
Abstract
Background
In contemporary atrial fibrillation trials most deaths are cardiac related, whereas stroke and bleeding represent only a small subset of deaths. We aimed to evaluate the long-term risk of cardiac events and all-cause mortality in individuals with atrial fibrillation compared to no atrial fibrillation.
Design
A systematic review and meta-analysis of studies published between 1 January 2006 and 21 October 2016.
Methods
Four databases were searched. Studies had follow-up of at least 500 stable patients for either cardiac endpoints or all-cause mortality for 12 months or longer. Publication bias was evaluated and random effects models were used to synthesise the results. Heterogeneity between studies was examined by subgroup and meta-regression analyses.
Results
A total of 15 cohort studies was included. Analyses indicated that atrial fibrillation was associated with an increased risk of myocardial infarction (relative risk (RR) 1.54, 95% confidence interval (CI) 1.26–1.85), all-cause mortality (RR 1.95, 95% CI 1.50–2.54) and heart failure (RR 4.62, 95% CI 3.13–6.83). Coronary heart disease at baseline was associated with a reduced risk of myocardial infarction and explained 57% of the heterogeneity. A prospective cohort design accounted for 25% of all-cause mortality heterogeneity. Due to there being fewer than 10 studies, sources of heterogeneity were inconclusive for heart failure.
Conclusions
Atrial fibrillation seems to be associated with an increased risk of subsequent myocardial infarction in patients without coronary heart disease and an increased risk of, all-cause mortality and heart failure in patients with and without coronary heart disease.
Introduction
Current treatment of thromboembolic complications associated with atrial fibrillation (AF) has mainly focused on the prevention of stroke.1,2 Notwithstanding, patients with AF frequently develop coronary heart disease (CHD). Similar cardiovascular risk factors for CHD and AF have been suggested to reflect a common pathway of underlying vascular disease. 3
In a recent meta-analysis of patients with AF, cardiac deaths accounted for 46% of all deaths during follow-up, whereas non-haemorrhagic stroke/systemic embolism and haemorrhage-related deaths represented only 5.7% and 5.6% of the total mortality, respectively. 4 As part of the Atherosclerosis Risk in Communities (ARIC) study, 5 including participants free of CHD at baseline, AF was associated with a 63% increased risk of incident myocardial infarction (MI). These studies limited inclusion to either AF-only or CHD-free patients.
The objective of the present systematic review was therefore to summarise the evidence from contemporary epidemiological studies, which included patients with predominantly sinus rhythm with or without CHD at baseline, examining the association between AF and the risk of major cardiac events (CEs) and mortality, followed by an evaluation of the influence of core patient-level characteristics such as age, gender and CHD at baseline.
Methods
The review protocol has been registered at http://www.crd.york.ac.uk/PROSPERO/ (reg. CRD42016033209). The manuscript was prepared according to the 2009 PRISMA checklist. 6
Eligibility criteria
We selected randomised trials or observational studies of clinically stable patients that evaluated MI, heart failure (HF) and mortality as endpoints in AF patients versus patients without AF; both categories with or without preceding CHD.
To reflect contemporary management in view of the large differences in risk and outcome as compared to earlier management strategies 7 we considered articles published between 1 January 2006 and 21 October 2016.
In order to minimise the problems associated with small-scale studies, at least 500 participants who were haemodynamically stable on inclusion and followed for 12 months or longer were required. As the unfavourable prognosis of AF complicating an acute MI 8 and cardiac surgery 9 is well established, studies selected had to have included patients who had sustained an MI or coronary artery bypass graft operation (CABG) more than 30 days prior to inclusion. Studies recruiting patients with acute AF at baseline were excluded, as were outcome studies comparing the prognostic impact of rate versus rhythm control in AF patients.
Literature search
We searched the databases Embase, Medline, Cochrane Library and Pubmed (including articles published ahead of print). Our search strategy combined text words and subject headings, with details presented in Supplementary Appendix 1.
Study selection
Two investigators independently evaluated studies for eligibility. Discrepancies were solved by repeated review and discussion. Reference lists were scrutinised to detect studies overlooked by the search.
Data abstraction
Data were extracted according to an a priori protocol registering the mean age of the cohort, frequency of men, CHD status at baseline, study design, median follow-up period and main results from multivariate analysis.
The study quality was assessed by evaluating design characteristics using the Newcastle–Ottawa scale (NOS) for cohort studies. 10 The checklist includes core domains to assess: (a) methods for selecting study participant; (b) appropriate control for confounding (comparability); and (c) methods assessing outcome variables.
Assessment of exposure and outcome
The diagnosis of AF should have been based upon electrocardiographic criteria and supported by hospital discharge letters and other available medical records. Objective criteria for CHD were: a confirmed hospitalisation for MI, percutaneous coronary intervention (PCI) or CABG, a clinical diagnosis of angina pectoris verified by a positive stress test, or significant coronary artery stenosis on a coronary angiogram.
Outcomes should have been verified from hospital records. Endpoint MI was defined as pure MI according to current standards, although the composite endpoints CEs (MI, angina pectoris, PCI or CABG), major CEs (coronary death and non-fatal MI) and cardiovascular events (composite of CEs (MI, acute and subacute ischaemic heart disease, CABG or PCI), cerebrovascular events (occlusion/stenosis of the precerebral/cerebral arteries or subarachnoid haemorrhage) and peripheral events (vascular interventions)) were accepted for the studies by Ruigomez et al., 11 Marte et al. 12 and Vermond et al., 13 respectively.
