
Abstract
Background
Health literacy may constitute a modifiable determinant of health behaviour and affect cardiovascular disease prevention. This study investigates the associations between health literacy and health behaviour as well as health status.
Design
A cross-sectional study on a population-based sample of people with acute myocardial infarction, angina pectoris or stroke (N = 3116).
Methods
Health literacy was assessed using two dimensions from the Health Literacy Questionnaire: ‘understanding health information’ and ‘engaging with healthcare providers’. Health behaviour included physical activity, dietary habits, smoking, alcohol consumption and body mass index. Health status was examined using Short Form Health Survey 12 version 2 (four-week recall) (physical and mental components). We used regression analyses to examine the associations.
Results
‘Understanding health information’ was inversely associated with physical inactivity (odds ratio (OR) 0.48 (0.39;0.59), unhealthy diet (OR 0.64 (0.47;0.88)), underweight (OR 0.43 (0.21;0.89)) and obesity (OR 0.79 (0.63;0.99)). ‘Engaging with healthcare providers’ was inversely associated with physical inactivity (OR 0.64 (0.53;0.77)), less than healthy diet (OR 0.79 (0.64;0.96)) and daily smoking (OR 0.81 (0.66;1.0)). An increase in ‘understanding health information’ as well as ‘engaging with healthcare providers’ was associated with an increase in both physical and mental health status.
Conclusions
The findings suggest that aspects of health literacy are associated with health status and health behaviour in cardiovascular patients and should be considered in interventions regarding cardiovascular disease prevention.
Introduction
Successful cardiovascular disease prevention requires a high level of individual self-care competences. 1 Health literacy encompasses some of the skills required, such as the understanding of health information and active interaction with healthcare professionals. Health literacy is open to change through building skills or improving health services and may constitute a significant, modifiable determinant of self-care and health behaviour.2,3
Health literacy can be defined as people’s knowledge, motivation and competences to access, understand, appraise and apply health information in order to make judgements and take decisions in everyday life concerning health. 4
Low levels of health literacy have been associated with social determinants such as low educational level, low income, ethnic minority status and living alone.5–7 It has been hypothesized at a theoretical level, that health literacy is a dynamic outcome of socio-demographic as well as individual and environmental factors,8,9 manifesting itself in the interaction between individuals and the demands of complex healthcare systems. 4
A large Danish survey investigated dimensions of health literacy and found that between 8.8% and 20.2% of the general population find tasks related to understanding health information or engaging with healthcare providers difficult. 6 In another study it was shown that the proportion was significantly higher in individuals with cardiovascular disease, 10 and low health literacy has also been associated with increased risk of being limited by long-term health conditions. 5
In people with cardiovascular disease low education is associated with higher prevalence of many cardiovascular risk factors, 11 which may be due to lower awareness. 12 At any rate, low health literacy has been related to more adverse health behaviours13–15 and poor subjective health.5,13–18 However, all these studies were either small and/or investigated health literacy as basic skills of reading and understanding. No more comprehensive studies have explored these associations.
The aim of this study was to investigate the association between health literacy and health behaviour as well as health literacy and health status in people with cardiovascular disease.
Methods
Design, data collection and participants
This study is based on data from the Danish health and morbidity survey coined ‘How Are You? 2013’ describing health and health behaviour in the general population. The survey was conducted in Central Denmark Region, which is the residence of approximately 1.3 million people.
A random sample of 46,354 adults aged 25 years or above was drawn from the Danish Civil Registration System and they were invited to complete a comprehensive postal or web-based questionnaire. In all, 29,473 respondents (63.6%) completed the questionnaire. Of these, 3116 individuals reported cardiovascular disease, that is, current or previous diagnosis of acute myocardial infarction, angina pectoris, or stroke, and were included in the present study.
