
Abstract
Background
Emotional distress, symptoms of depression and anxiety, is common among patients after a myocardial infarction (MI), and is associated with an increased risk of cardiovascular morbidity. Real world population data on factors associated with emotional distress in MI patients are scarce. The aim was to determine factors associated with incident emotional distress two and 12 months post MI respectively, and with persistent emotional distress, versus remittent, in patients <75 years old.
Design
This was a registry-based observational study.
Methods
Data from the national SWEDEHEART registry on 27,267 consecutive patients with a first-time MI, followed up at two and 12 months post MI (n = 22,911), were included in the analyses. Emotional distress was assessed with the EuroQol-5D questionnaire. Several candidate sociodemographic and clinical factors were analysed for their association with emotional distress in multivariate models.
Results
Symptoms of emotional distress were prevalent in 38% and 33% at two and 12 months post MI respectively. At both time-points, previous depression and/or anxiety, readmission for new cardiovascular event, female gender, younger age, born outside the neighbouring Nordic countries, smoking and being neither employed nor retired showed the strongest associations with emotional distress. Other factors related to medical history, the MI and its care or were only modestly associated with emotional distress. Persistent emotional distress was associated with younger age, female gender, smoking and being born outside of the Nordic countries.
Conclusion
Previous depression/anxiety, female gender, younger age, smoking, born outside of the Nordic countries, neither employed nor retired and readmission due to cardiovascular events were strongly associated with emotional distress post MI. These factors may be of relevance in tailoring rehabilitation programmes.
Introduction
Emotional distress is common among patients with myocardial infarction (MI). Up to 30% report depressive symptoms, and symptoms of anxiety have been reported with similar frequency.1,2 Depression and anxiety are both associated with poor quality of life and higher healthcare costs, as well as increased risk of new cardiac events and mortality.3–6 In particular, persistent depression and anxiety seems to be related to a higher risk for adverse events.5,7 Although anxiety and depression have distinct features, they are moderately to strongly correlated, and studies suggest that as a risk-factor in the coronary heart disease (CHD) population, a general disposition toward emotional distress may be more important than the expression of any specific negative affect.8,9 Despite guidelines for managing psychosocial risk-factors, such as emotional distress, aimed at improving prevention of recurrent cardiac events in patients with CHD, 10 less than one-third of depressed post MI patients are recognized. 11 Identifying MI patients with emotional distress is highly relevant to cardiac rehabilitation and delineating factors that indicate high-risk might elevate the chance of successful rehabilitation through tailored treatment, especially since they may benefit both emotionally and in cardiac prognosis from, for example, physical exercise. 12
Previous studies on factors associated with emotional distress in post MI patients have mainly focused on depression. Factors such as age, gender, diabetes, smoking, left ventricular ejection fraction (LVEF), previous history of depression or anxiety and type D personality have been suggested, but findings are heterogeneous and sometimes conflicting.13–22 Anxiety has been less studied but one study found that negative feelings, type D personality and anxiety sensitivity, but not clinical factors, were associated with anxiety. 23
Risk markers of persistent depression and anxiety up to 12 months post MI have been more rarely studied, with conflicting results. Young age and female gender have been found to be associated with persistent depression and/or anxiety in some studies13,24 but not in others.18,23,25 Moreover, previous studies have shown that history of depression,18,24 frequent angina, recurrent MI, 13 type D personality,18,23 negative affectivity and anxiety sensitivity 23 are factors related to persistent depression and/or anxiety. These studies, however, have often been underpowered and have investigated personality factors that require expertise and specialized screenings, which are rarely available in the cardiac clinical setting.
To our knowledge, no studies have examined associations of incidental and persistent emotional distress in a high powered, real world population of first time MI patients <75 years old. The aims of this study were to investigate which factors are associated with emotional distress in first-time MI patients, at two and 12 months post MI, as well as factors associated with persistent emotional distress, compared with remittent, during the first year post MI.
