
Abstract
Background
Arterial stiffness is an important predictor of cardiovascular risk in adult life. Increased arterial stiffness can also be present in children and may be associated with several other cardiovascular risk factors. Until now, however, we know little about measuring arterial stiffness in preschool children. In this study, we assessed the feasibility of measuring arterial stiffness in preschool children and explored possible determinants related to arterial stiffness at this age.
Methods
We studied 168 healthy children, aged 3.3–4.1 years, who were recruited from a prospective birth cohort. We measured arterial stiffness, expressed in aortic pulse wave velocity and augmentation index, using a non-invasive oscillometric device (Arteriograph). We measured anthropometry and recorded other determinants using a questionnaire.
Results
In 100 children (59.5%) at least one valid arterial stiffness measurement was obtained. Of these infants, 89 had at least two valid measurements and 73 infants had at least three valid measurements. The mean aortic pulse wave velocity was 5.56 m/s (SD 0.77), and the mean augmentation index of the aorta was 19.7 m/s (SD 7.0). The augmentation index was significantly inversely associated with body height, with a regression coefficient of –0.78 (m/s)/cm (95% confidence interval –1.13 to –0.42). The augmentation index was not significantly associated with age, sex or (birth) weight.
Conclusion
The feasibility of measuring arterial stiffness in preschool children using the Arteriograph is moderate. We identified height as the most important determinant of the augmentation index in preschool children.
Introduction
Arterial stiffness is an important marker for the risk of developing cardiovascular diseases in adult life. Arterial stiffness, which describes the loss of capability of an artery to react on pressure changes due to loss of elasticity, is influenced by several parameters. In adulthood, male sex, older age, increased weight and a lower height are shown to be the most important determinants of increased arterial stiffness.1,2 In childhood, low birth weight (small for gestational age), 3 higher gestational age 3 and breastfeeding in the first year of life are associated with a higher arterial stiffness.4–8 Furthermore, several studies have demonstrated that chronic inflammation increases arterial stiffness.9–12
Arterial stiffness is expressed in several parameters, such as carotid-femoral pulse wave velocity (PWVao) and the augmentation index (AIX) of the aorta (AIXao) and the brachial artery (AIXbr). While PWVao is used as a direct marker for arterial stiffness, the AIX is used as a direct marker for wave reflection and an indirect marker for arterial stiffness.13–15 In addition, central systolic blood pressure (SBP) is an important parameter describing arterial stiffness, and shows a strong correlation with an increased arterial stiffness when increased. 15 PWVao and AIX increase with the ageing process and both markers provide information about the status of the arterial system. 14
Atherosclerosis, the leading cause of cardiovascular disease, starts to develop in early life; however, this does not directly cause symptoms in childhood.4,16–18 Increasing evidence suggests that cardiovascular risk factors are in childhood associated with increased arterial stiffness and other cardiovascular risk factors.4,5,18 These studies mainly focused on children over 5 years of age. Little is known about measurements of arterial stiffness in preschool children.
Arterial stiffness can be measured with many different devices. However, many of them are not validated in childhood and are not suitable to measure preschool children. With this study, we aim to assess the feasibility of measurements of arterial stiffness in preschool children, using the Arteriograph, a non-invasive oscillometric device. Secondly, we aim to explore possible determinants for arterial stiffness in preschool children.
Methods
Study population
We performed arterial stiffness measurements in 3-year-old healthy children, recruited from the Wheezing Illnesses Study Leidsche Rijn (WHISTLER), a population-based birth cohort study in Utrecht, the Netherlands. 19 The study design was described in detail earlier. 19 In short, healthy children born in Leidsche Rijn, Utrecht, the Netherlands, were invited to participate. Children were excluded when gestational age was under 36 weeks, when they were born with congenital abnormalities or when they suffered from respiratory diseases. From December 2011 to April 2013 participants were invited for a follow-up visit at the age of 3 years. At this visit, the investigated subjects each underwent a physical examination, a lung resistance measurement using a MicroRint device (MicroMedical; VIASYS Healthcare, Kent, UK) 20 a transthoracic echocardiography and arterial stiffness measurements. The paediatric medical ethics committee of the University Medical Centrum Utrecht, the Netherlands, approved the study. Written informed consent was obtained from the parents.
Questionnaire
We used questionnaires completed at the first neonatal visit, at approximately 4 weeks of age, to assess characteristics, including gender, age at visit, gestational age, birth weight and height, socioeconomic status based on maternal education and exposure to environmental factors, such as tobacco smoke exposure during pregnancy. Information about the duration of breastfeeding was obtained from monthly taken questionnaires in the first year of life. Prior to the visit at the age of 3 years, the parents completed a new questionnaire containing information about current risk factors, current smoke exposure and health status of both the child and the relatives.