Measures
Health literacy
The Health Literacy Questionnaire (HLQ) is a comprehensive instrument measuring nine dimensions of health literacy. The questionnaire was developed using a grounded psychometric approach and has been shown to have strong measurement properties in diverse settings.19–22 The translation and cultural adaption from English into Danish has followed standardized procedures. 23
Due to limited space in the lengthy survey only two of the nine subscales were included in the survey, namely ‘Understanding health information well enough to know what to do’ and ‘Ability to actively engage with healthcare providers’. Each of the two subscales consists of five questions. Each response is indicated on a four-point scale: very difficult (1), difficult (2), easy (3), very easy (4). Scale scores were calculated as the mean score of the number of items answered in that particular subscale. If more than two items in a scale were unanswered, the scale score for that individual was regarded missing.
Health status
Health status was measured using the Short Form Health Survey 12 version 2 (four-week recall) (SF-12). The two summary measures – physical component summary (PCS) and mental component summary (MCS) – were each calculated and adjusted using norm-based methods developed with the general US population as reference, with a mean of 50 units and standard deviation of 10 units. 24
Health behaviour
Four different aspects of reported health behaviour were included (physical activity, dietary habits, smoking, alcohol consumption). Body mass index (BMI) was added as a proxy for long-term health behaviour.
Physical activity was measured as number of days per week with at least 30 min of physical activity and categorized as ‘very active’ (5–7 days), ‘active’ (2–4 days) and ‘inactive’ (0–1 days). Danish Health Authorities recommend 30 min of physical activity per day. 25
The Diet Quality Score was used to classify dietary habits. 26 The score is a 25-item validated questionnaire, developed in a Danish setting to evaluate diet in relation to cardiovascular risk. In line with the recommended scoring dietary habits were categorized as ‘unhealthy’ (1–3 points), ‘average’ (4–6 points) or ‘healthy’ (7–9 points).
Smoking was categorized as ‘daily smoker’, ‘occasional smoker’ (less than daily), ‘former smoker’ and ‘never smoked’.
Respondents were asked how many alcoholic drinks they drank on average per week, and high-risk alcohol consumption was considered weekly consumption above Danish Health Authority recommendations of 14/21 drinks for females/males, respectively. 27
BMI (weight/(height) 2 ) was calculated using self-reported weight (kg) and height (m) and classified as ‘underweight’ (BMI < 18.5), ‘normal’ (BMI 18.5–24.9), ‘overweight’ (BMI 25–29.9) and ‘obese’ (BMI ≥ 30).
Socio-demographic factors
Socio-demographic factors included gender, age, educational level, cohabitation status and ethnic background. Information on gender, age and ethnic background was collected from the Danish National Civil Registry. Ethnic background was defined as Danish if the respondent or at least one parent had Danish citizenship.
Educational level and cohabitation status were self-reported. Years of education was categorized as ‘low’ (1–10 years), ‘medium’ (11–14 years), ‘high’ (>15 years). Cohabitation was defined as respondents living with another adult.
Statistical analysis
To account for selection probabilities and response rates data were weighted prior to any research access using a model-based calibration approach based on information from Statistics Denmark on gender, age, municipality of residence and a number of social variables to represent the population of Central Denmark Region.
Each of the two HLQ subscales’ association with distinct socio-demographic factors has been established6,20,28 and we hypothesise that they cover distinct aspects of health literacy important for successful self-care of cardiovascular disease. Cronbach’s alpha was found high in both scales, α = 0.86 and α = 0.90 respectively, indicating high internal reliability.
The associations between the two HLQ subscales and health behaviours were analysed using logistic regression. High physical activity, healthy diet, never smoked, low-risk alcohol consumption and BMI within normal range were used as reference categories. For each health behaviour dummy variables were created including only respondents within a specific category and the reference category. Regression analyses were performed separately for each dummy variable. Odds ratios were adjusted for gender, age, ethnic background, educational level and cohabitation status.
The association between each of the two HLQ subscales and health status was examined using linear regression on the summary scores for PCS and MCS. The analyses were adjusted for gender, age, ethnic background, educational level and cohabitation status.
Level of significance was set at p < 0.05. All statistical analysis was performed using STATA version 14.
Ethics and approvals
Information about aim, voluntary participation and confidentiality was provided with the questionnaire. Voluntary completion of questionnaires constituted consent. The study was performed in accordance with the Helsinki Declaration. According to Danish law no specific ethic evaluation is required in survey studies such as this. The study has been approved by the Danish Data Protection Agency (ref. no. 2015-57-0002).