Methods
Data sources
Data from the SWEDEHEART national quality registers for cardiac care, which covers approximately 90% of all MIs in Sweden, was used. 26 The Register of Information and Knowledge about Swedish Heart Intensive Care Admissions (RIKS-HIA) sub-register contains data on >100 historical, acute cardiac care and discharge variables from patients admitted to any cardiac care unit (CCU) in Sweden. 26 The register has an excellent quality. When comparing data from RIKS-HIA with hospital records of randomly chosen patients at different hospitals an average agreement of 95% was found and all variables are standardized. 26 The Secondary Prevention after Heart Intensive Care Admission (SEPHIA) sub-register collects data on patients <75 years old with a coverage of almost 80%. 27 As part of the SEPHIA follow-up, patients are interviewed by a nurse or physician during an outpatient visit or via telephone for completion of a questionnaire on two occasions: 6–10 weeks (two-month follow-up) and 12–14 months post MI (12-month follow-up). RIKS-HIA and SEPHIA data were linked to the National Patient Register, which records all diagnoses given at inpatient and outpatient hospital visits.
The study was conducted with approval from the regional ethics committee in Uppsala, Sweden (Dnr: 2013/478).
Study population
Demographic and clinical characteristics of patients with a myocardial infarction by emotional distress symptoms.

Unless otherwise specified, data are shown as n (%) of patients; missing data are due to lack of information in registers.
Some emotional distress corresponds to response category 2 and 3 and no emotional distress corresponds to response category 1 in the EuroQol-5D item pertaining to emotional distress.
Within six months prior to myocardial infarction.
ICD codes F20–29.
Bleeding and/or cardiogenic shock.
1) Beta blockers, 2) statins, 3) other lipid lowering drugs, and 4) angiotensin-converting enzyme inhibitor or angiotensin II receptor blockers.
During the first 30 days.
Subsamples; 20,766 patients at two months and 17,234 patients at 12 months as type of infarction has been recorded only since 2008.
CABG: coronary artery bypass graft; CV: cardiovascular; HR: heart rate; LVEF: left ventricular ejection fraction; NSTEMI: non-ST-segment elevation myocardial infarction; PCI: percutaneous coronary intervention; STEMI: ST-segment elevation myocardial infarction
Outcome measures
The EuroQol-5D (EQ-5D) assesses health-related quality-of-life with five questions. 28 The following question pertains to emotional distress: ‘Please indicate which statements best describe your own health state today.’ (1) ‘I am not anxious or depressed’, (2) ‘I am anxious or depressed to some extent’, (3) ‘I am extremely anxious or depressed’. Due to a small proportion reporting extreme anxiety and depression, the second and third response were combined to compare individuals who reported some emotional distress versus no emotional distress. 29 Persistent emotional distress was defined as patients reporting emotional distress at both the two- and the 12-month assessment. Remittent emotional distress was defined as patients reporting emotional distress only at the two-month assessment. The emotional distress domain in EQ-5D has been validated and found to be moderately associated with the Beck Depression Inventory, the Beck Anxiety Inventory 30 and diagnostic interviews for major depressive episodes and/or anxiety disorders. 31 Symptoms of emotional distress in the EQ-5D are more common among patients with major depression alone than those with anxiety disorders alone, but most common among those with both depression and anxiety. 31 The EQ-5D has been used in several studies on cardiovascular disease and is considered a valid instrument in this population. 29
Exposure variables
Sociodemographic and clinical factors potentially associated with emotional distress were obtained from RIKS-HIA at the time of the index MI. Sociodemographic variables included age, gender, employment status (categorized into employed, retired, and other, of which the last includes being on sick leave, unemployed or studying) and smoking (never, former smoker (quit > 1 month ago) or current smoker). Medical history included diabetes, stroke, hypertension and hyperlipidaemia. Data obtained on admission included chest pain, dyspnoea, Killip class, cardiac arrest and heart rate. Atrial fibrillation was estimated by electrocardiography (ECG) at discharge. LVEF was assessed during the hospitalization. Complications during hospitalization were defined as bleeding and/or cardiogenic shock under medical care. Length of hospital stay was defined as the time between dates of CCU admission and discharge. Discharge medication coverage consisted of: (1) beta blockers, (2) statins, (3) other lipid lowering drugs and (4) angiotensin-converting enzyme inhibitor or angiotensin II receptor blockers. Aspirin was not included since it was prescribed to more than 99% of the patients. In-hospital interventions consisted of coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), thrombolytics or no in-hospital intervention. In the case of first thrombolytics and then PCI, PCI was chosen. Readmission was any readmission due to angina, MI, heart failure, other cardiac disease, bleeding complication or stroke within 30 days after discharge. Hospital size was based on its number of MIs treated in the same year as the respective patient. Type of MI (ST-segment elevation MI/non-ST-segment elevation MI) was based on ECG at intake.
