
Abstract
Background
There is broad consensus that regular physical activity yields major health benefits. However, current guidelines on physical activity are mainly aimed at middle-aged adults. It is unclear whether physical activity also translates into cardiovascular health benefits in older adults. Therefore, we aimed to compare the association between different levels of physical activity and the risk of cardiovascular disease (CVD) in elderly to middle-aged individuals.
Methods
We analysed data from the EPIC Norfolk prospective population study. Cox proportional hazards models were used to analyse the association between physical activity levels and time to CVD events in three age categories (<55, 55–65 and >65 years). Interaction between age categories and physical activity levels was assessed.
Results
Analyses were based on 24,502 study participants aged 39–79 years. A total of 5240 CVD events occurred during 412,954 person-years follow-up (median follow-up was 18.0 years). Among individuals aged over 65 years, hazard ratios for CVD were 0.86 (95% confidence interval (CI) 0.78–0.96), 0.87 (95% CI 0.77–0.99) and 0.88 (95% CI 0.77–1.02) in moderately inactive, moderately active and active people, respectively, compared to inactive people. Among people aged 55–65 and less than 55 years, the associations were directionally similar, but not statistically significant. The interaction term between physical activity levels and age categories was not significant (P = 0.38).
Conclusion
The inverse association between physical activity and the risk of CVD was significant in elderly and comparable with middle-aged individuals. In addition, we observed that modest levels of physical activity confer benefits in terms of CVD risk, compared to being completely inactive.
Introduction
In the early 1960s, Morris investigated the association between physical activity (PA) and cardiovascular disease (CVD) prevalence. 1 Since then, many studies have confirmed that PA is associated with major health benefits.2–5 However, despite accumulating evidence of health benefits from PA, there is a worldwide trend towards a more sedentary lifestyle and less PA.6,7 In many western countries, the population is ageing rapidly, 8 with profound consequences for public health. Elderly people may have more difficulty engaging in PA compared to middle-aged adults due to frailty and comorbidity. Several recent guidelines and initiatives have recommended more engagement in PA in order to improve public health.9–12 The World Health Organization (WHO) stated that substantial health benefits can be achieved by moderate intensity PA of at least 150 minutes a week, or vigorous intensity PA of at least 75 minutes a week, or any combination of moderate and vigorous intensity PA. 9 However, it is also emphasised that any amount of PA leads to health benefits.
Current PA guidelines are mainly aimed at middle-aged individuals. It is less well established whether different PA intensities also translate into cardiovascular health benefits in elderly people. We hypothesised that elderly individuals benefit equally from PA compared to middle-aged individuals regarding the risk of CVD. We tested this hypothesis in the European Prospective Investigation into Cancer (EPIC) Norfolk prospective population study.
Methods
The EPIC Norfolk cohort is a prospective population study, which is part of the 10-country collaborative EPIC study. The design, methods and baseline characteristics have been described previously. 13 The cohort was primarily designed to assess dietary and other determinants of cancer, yet additional data were obtained to investigate determinants of other chronic diseases, particularly CVD. Participants aged 39–79 years were recruited from registries of general practices in the area of Norfolk, and completed a detailed health and lifestyle questionnaire at the baseline survey between 1993 and 1997. They underwent standardised physical examination and blood samples were obtained. Measurements were performed by trained nurses. PA was assessed using a questionnaire to quantify activities in occupational and leisure time domains, and was categorised into four levels: active, moderately active, moderately inactive and inactive, see Supplementary material. The PA questionnaire has been validated against estimated energy expenditure from individually calibrated heart rate monitoring.14,15 Standardised measurements were obtained for body mass index (BMI), blood pressure and serum total cholesterol. Smoking status was derived from questionnaires. 13
Hospitalisation or death from cardiovascular events was identified if the corresponding International Classification of Disease (ICD)-10 code was recorded as the underlying cause of hospitalisation or mortality. Hospitalisations were identified by linking the participant’s unique National Health Service number with the East Norfolk Health Authority (ENCORE) database. The ENCORE database identifies all hospital contacts throughout England and Wales for residents of Norfolk. Death certificates were coded by trained nosologists according to the ICD-10. Deaths or hospitalisations were attributed to coronary heart disease (CHD) if the underlying cause was coded as ICD-10 codes 120–125, which encompass the clinical spectrum of CHD including unstable angina, stable angina and myocardial infarction. Deaths or hospitalisations were attributed to stroke if the underlying cause was coded as ischaemic (I63) or haemorrhagic stroke (I60–62). CVD was defined as either CHD or stroke. The follow-up was censored on 31 March 2015. The study protocol was approved by the Norwich District Health Authority Ethics Committee. All participants gave written informed consent.