Results
General characteristics
Participant characteristics among responders reporting a cardiovascular disease.
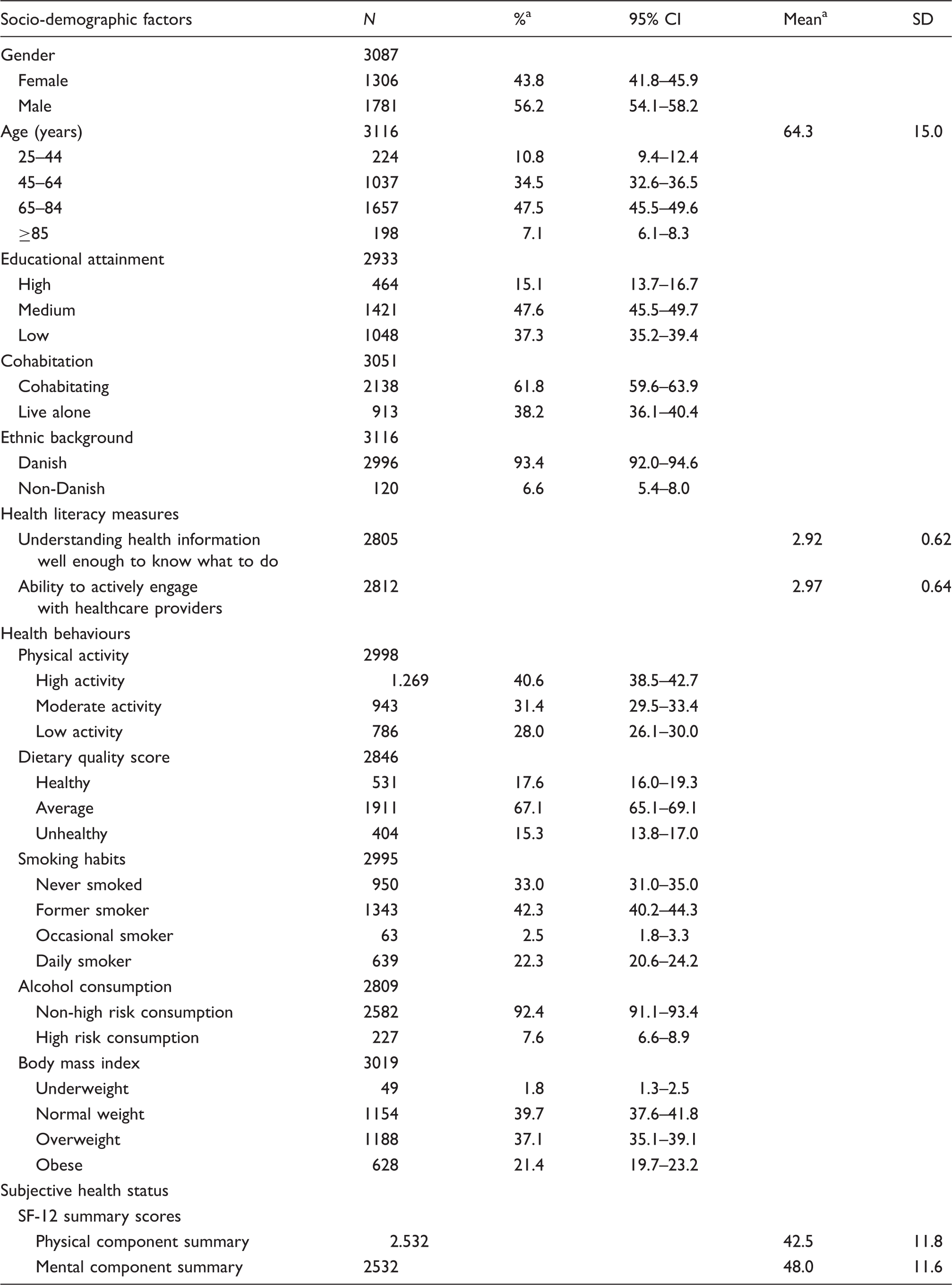
CI: confidence interval; SD: standard deviation; SF-12: Short Form Health Survey 12 version 2 (four-week recall)
All percentages and means are weighted based on register data to represent the population of Central Denmark Region, 2013.