Country of birth was obtained from the National Patient Register and categorized into three groups: Sweden, the Nordic countries (Finland, Norway, Denmark and Iceland) and the rest of the world. Psychiatric diagnoses, given at specialized inpatient and outpatient care, within six months prior to the MI, obtained from the same registry, included depression and/or anxiety (ICD-10 codes F30-39 and F40-48), substance abuse (F10-19) and schizophrenia or similar diagnosis (F20-29).
Statistical analysis
Statistical analyses were conducted with SAS version 9.4 (Cary, NC, USA) and R version 3.3.2 (Vienna, Austria). Chi-square- and t-tests were performed for all baseline measures comparing patients with and without emotional distress. Logistic regression models were applied in the analysis of the outcomes; two-month, 12-month and persistent emotional distress. In the analyses of two-and 12-month emotional distress, no emotional distress was the reference, whilst when analysing persistent emotional distress remittent emotional distress was the reference. In the fully adjusted model all the potential exposures were added at the same time. Sensitivity analyses were performed after multiple imputation of exposure variables through mass imputation via chained equations and predictive mean matching. 32
Results
At two-month follow-up, the mean age of the patients was 62 years, 73% were men, 46% were working, 32% smoked and 86% were born in Sweden. Furthermore, 3% of the patients had been diagnosed with depression and/or anxiety within six months prior to their MI, 56% had normal LVEF at discharge and 7% were readmitted within the first 30 days (Table 1). At 12-month follow-up, patients showed similar characteristics. Emotional distress was reported by 38% at two months and by 33% at 12 months. Strong emotional distress corresponding to ‘I am extremely anxious or depressed’ on EQ-5D was reported by 4% and 3%, respectively. Of the 22,882 patients with complete data at both two and 12 months post MI, emotional distress was reported at two months by 8493 patients. Of these, 5008 (59%) patients were also reporting emotional distress at 12 months (persistent emotional distress). Persistent emotional distress was thus reported by 22% of the complete sample.