Statistical analysis
Study participants with missing data for PA and those who had prevalent CHD or stroke at baseline were excluded from this analysis. Descriptive data were presented as a percentage and frequency for categorical variables, as mean and standard deviation for continuous variables with a normal distribution, and as median with interquartile range for continuous variables with a non-normal distribution. Age was categorised into three categories: less than 55 years, 55–65 years and over 65 years. A Cox proportional hazards model was used to assess the association between the PA categories and the risk of cardiovascular events in all three age categories. Hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for time to the occurrence of cardiovascular events were calculated for study participants classified as active, moderately active and moderately inactive, using those classified as inactive as the reference category. Analyses were performed for total CVD events (i.e. CHD and stroke combined). HRs were calculated according to an unadjusted regression model as well as model 2 that was adjusted for socioeconomic status which was based on social class (professionals, managerial and technical occupations, non-manual skilled workers, manual skilled workers, partly skilled workers and unskilled workers), age, sex and smoking status (current, former or never), and model 3 that was adjusted for socioeconomic status, age, sex, smoking status, systolic blood pressure, diabetes, BMI, low-density lipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol. Interactions between PA and age, and PA and sex were tested by including the relevant parameters in the Cox regression model. The attributable risk fraction was based on the following calculation: incidence of CVD (exposed*) – incidence CVD (active)/incidence of CVD (exposed*). Exposed was defined by PA levels inactive or moderately inactive or moderately active. In order to assess the shape of the relationship between PA categories and the hazard of CVD, we used a log-likelihood ratio test to compare Cox regression models assuming a (log-)linear association of PA category, and allowing a different association for each category compared with the inactive group. A significant difference between the fit of the two models was assumed to support departure from a (log-)linear relationship between PA categories and the hazard of CVD. Statistical analyses were performed using SPSS version 23 (IBM Corp., Armonk, NY, USA). A P value less than 0.05 was considered statistically significant.
Results
The EPIC Norfolk cohort comprised 25,639 study participants. A total of 1136 (4%) were excluded because of prevalent CHD or stroke or prevalent CHD and stroke or missing data in any of the two, and a further one had missing PA data. Thus 24,502 study participants were available for the current analysis. Median (interquartile) follow-up was 18.0 years, yielding a total of 412,954 person-years follow-up. A total of 4450 (18.2%) participants experienced a CHD event during follow-up, 1231 (5.0%) experienced a stroke event, and 441 (1.8%) experienced both a CHD and a stroke event. Thus, a CVD event occurred in 5240 study participants.
Baseline characteristics in EPIC Norfolk participants.