Regarding health literacy, the mean scale score of ‘Understanding health information well enough to know what to do’ was 2.92, while the mean scale score of ‘Ability to actively engage with healthcare providers’ was 2.97.
Poor health behaviour was reflected in 28.0% of the study population reporting physical inactivity, 15.3% reporting unhealthy diet, 22.3% being daily smokers, 7.6% reporting high-risk alcohol consumption and 21.4% being obese (BMI ≥ 30).
SF-12 physical domains were generally scored below mental domains and the population had mean PCS of 42.5 and MCS of 48.0. The effect sizes using Cohen’s d on the standardized mean of 50 10 equal 0.75 (0.71;0.79) and 0.20 (0.16;0.24) respectively.
Health literacy and health behaviour
Associations between health behaviour and Health Literacy Questionnaire subscales.
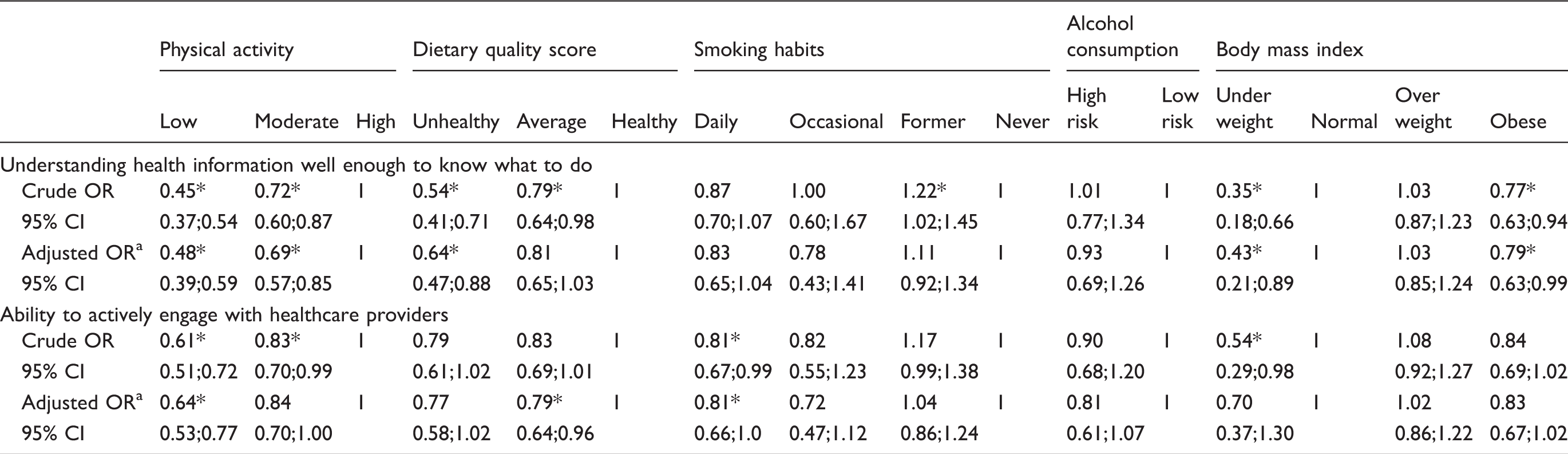
OR adjusted for gender, age, ethnic background, educational attainment and cohabitation.
OR: odds ratio; CI: confidence interval; *P < 0.05.
Similarly, in the adjusted analyses we found that a one-unit increase in mean scale score of ‘ability to actively engage with healthcare providers’ decreased the odds of being physically inactive (OR 0.64 (0.53;0.77)), eating a less than healthy diet (OR 0.79 (0.64;0.96)) and being a daily smoker (OR 0.81 (0.66–1.0)).
No association was found between health literacy competences and high-risk alcohol consumption.
Health literacy and health status
Associations between SF-12 summary scale scores and HLQ subscales.