Associations of emotional distress in multivariate analyses
Crude and adjusted associations of incident emotional distress and adjusted associations of persistent emotional distress versus remittent emotional distress.
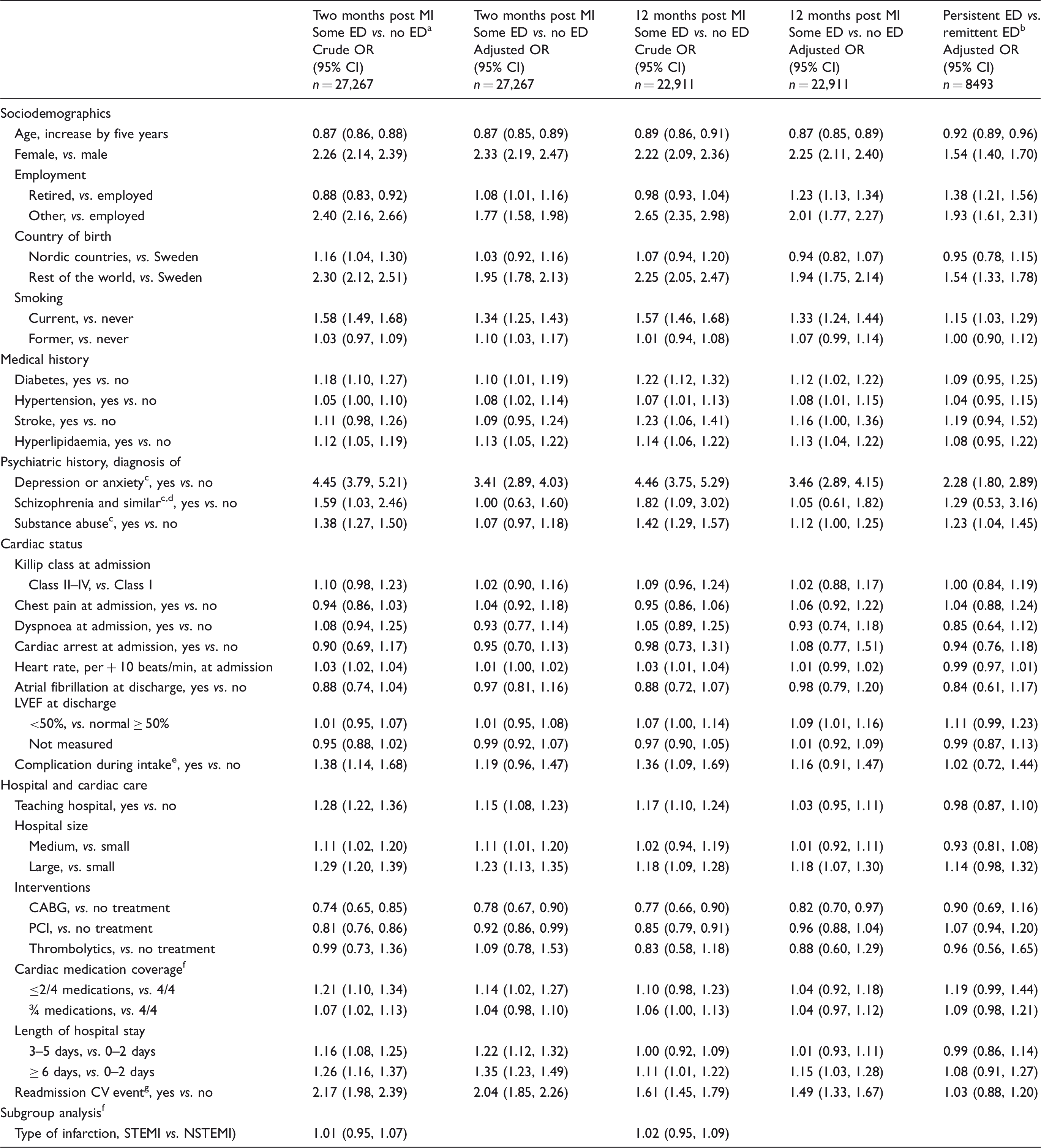
Some emotional distress corresponds to response category 2 and 3 and no emotional distress corresponds to response category 1 in the EuroQol-5D item pertaining to emotional distress.
Persistent emotional distress corresponds to some emotional distress at both two and 12 months, remittent emotional distress corresponds to some emotional distress at two months only.
Within six months prior to myocardial infarction.
ICD codes F20–29.
Bleeding and/or cardiogenic shock.
1) Beta blockers, 2) statins, 3) other lipid lowering drugs, and 4) angiotensin-converting enzyme inhibitor or angiotensin II receptor blockers.
During the first 30 days.
Subsamples; 20,766 patients at two months and 17,234 patients at 12 months as type of infarction has been recorded only since 2008.
CABG: coronary artery bypass graft; CI: confidence interval; CV: cardiovascular; ED: emotional distress; LVEF: left ventricular ejection fraction; MI: myocardial infarction; NSTEMI: non-ST-segment elevation myocardial infarction; OR: odds ratio; PCI: percutaneous coronary intervention; STEMI: ST-segment elevation myocardial infarction
Persistent emotional distress, as compared with remittent, was associated with previous diagnoses of depression and anxiety (2.28, 95% CI 1.80, 2.89), substance abuse (1.23, 95% CI 1.04, 1.45), female gender (1.54, 95% CI 1.40, 1.70), younger age (0.92, 95% CI 0.89, 0.96), being retired (vs. employed) (1.38, 95% CI 1.21, 1.56), being neither employed nor retired (vs. employed) (1.93, 95% CI 1.61, 2.31), born outside of the Nordic countries (1.54, 95% CI 1.33, 1.78) and current smoking (1.15, 95% CI 1.03, 1.29).