Anthropometric measurement
During the visit, the body weight of the children was measured wearing light clothing, using a standard electronic scale. Body height was measured without shoes, using an infant stadiometer. Body mass index (BMI) was calculated according to the World Health Organization (WHO) BMI-for-age growth standards. We measured the distance between the jugulum and the upper edge of the symphysis, measuring from the sternal notch to the pubic bone, to be able to calculate the aortic PWVao.
Arterial stiffness measurement
The children were measured with the Arteriograph (Tensiomed, Budapest, Hungary), a non-invasive oscillometric device, which has been validated earlier in adults,13–15,21 but not yet in (preschool) children.15,22 Measurements were taken in a supine position after 30 minutes of rest. The Arteriograph measures several parameters of arterial stiffness, such as blood pressure, PWVao and AIX.
Measuring the arterial stiffness is based on the physiological process of pulse waves. This pulse wave is measured in the brachial artery, with a brachial cuff. 23 As the cuff is pressurised, approximately 35–40 mmHg above the SBP, the brachial artery is completely occluded, so that oscillations can be recorded and pressure peaks can be detected. There are two systolic peaks that can be distinguished. First, there is the ‘early’ systolic pulse pressure wave (P1), which is formed by the left ventricle ejecting blood into the aorta. The ‘late’ systolic peak (P2) is due to the first pressure wave travelling along the aorta, being reflected at the site of the aortic bifurcation.2,23,24 The return time of the systolic pressure wave, from the aortic root to the iliac bifurcation and back, is equal to the time lapses between the peaks of P1 and P2. PWVao can be calculated by halving this time and measuring the distance between the jugulum and the symphysis, which is comparable with the aortic length. 23 AIX can be abstracted from the measured pulse pressure, and expresses the effect of the reflected wave. 25 The Arteriograph software gives an overall value of arterial stiffness, if all consecutive pulse waves can be analysed. As pulse waves in early childhood are small and movement can distort the shape of a pulse wave, which could make evaluation of pulse waves impossible, we analysed each cardiac cycle one by one using the automatic Arteriograph software. A measurement was considered valid after a visual check and if the software was able to calculate a reliable value from the pressure wave curves. For every individual subject, we used the median of at least three valid curves.
Of randomly selected children, we also measured the blood pressure with the Dinamap oscillometric device (Dinamap 1846 SX/P; GE Healthcare, Waukesha, WI, USA). 26
Statistical analysis
The subjects’ characteristics are presented in percentages, mean (standard deviation; SD) or median. All variables were checked for normality of distribution. An intraclass correlation coefficient (ICC) was used to determine the intrameasurement variability of average AIXbr, AIXao and PWVao based on one to three or more valid curve measurements. The correlation between the blood pressure measured with the Dinamap and the pressure measured with the Arteriograph was analysed calculating Pearson’s correlation coefficient. 27 Differences in characteristics of children with and without a valid measurement were tested using independent samples t-test for continuous variables or χ2 for categorical variables. Univariable linear regression analysis was used to assess the associations of determinants based on the previous literature, with the arterial stiffness parameters as dependent variables.
Statistical analysis was performed using SPSS Inc. version 21.0 for Windows (IBM, 2012, Chicago, IL, USA). A statistical significance was considered reached at a P value of less than 0.05.
Results
Baseline characteristics (n = 168).

Data are means and standard deviations (SD) unless otherwise indicated.
BMI: body mass index.
As defined according to the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) definition. 28 Parental waist circumference was not measured.
First-degree relatives are parents, second-degree relatives are grandparents. Considered positive if coronary or peripheral artery disease was present before the age of 60 years.
Higher vocational or university education.
Blood pressure measurements with the Arteriograph succeeded in 136 subjects (81.0%). Of all children with no blood pressure measurement, 13 children refused to participate and 14 measurements could not be performed due to restlessness. We were not able to measure three children due to technical errors as a consequence of low battery, and during the visit of two children measurements were prematurely stopped due to illness of the child.
Arterial stiffness parameters.

AIXbr: augmentation index of the brachial artery; AIXao: augmentation index of the aorta; PWVao: aortic pulse wave velocity; SBPao: systolic blood pressure of the aorta; PPao: aortic pulse pressure; MAP: mean arterial pressure; ED: ejection duration; RT: return time.
Data are means and standard deviations (SD).