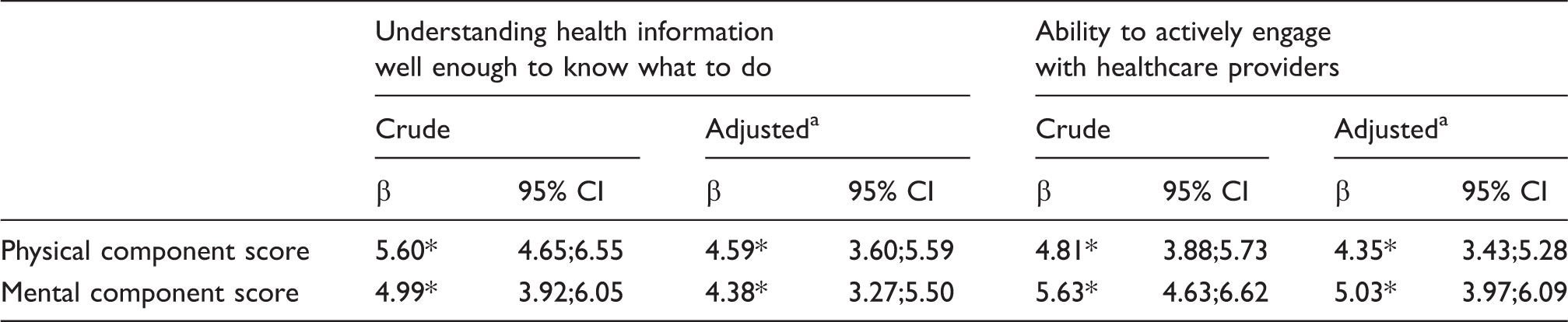
aβ adjusted for gender, age, ethnic background, educational attainment and cohabitation.
*p < 0.05
SF-12: Short Form Health Survey 12 version 2 (four-week recall); HLQ: Health Literacy Questionnaire; β: beta coefficient; CI: confidence interval
The association between the two HLQ subscales and PCS were significantly stronger than corresponding associations in the total survey population, while this is not the case for MCS (data not shown).
Discussion
In a large population of individuals with self-reported cardiovascular disease, we found significant associations between two aspects of health literacy and increased physical activity, healthier diet and higher self-reported health status. Also, for the ability to understand health information we found significant associations with better weight control, and for the ability to actively engage with healthcare providers we found significant associations with abstinence from smoking.
Strengths and limitations
To our knowledge, this is to date the largest and most comprehensive study examining the relationship between health literacy and health behaviour as well as health status in individuals with cardiovascular disease. The large sample size has allowed strong analyses even after controlling for multiple potential confounders.
Health literacy is a dynamic quality depending on a number of contextual, individual and situational factors.4,9 The demands for health literacy competences depend on the complexity of an individual’s condition and the health services provided, but the condition may also change the individual and social resources available and thus the ability to use such competences effectively. The cross-sectional nature of this study precludes any causal conclusions. Further research with longitudinal or qualitative designs may provide a better understanding of these issues.
The survey had a high response rate (63.3%) and the population weights used on the survey data prior to our analyses compensate to some extent for selection bias based on selection probabilities and socio-demographic as well as geographic differences in response rates.
However, low health literacy may decrease the motivation and ability to fill out the survey, as would other personal and health-related characteristics. Response rate in the eldest age group was low (43% in people aged > 85 years) and it is likely that people with severe chronic conditions may have refrained from returning the questionnaire. As a consequence, the health literacy level in our study may have been overrated.
The survey included three self-reported cardiovascular diseases and we did not make any comparison of reported cases with patient registers. Respondents’ knowledge of their condition and the lack of options such as chronic heart failure and heart valve conditions may have excluded relevant respondents from the population, reducing the power of our results.
To limit the length of the survey we were not able to include all nine subscales of the HLQ in this study. Conclusions can therefore only be drawn on the two included domains. Studies examining detailed health literacy profiles are warranted to identify additional health literacy challenges and opportunities to mitigate the effect of such challenges among people with cardiovascular disease.