Discussion
In this study, using a population-based registry of Swedish first MI patients, previous diagnosis of depression and/or anxiety, sociodemographic variables and readmission due to cardiovascular events were found to have the strongest association with emotional distress at two and 12 months post MI. Persistent emotional distress was even more strongly associated with sociodemographic factors and previous depression and anxiety than remittent emotional distress. The prevalence of emotional distress post MI is consistent with previous reports. Further, out of those reporting emotional distress at two months, the majority (59%) reported persisting symptoms at 12 months post MI.
As mentioned, the prevalence of moderate to severe emotional distress post MI corroborates earlier studies reporting depressive symptoms being present in 10% to 47% of post MI patients 1 and anxiety symptoms in, similarly, 13% to 60%. 2 The prevalence of some emotional distress, assessed with EQ-5D, in the general Swedish population aged 50–70 years is between 27% and 32%. 33 Thus, emotional distress seems more common in MI patients, which might be due both to selection, in that depression and anxiety are risk-factors for developing a MI, and to a reaction to the MI itself.1,3
A previous diagnosis of depression and anxiety was most strongly associated with emotional distress post MI, which is in agreement with previous studies.13,15,18 Clearly patients with a history of emotional distress are vulnerable to reporting emotional distress post MI.
The strong association between emotional distress and readmission due to cardiovascular events has been described before, 14 for which there are several potential explanations. First, emotional distress is likely a reaction to the negative physical and psychological experience of having recurrent cardiovascular events after the initial MI. Second, MI patients with emotional distress are also more likely to experience and report chest pain and might have a lower threshold for emergency visits and readmissions. 34 Third, emotional distress is a risk-factor for cardiovascular events. 3
Sociodemographic characteristics showed strong associations with emotional distress in our study. First, women seem to report more emotional distress. This is also true for the general population where depression is almost twice as common in women. 35 Further, younger age was a risk-marker of emotional distress, consistent with results from previous studies of the MI population.13,16,36 The reason for this is unknown but might be due to a similar pattern in the general population33,35 as well as to stronger emotional reaction to the MI itself if younger. Moreover, being born outside the Nordic countries was also associated with emotional distress post MI. Immigrants have a higher prevalence of emotional distress than those born in Sweden, possibly due to previous traumatic events, such as war, prior to immigration and adverse circumstances in their new country. 37 Smoking was associated with emotional distress, confirming earlier studies.17,38,39 The reason for this is still unclear but two pathways have been suggested, the first involving common or correlated risk-factors, and the second a direct path in which smoking increases the risk of depression. 40 Being retired or belonging to the category of ‘other’ (sick leave, unemployment and students) was associated with more emotional distress. The retired group also includes patients on disability pension, which could perhaps influence the results. Sick leave or unemployment might lead to emotional distress or vice versa.
Being discharged from teaching hospitals or larger hospitals was associated with emotional distress. This might be due to the patient mix, in that these hospitals often receive more complicated cases compared with smaller hospitals. Unmeasured risk-factors might also be more common in the catchment areas of teaching or larger hospitals. For example, psychiatric disorders seem to be more present in urban areas. 41 One might also speculate that small hospitals provide more personalized care post MI, which might reduce self-rated emotional distress.
A longer hospital stay was associated with emotional distress, in agreement with two previous studies.15,24 This might reflect more severe cardiac disease, co-morbidities, or complications unmeasured in our study, as well as the possibility of emotional distress or social problems preventing discharge. Except for readmission due to cardiovascular events and length of hospital stay, we did not find an association between emotional distress and markers of cardiac disease severity such as Killip class, atrial fibrillation, cardiac arrest on admission or level of LVEF during the index MI. A robust association between LVEF and emotional distress has not been found in previous studies,15,23 with two exceptions.16,22 However, Doyle et al. 22 found a relation with LVEF only in men. That study used a lower cut-off level as reference (LVEF < 30% compared with LVEF < 50 % in the present study) and evaluated diagnosed depression. Additionally, low LVEF measured at discharge might improve during the first months and may therefore not affect emotional distress later.