The mean value of SBP measured by the Dinamap device was 95 mmHg (SD 6), whereas diastolic blood pressure (DBP) measured showed a mean value of 58 mmHg (SD 6). In the same 34 children, SBP measured by the Arteriograph showed a mean value of 94 mmHg (SD 7), with a DBP mean value of 50 mmHg (SD 5). Pearson’s correlation coefficients of blood pressures measured using the Arteriograph and the Dinamap were 0.56 for SBP and 0.69 for DBP.
Differences in characteristics of children with and without a valid measurement.
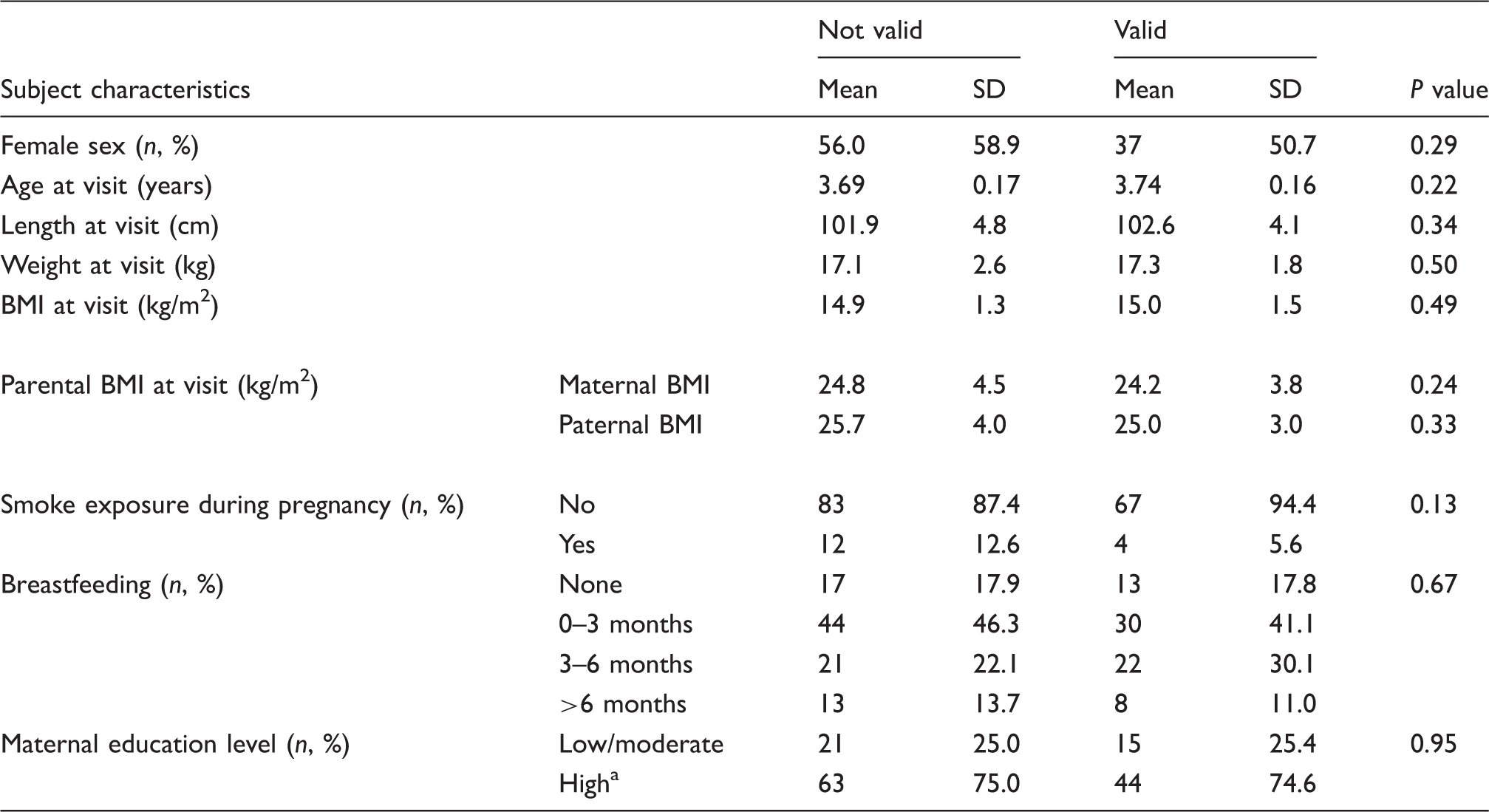
Data are means and standard deviations (SD).
BMI: body mass index.
P value <0.05 is considered significant.
Higher vocational or university education.