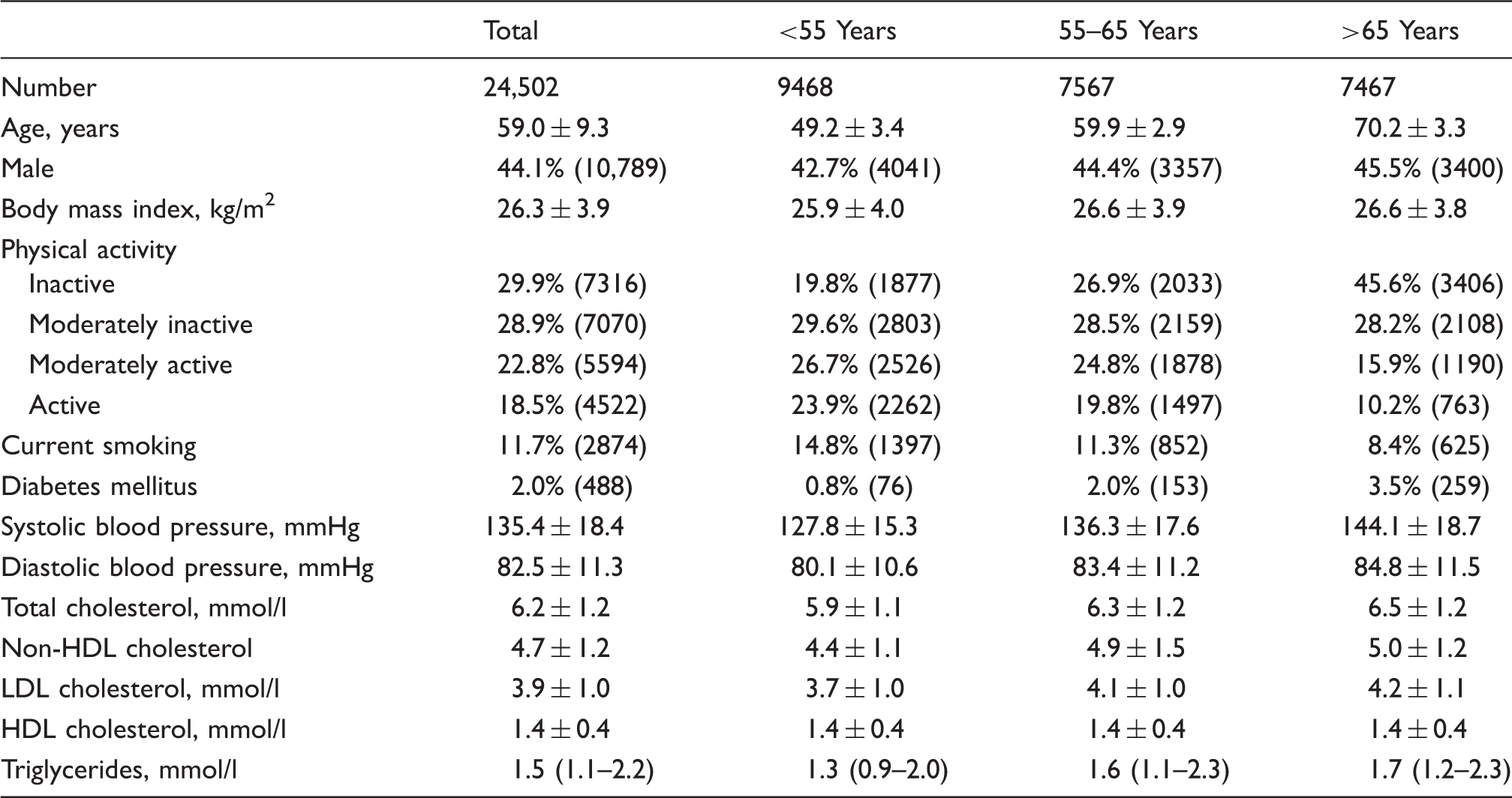
Data are presented as percentage (number) for categorical variables, mean ± standard deviation for ontinuous variables with normal distribution, or median (interquartile range) for continuous ariables with a non-normal distribution. Data were available in up to 24,502 study participants.
For age categories <55, 55–65 and >65 years up to 9468, 7567 and 7467 study participants were available, respectively.
LDL: low-density lipoprotein; HDL: high-density lipoprotein; non-HDL cholesterol: total cholesterol minus HDL cholesterol.
Baseline characteristics by physical activity categories and age categories.