CABG and PCI were associated with less emotional distress compared with no intervention at two months post MI, although the association was not seen at 12 months. These interventions are likely to have a health-promoting effect on cardiac status and symptom relief, and in turn result in less emotional distress. However, systematic selection due to doctors refraining from treatments in severely sick patients with concurrently more emotional distress is also possible. Van Melle and colleagues found a similar preventive effect of CABG (but not PCI) on emotional distress three months post MI. 16 No study has investigated this at 12-month follow-up.
Patients with persistent emotional distress, which might be the clinically most important group, differed from remittent emotional distress only in association with sociodemographic factors with the exception of having had a previous diagnosis of depression, anxiety or substance abuse. Studies on factors related to persistent depression or anxiety, including up to a year post MI, are few and most often small.13,18,23,25 Prior depression has been found to be associated with persistent depression in one study, 18 and female gender and younger age have been reported in one study each.13,25 Our study is possibly the only one assessing persistent emotional distress with enough power to identify a range of factors that can indicate enhanced risk for persistent emotional distress. This study found a range of factors associated with emotional distress. It is unknown whether an accumulation of these factors in the same individual further increases the risk of emotional distress. Furthermore, whether the predictive factors are the same in women and in men is not known.
Strengths and limitations
Emotional distress was not estimated through structured diagnostic interviewing or an established multi-item questionnaire. However, the question from EQ-5D about anxiety and depression has been validated against established instruments with good results.29,30 Importantly, not only diagnosed depressive and anxiety disorders but also sub-diagnostic symptoms are associated with subsequent cardiac events.5,7 Furthermore, psychological vulnerabilities as cause of emotional distress, such as personality, anxiety sensitivity and previous negative life events, were not considered in this study, yet they have been identified as important factors for depression and anxiety.18,23,42 However, all factors used in this study are readily available for nurses and physicians at the CCU, whereas assessing psychological vulnerability requires special assessment, competence and resources. These factors might be useful to identify patients that might benefit from further screening of emotional distress and, if needed, referral to appropriate care.
The prevalence of previous diagnosis in this study was fairly low, at 3%. Only diagnoses registered in specialist care within six months prior to the MI were included in our analysis. This probably reflects the more severe cases, hence the lower percentage. Further, a limitation of this study was lack of socioeconomic status variables except for occupational status, which may affect both depression and anxiety.
It should be highlighted that this is an exploratory study with observational data, which prohibits us to draw any firm conclusions regarding causality. Though the longitudinal nature of the data is a strength, causal modelling of the identified associations deserves further research attention.
Despite limitations, this real world, high-quality population database with nationwide coverage is unique. It generally reduces problems with selection bias and increases the potential generalizability. The large sample size also allowed for both precise statistical modelling and exploratory analysis on a wide range of exposures.
In conclusion, this is to our knowledge the first study investigating the association between symptoms of depression and anxiety in a nationwide, real world sample of post MI patients with a range of exposure variables easily obtained in a clinical setting. Sociodemographic factors, previous psychiatric diagnoses and readmission due to cardiovascular events were the most important factors related to emotional distress. In contrast, cardiac and clinical factors seem to be less important. When it comes to persistent emotional distress it was even more strongly associated with sociodemographic factors. Although exploratory and in need of further research, our findings might help clinicians to identify patients at high risk of short term and persistent emotional distress post MI.
Supplemental Material
Supplemental material for Factors associated with emotional distress in patients with myocardial infarction: Results from the SWEDEHEART registry
Supplemental material for Factors associated with emotional distress in patients with myocardial infarction: Results from the SWEDEHEART registry by Fredrika Norlund, Claudia Lissåker, John Wallert, Claes Held and Erik MG Olsson in European Journal of Preventive Cardiology
Footnotes
Author contribution
FN, CL, JW, CH and EO designed of the study. JW and EO contributed to the acquisition of the data, FN, CL, JW, CH and EO analysed and interpreted the data. FN drafted the manuscript. CL, JW, CH and EO critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Heart and Lung Association and is part of the strategic research program U-CARE, funded by Swedish Research Council.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.