Interpretations
The European Health Literacy Project has examined health literacy in a general population of approximately 8000 individuals across Europe. 5 The results indicate an association between health literacy and long-term illness, which has been confirmed in a study on the survey data on which our study is also based. 10 In this, cardiovascular disease has been shown to be one of the most challenging conditions in this respect.
The role of health behaviour in relation to the prognosis and quality of life in people with cardiovascular disease is well-established 29 and so is the need for improvements in secondary prevention and rehabilitation across Europe.30,31 In concordance with our results previous research in diverse populations has found associations between low health literacy and physical inactivity,5,7,32–34 unhealthy diet,7,33–35 smoking,7,35 obesity,5,7,32,36 and underweight. 37 The associations are most consistent in relation to physical activity and diet, while findings regarding smoking and weight are contradictory.5,33,34,37 Studies on the associations between health literacy and alcohol consumption report either no association, weak or even negative associations.5,32,33,37
Interestingly, we found that in the case of smoking and weight control, health literacy was only associated with very unhealthy behaviours while being insignificant in relation to more mediocre behaviours. After cardiovascular disease onset, efforts are often made by the individual and health professionals to change unhealthy behaviours, for example, through rehabilitation programmes, preventive consultations etc. Thus, people receptive to such interventions may move towards healthier lifestyles leaving a group of individuals facing additional challenges behind. Our finding may reflect the lower health literacy of this vulnerable group and this may also explain some of the inconsistent associations regarding smoking and weight in the literature.
The widely acknowledged health literacy levels – functional, interactive and critical health literacy – presented by Nutbeam 38 are emphasized differently in the HLQ subscales with ‘Understand information well enough to know what to do’ focusing on functional health literacy while ‘Ability to actively engage with healthcare providers’ accentuates interactive health literacy. To our knowledge no previous studies on individuals with cardiovascular disease have distinguished between the two levels. Strong associations with understanding health information were found in physical activity, dietary quality and weight control. Perhaps this reflects the complex knowledge needed to understand and change these behaviours. On the other hand, smoking is a less complex behaviour, but inducing change may depend more on the motivations created by social networks and interaction with healthcare providers.
Existing literature on general populations finds a positive association between health literacy and general health status5,17,35 as well as physical and mental health status.39–41 However, in accordance with our findings, studies performed on people with cardiovascular conditions15,18 suggest a far stronger association between health literacy and physical health status than mental health status. Physical function after the onset of a cardiovascular disease is highly dependent on self-care behaviours. Macabasco-O’Connell et al. 13 have shown an association between inadequate health literacy and lack of disease specific self-care behaviours in patients with heart failure, but other studies have not been able to fully reproduce this result.42–44
Generalizability
The population characteristics of this study, that is, with the ‘typical’ respondent being a man above 60 years with low educational level, are in line with that of other studies on individuals with cardiovascular disease.45,46 The population of Central Region Denmark has similar demographic, health and social composition to the Danish population in general, 47 but the generalizability of our findings to populations outside Denmark depends largely on the specific local demography and context. In this study, external validity in relation to cardiovascular patients is also limited by the lack of discrimination between all relevant diagnoses and disease severity.
Conclusion
Among individuals with cardiovascular disease, the ability to understand health information and the ability to actively engage with healthcare providers were associated with important health behaviours and health status. This places health literacy as an important determinant of successful cardiovascular disease prevention and a target in future interventions on skill development, patient–provider interaction and health service improvement.
Keeping in mind the socially unequal distribution of both health literacy competences and cardiovascular disease recovery this study provides a strong argument for health literacy interventions as a means to fight inequality in health among individuals with cardiovascular disease.
Footnotes
Author contribution
AA, KF and HTM contributed to conception and design. AA and KF contributed to acquisition of the analysis. AA, KF and HTM contributed to analysis. AA, KF, BC, GR and HTM contributed to interpretation. AA drafted the manuscript. KF, BC, GR and HTM critically revised the manuscript. AA, KF, BC, GR and HTM all gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgement
Our appreciation goes to individuals responding to the questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish Heart Foundation [grant number 15-R99-A5895-22939]; Central Region Denmark [grant number 1-15-1-72-13-09]; Karen Elise Jensen’s Foundation; and Aarhus University [grant number 18296471].