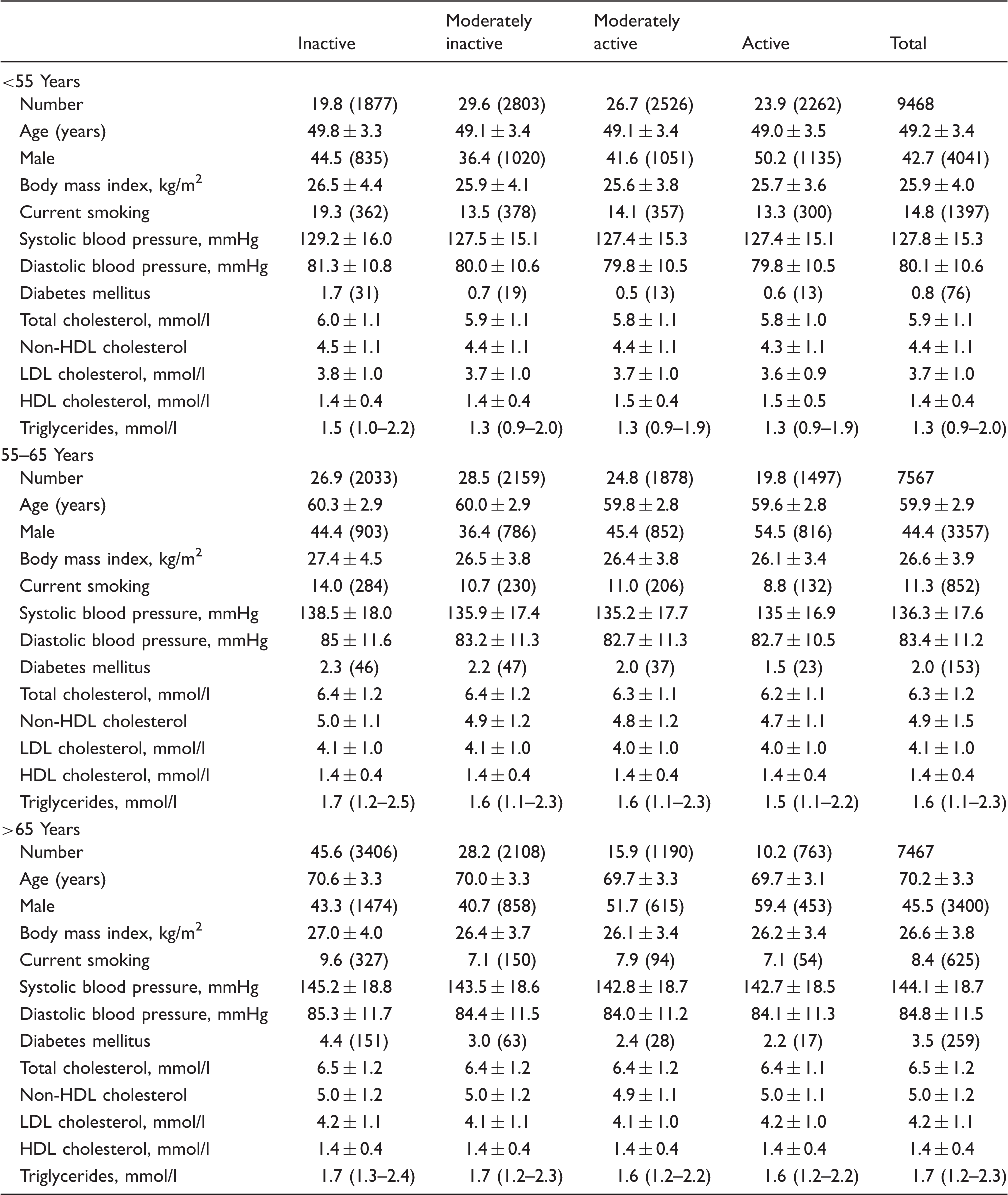
Data are presented as percentage (number) for categorical variables, mean ± standard deviation for continuous variables with normal distribution, or median (interquartile range) for continuous variables with a non-normal distribution.
