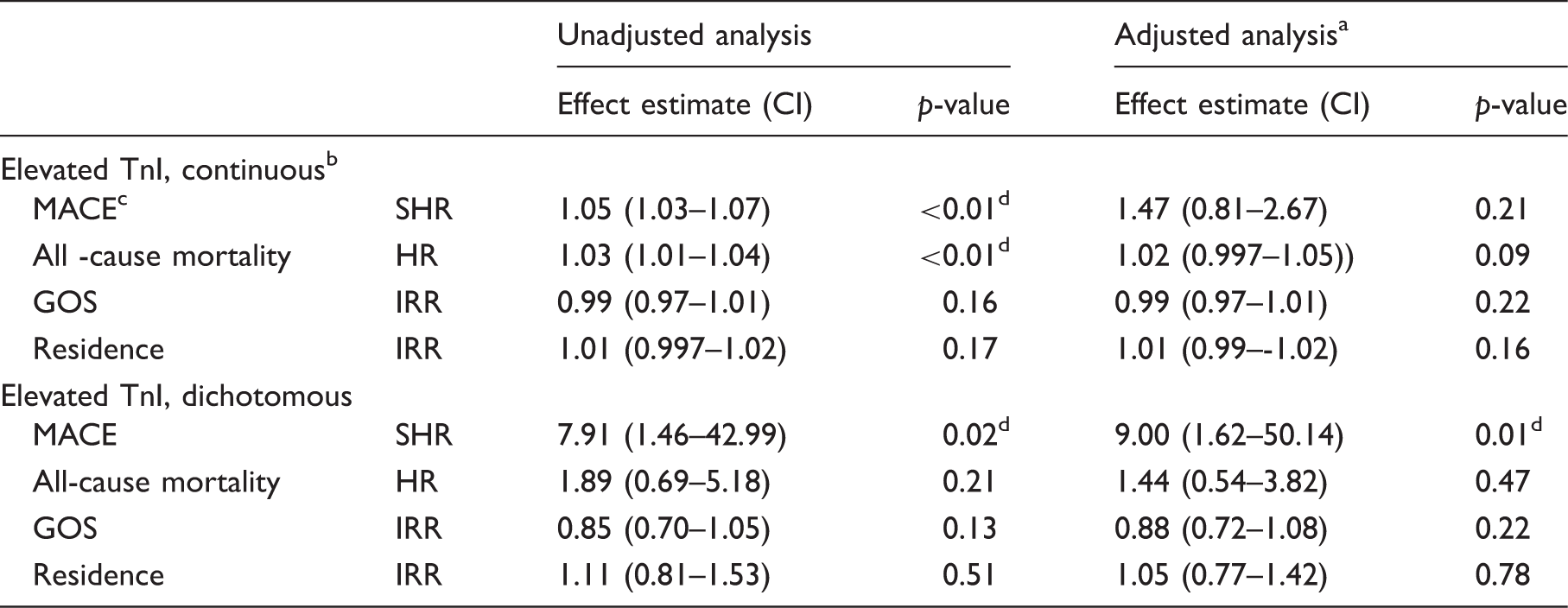
Adjusted for age and World Federation of Neurological Surgeons Grading System for aneurysmal subarachnoid haemorrhage.
Expressed per 10 ng/l change in troponin from the cutoff.
MACE, all-cause mortality and residence at one year; GOS at three months.
Statistically significant at a level of significance of p < 0.05.
CI: confidence interval; TnI: troponin I; MACE: major adverse cardiac event; SHR: subdistribution hazard ratio; HR: hazard ratio; GOS: Glasgow Outcome Scale; IRR: incidence rate ratio
Predictive value of post-intervention TnI.
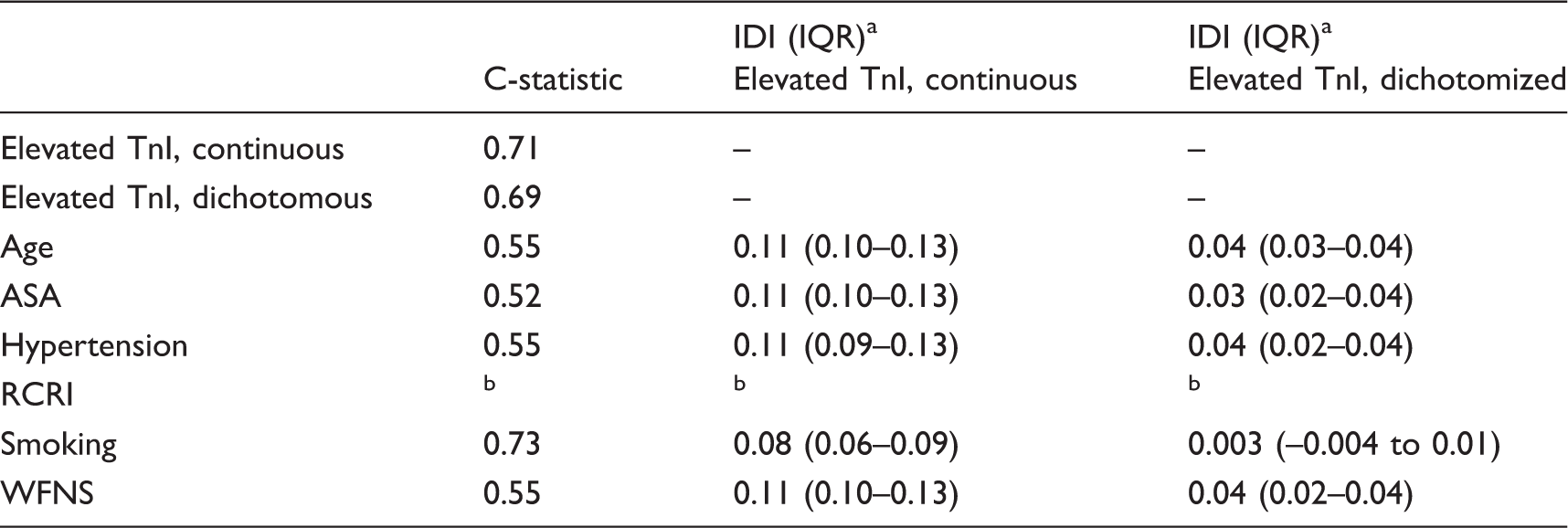
Predictive value of TnI compared with the predictive value of pre-intervention patient characteristics separately.