Association between arterial stiffness and child characteristics in early life.

AIXao: augmentation index of the aorta; PWVao: aortic pulse wave velocity; CI: confidence interval.
P value <0.05 is considered significant.
Discussion
This is the first study that has assessed the feasibility of measuring arterial stiffness using the Arteriograph in a large group of preschool children. We were able to measure arterial stiffness (with at least three valid curve waves) in almost half of our study population, which indicates that the feasibility is moderate.
Main results and strengths
In our study, height was the only determinant that was significantly associated with the AIXao. The influence of body height on arterial stiffness, in particular the AIXao, had been investigated before. This study showed that the influence of body height changes over time, probably due to a changing aorta growth rate. 29 Other studies in childhood, using different devices, also found evidence for age and weight as determinants of arterial stiffness.1,2,4 Although these two determinants were not significantly associated with the PWVao or the AIXao in our study, the trends of the regression coefficients were comparable to these previous findings. The age range of our study population was small, which might explain these differences in statistical significance. We found comparable arterial stiffness in boys and girls, while previous studies found evidence for increased arterial stiffness in boys.1,2 As previous studies were performed in older age groups, these sex differences probably develop at an older age. These differences might be influenced by hormonal puberty-related changes.4,16,30
To determine the intra-measurement variability we calculated the ICC. This showed a good correlation, with an ICC of 0.87 for PWVao and 0.72 for AIXao for three or more occlusions per child. Regarding blood pressure measurements, we calculated the correlation between the measurements by the Arteriograph and the Dinamap device, using a Pearson correlation coefficient. In our homogeneous study population with a low variability in age, weight and height, the values of these correlation coefficients can be considered strong.
We were able to determine the feasibility of the Arteriograph device in a relatively large group of healthy 3-year-old children, which we consider moderate. In addition, we were able to investigate the characteristics of arterial stiffness measurement in this age group. One previous study determined reference values in the preschool age group, but they only studied a small group of preschool children (n = 44). 2 This previous study only stratified for sex and age and did not study the associations between child characteristics and arterial stiffness. The measured PWVao and AIXao in our 3-year-olds are in accordance with the results of the previously performed study. 2
In preschool children many devices are not suitable to measure arterial stiffness. The feasibility of measuring arterial stiffness using the Arteriograph had not previously been assessed in this group. Measurement of arterial stiffness using the Arteriograph was relatively quick (a few minutes), and children experienced only a little discomfort, comparable with the amount of discomfort experienced during a blood pressure measurement. However, we must note that recent studies have demonstrated the feasibility of measuring arterial stiffness with different devices, although this mainly applies to older subjects.31–34
Limitations
Our study has several limitations. First, we measured the arterial stiffness in children during a study visit after other measurements: the children first underwent a physical examination (length and weight), a lung function measurement and a transthoracic echocardiography. However, performing multiple consecutive tests reflects current practice. Also, children were allowed to rest for at least 10 minutes before the measurements were taken, according to the Arteriograph’s manual.
A second limitation is that there is a reasonable chance of dropout of the children because the children were tired or restless, even though these measurements are all completely non-invasive. In our study, we were able to obtain one valid measurement in a relatively high percentage of subjects, while we were able to obtain at least three valid measurements per child in only almost half of the study group. The number of valid measurements will probably increase in a study without performing other tests.
Future directions
Although the Arteriograph has been validated in adults and adolescents before, the Arteriograph should be further validated in young children. 15 Given the fact that atherosclerosis starts early and increasing evidence suggests that early life adverse exposures could lead to structural changes in the vascular system, it is of the utmost importance to gain more knowledge about the vascular system in early childhood. In our study, we only measured the arterial stiffness at the 3-year visit. We recommend measuring arterial stiffness during follow-up later in life, in order to track possible alterations in risk factors and arterial stiffness parameters.
In conclusion, in our study, we were able to determine the feasibility of measuring arterial stiffness in preschool children using the Arteriograph, which is considered moderate. We consider height as the most important determinant of the AIX.
Footnotes
Author contribution
All authors contributed to the conception and design of the work and to the analysis and interpretation of data. MMV and JBE contributed to acquisition of data. MMV drafted the manuscript. CSPMU, CKvdE and JBE critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
The authors gratefully acknowledge all parents and children who participated, and Eltje Bloemen for her contribution of analysing the pulse waves and Myriam Olling-de Kok for secretarial support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Wheezing Illnesses STudy LEidsche Rijn received grant 2100.0095 from The Netherlands Organisation for Health Research and Development (ZonMw). An unrestricted grant was received from Glaxo Smith Kline.