LDL: low-density lipoprotein; HDL: high-density lipoprotein; non-HDL cholesterol: total cholesterol minus HDL cholesterol.
Risk of cardiovascular disease events in EPIC Norfolk participants; total person-years follow-up = 412,954.
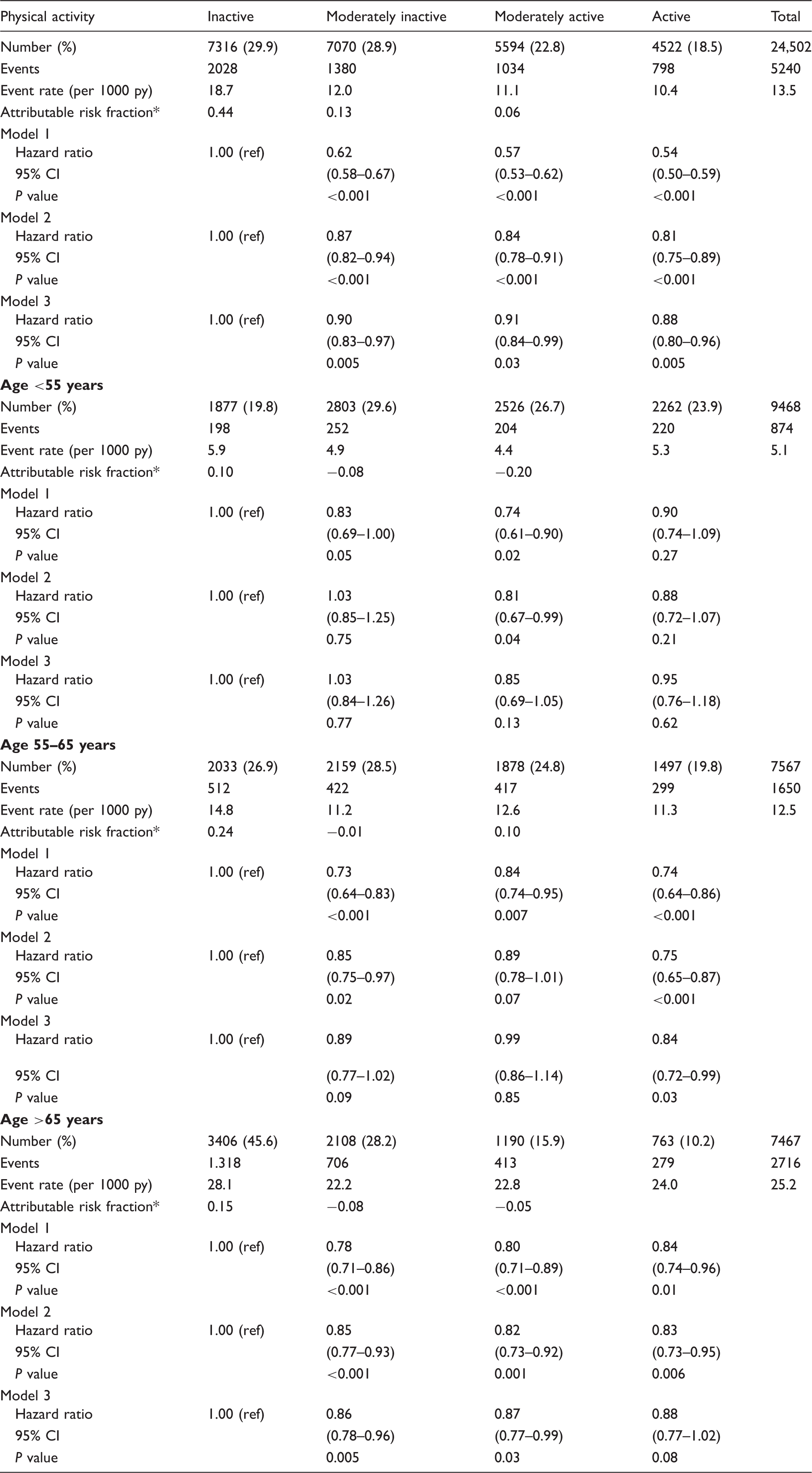
Model 1 unadjusted.