Variable could not be included because the model did not converge.
TnI: troponin I; IDI: integrated discrimination improvement index; IQR: interquartile range; ASA: American Society of Anesthesiologists Physical Status Classification; RCRI: Revised Cardiac Risk Index; WFNS: World Federation of Neurological Surgeons Grading System for aneurysmal subarachnoid haemorrhage
Discussion
This study showed that troponin elevation after early occlusion of a ruptured intracranial aneurysm was an independent predictor for MACE within one year after the ASAH. After adjustment for age and WFNS score on admission, the association with MACE at one year was no longer statistically significant for troponin elevation on a continuous scale, but remained significant for troponin elevation as a dichotomized measure. There was no association between troponin elevation after aneurysm occlusion and neurological outcome, nor with mortality in the multivariable analysis. The pattern in troponin levels during the initial days after admission suggested a second elevation corresponding to the average day of aneurysm treatment, as was found previously. 5 This renewed increase in troponin might very well reflect perioperative myocardial injury.
Clinical implications
To our knowledge, neither the predictive value of post-intervention troponin elevation nor the association of post-intervention troponin values with MACE in the long term has been investigated before in ASAH patients. The 2016 European Guidelines on cardiovascular disease prevention states that patients with a history of a cardiovascular disease, including any kind of stroke, have a high cardiovascular risk profile. Implementation of prevention strategies such as lifestyle changes and management of risk factors before hospital discharge is recommended.27 We believe that post-intervention troponin elevation may be helpful in identifying the patients with the highest cardiovascular risk. The predictive value of post-intervention troponin levels has been more extensively studied in the general non-cardiac surgery population,7,8 where the vast majority of patients with elevated troponin levels was asymptomatic, despite frequent perioperative exposure to physiological and emotional stress. 8 This implicates that postoperative TnI elevation reflects myocardial injury rather than myocardial ischaemia, as well as that routine postoperative TnI surveillance can be utilized for postoperative risk stratification to direct secondary prevention. It has been shown in the non-cardiac surgery population that this can not only improve outcomes, but it is also cost-effective. 28 For ASAH patients, the (cost-)effectiveness of secondary prevention for cardiac events remains unclear and needs further investigation. 27
Limitations
The strength of this study is the use of routinely obtained troponin values and data from clinical care, thus representing daily practice instead of a controlled research setting. Nevertheless, this study has some obvious limitations. First, although we found that a post-intervention increase in TnI is an independent predictor of MACE, the sample size was too small to create an extensive prediction model. Second, due to a limited amount of routine pre-intervention TnI measurements, pre-intervention values were used for the boxplot, but were excluded from further analyses. To explore the underlying aetiology of perioperative myocardial injury and MACE, these values should be incorporated into future studies. Third, although we did not find a relevant difference in baseline characteristics (see Supplementary Material Table 3), our study cohort was created using two different cohorts. We used the cutoff values set by our laboratory, since clinical decision making and diagnosis was based upon these values. Therefore, we believe that the use of different TnI assays did not influence our results. Fourth, this study does not differentiate between intervention types, since surgical and endovascular therapies are known to be associated with similar risks of cardiac injury in patients with an ASAH. 29 Finally, we used a survey to collect data after discharge, which can cause (non-)response bias. Although the response rate of the survey was reasonable (65%; see Supplementary Material Table 4), myocardial infarction might be underreported in our study, possibly underestimating the effect estimates.
Conclusions
Patients with TnI elevation after occlusion of a ruptured intracranial aneurysm have a higher risk of MACE within one year than patients without TnI elevation. Although post-intervention troponin elevation was a predictor of these events, further research is required to explore the utility of troponin monitoring in directing secondary prevention in ASAH patients.
Take home message
Troponin elevation after occlusion of a ruptured intracranial aneurysm predicts the occurrence of future MACEs.
Supplemental Material
Supplemental material for Cardiac events within one year after a subarachnoid haemorrhage: The predictive value of troponin elevation after aneurysm occlusion
Supplemental material for Cardiac events within one year after a subarachnoid haemorrhage: The predictive value of troponin elevation after aneurysm occlusion by Annemarie Akkermans, Linda M Peelen, Judith A van Waes, Gabriël J Rinkel and Wilton A van Klei in European Journal of Preventive Cardiology
Footnotes
Author contribution
All authors contributed to the conception and design, to the interpretation and gave final approval. AA contributed to the acquisition and drafted the manuscript. AA and LP contributed to the analysis. LP, JW, GR, WK critically revised the manuscript. All authors agree to be accountable for all aspects of work ensuring integrity and accuracy
Acknowledgement
We acknowledge Dorien Slabbers and Wietze Pasma for their contribution in data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.