Model 2 adjusted for socioeconomic status, age, sex and smoking status.
Model 3 adjusted for socioeconomic status, age, sex, smoking status, systolic blood pressure, diabetes, BMI, LDL cholesterol and HDL cholesterol.
CI: confidence interval; py: person years; BMI: body mass index; LDL: low-density lipoprotein; HDL: high-density lipoprotein.
Attributable risk fraction*: event rate (per 1000 py) per physical activity level.
There was no statistical evidence for a better fit of the regression model using discrete PA categories versus test for linear trend across categories in both Cox regression models 2 and 3 (–2 log likelihood difference 3.83 and 3.48; P values 0.15 and 0.18, respectively), when adjusted for socioeconomic status. There was statistical evidence of a threshold (2 log likelihood difference 6.96, P value 0.03, when not adjusted for socioeconomic status (data shown in Supplementary Table 1b).
Discussion
In this analysis among apparently healthy participants of the EPIC Norfolk prospective population study, elderly people appeared to benefit at least comparably from PA compared to middle-aged individuals regarding the risk of CVD. Secondly, we observed that even those participants who were moderately inactive had a substantially lower CVD risk than those who were completely inactive, suggesting that even modest engagement in PA may be associated with a substantially lower risk of CVD in the elderly.9–11 These observations are consistent with, but also extend on, the findings from a previous analysis in EPIC Norfolk, but in that analysis, participants were only stratified into groups under 65 and over 65 years of age, and the number of CVD events was lower due to a shorter follow-up compared to the current analysis (average 8 vs. 16.9 years). 16
As expected, we observed that elderly people had lower levels of PA and higher CVD event rates compared to middle-aged individuals. However, a directionally similar inverse association between PA and CVD risk was observed in all age categories. Health benefits from PA in middle-aged and older individuals have previously been demonstrated. Among 267,153 people enrolled in the ‘45 and up study’ there was an inverse association between PA and all-cause mortality in the age categories 45–54 and 55–64 years. The association between PA and mortality among elderly people (65–75 years) was not statistically significant. However, there was no statistical evidence for a difference between the age categories (P value for interaction >0.05). 17 In the National Cancer Institute Cohort Consortium of six population studies, there was an inverse association between PA and the risk of mortality among all age groups (<50, 50–59, 60–69, >70 years). There was statistical evidence for a difference between age categories (P value for interaction <0.001) but, if anything, the association between PA and mortality was stronger rather than weaker among those aged over 70 years old, which is consistent with our findings for CVD. However, Gulsvik et al. observed in a large cohort of 42 years’ follow-up that the population attributable fraction of no/low activity was consistent across all age groups. 18 In the current study, we observed that the decreased risk of CVD associated with PA was not as pronounced as reported by Soares-Miranda et al., 19 who found a significantly lower risk (by 51% and 70%, respectively) in individuals under 75 years and 75 years and over engaging in the highest intensity exercise.
We observed that the shape of the PA–CVD risk relationship does not appear to have a threshold when it was adjusted for socioeconomic status. However, when no adjustment for socioeconomic status was done, the shape of the PA–CVD risk relationship appears to have a threshold such that the largest step in terms of CVD risk is seen in completely inactive and moderately inactive people, which is consistent with the international consensus that ‘any PA is better than none at all’. Soares-Miranda et al. observed that low intensity exercise compared to no exercise intensity at all was associated with a significantly lower CVD risk among individuals aged 75 years and older. 19 Higher intensity PA levels yielded a comparably lower risk. Similar findings were reported by other large cohort studies. A pooled analysis from six studies comprising a total of 661,137 individuals showed that individuals engaging in any leisure time activity had a 20% lower mortality compared to individuals who did not report any PA across all age categories. 20 Furthermore, a combined analysis of the Harvard Alumni Health Study and the Women’s Health Study demonstrated that vigorous PA was not associated with lower CVD mortality risk compared to moderate intensity PA. 21 These findings indicate that health benefits are not restricted to those engaging in vigorous intensity PA, but that individuals exercising at lower intensity may also benefit. In our study we investigated total PA levels, not PA intensity. However, we observed that people doing some PA compared to being completely inactive had a lower CVD risk.
As there appeared to be a threshold between completely inactive and moderately inactive people in the relationship between PA and CVD risk, the avoidance of a sedentary lifestyle in general should be recommended. The association between PA and CVD risk was maintained at low levels of PA in age categories 55–65 and over 65 years. These observations suggest that in order to achieve cardiovascular health benefits from PA, elderly people should be encouraged to engage in at least some PA of low level. Huang et al. demonstrated that aerobic training in healthy sedentary elderly people yielded cardiorespiratory benefits. 22 However, elderly people with mobility impairment may be unable to meet the current PA recommendations; the benefits of low levels of PA may be of particular relevance to this group. Fitzgerald et al. reported that sedentary elderly people with mobility impairment also benefit from engagement in PA. 23 In their cross-sectional analysis, objectively measured PA with an accelerometer was inversely associated with the calculated risk of cardiac events. In general, health benefits can be achieved by changing a sedentary lifestyle into a more active lifestyle in all age categories. 24
Our study has several strengths. First, this analysis included a large proportion of individuals aged 65 years and older (n = 7467) with a long duration of follow-up, which allows us to observe a relatively large population of older age. Secondly, in EPIC Norfolk PA levels were derived from leisure time and work-related activities. Individuals could be engaged in different activities across the major life domains including leisure, occupation and transport. Daily PA may be underestimated if PA quantification is based on activities derived from only one life domain. Some limitations of our study should also be considered. PA was assessed by self-report, which is imprecise relative to more objective measurement tools. However, the PA questionnaire in EPIC Norfolk was validated against energy expenditure assessed by individually calibrated heart-rate monitoring.14,15
Notably, CVD events were exclusively based on ICD codes of the hospital discharge ENCORE register or the ICD death certification codes, and were not clinically validated events. Furthermore, our analysis included participants from 39 years of age and older, younger participants were not represented in the present analysis. However, health benefits are obtained by the maintenance of a physically active lifestyle that is adopted at young age.24–26
Conclusion
Our findings in the EPIC Norfolk population support current international guidelines and recommendations on PA including middle-aged and elderly people. In all age groups, even a little engagement in PA of moderate inactive level and not necessarily PA of vigorous level was associated with a substantially lower CVD risk compared to no PA at all; however, when adjusted for socioeconomic status this is only observed in elderly people. A broader array of public health, healthcare systems and communities should be involved in helping elderly people to engage in any PA of any level and to reduce a sedentary lifestyle.
Footnotes
Author contributions
SL, SMB and RP contributed to the conception and design of the work. SL, SMB, SS and SB contributed to the acquisition, analysis and interpretation of data for the work. SL and SMB drafted the manuscript. RL, KK, RP and NW critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
The authors wish to thank the participants and staff of the EPIC Norfolk prospective population study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SL is supported by a studentship from Unilever Corporate Research, UK. SJS, SB, and NJW are supported by the Medical Research Council (MC_UU_12015/1 and MC_UU_12015/3). SMB reported personal fees from Pfizer, outside the submitted work; RJGP reported personal fees from Sanofi Aventis, Boehringer Ingelheim, Amgen and AstraZeneca, outside the submitted work. The other authors declare that they have no known conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The EPIC Norfolk study is funded by Cancer Research UK grant number 14136 and the Medical Research Council grant number G1000143. The funders had no role in the study design, data collection, analysis, decision to publish or preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.