Statistical analysis
To calculate an overall relative risk (RR) we used the effect estimates and its 95% confidence interval (CI) given from multivariable analysis, and a standard random effects meta-analysis. 14
The magnitude of between-study heterogeneity was evaluated by the I2 statistics. I2 values of 25%, 50% and 75% indicate low, moderate and high heterogeneity. 15 To investigate possible sources of heterogeneity, we performed analyses stratified by the patient characteristic CHD at baseline, and the study characteristic prospective versus retrospective timing of the study. Univariable random effects meta-regression analyses were used to examine whether effect estimates were affected by these covariates as well as by the patient covariates mean age of the cohort and frequency of men. The proportion of heterogeneity explained by the covariates was calculated by comparing the estimated between-study variance, τ2, with its value when no covariates were fitted. For power consideration we needed a minimum of 10 studies per covariate in a single model of meta-regression. 16 Sensitivity analyses were conducted by omitting one study in turn from the meta-analysis and assessing its effect on the overall results. 17 Publication bias was assessed using Egger’s test, which can be used only when at least 10 studies are included in the meta-analysis. 18
The analyses were performed using STATA 13.0 (StataCorp LP, College Station, TX, USA).
Results
Study selection
Our search identified 7927 references. Excluding duplicate publications and irrelevant content, 15 publications (18 studies) met our inclusion criteria.5,11–13,19–29 The flow of information is presented in Supplementary Appendix 2. Goto et al. 26 reported results from a CHD population (Goto_RCHD) and a risk factor-only population (Goto_RRFO). Otterstad et al. 27 reported results for patients with prevalent AF (Otterstad_APAF) and incident AF (Otterstad_AIAF). Andersson et al. 29 presented results separately for men and women.
Characteristics of the studies included in the meta-analysis
Characteristics of the 15 publications (18 studies) included in the meta-analysis.
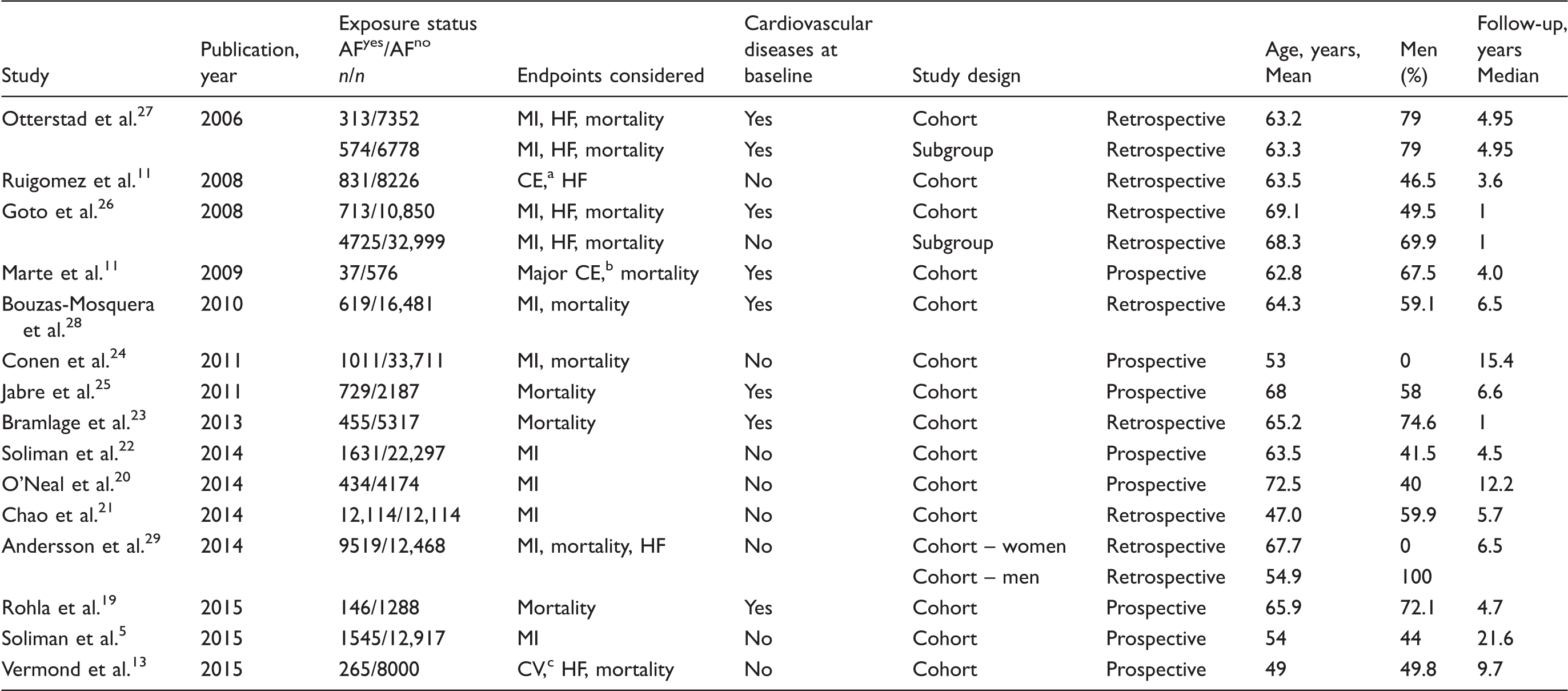
AF: atrial fibrillation; MI: myocardial infarction; HF: heart failure; CEs: cardiac events; CV: cardiovascular event.
CE defined as myocardial infarction, angina pectoris, percutaneous coronary intervention or coronary artery bypass grafting.
Major CE defined as coronary death and nonfatal myocardial infarction.
CV defined as cardiac events (acute myocardial infarction, acute and subacute ischaemic heart disease, coronary artery bypass grafting or percutaneous transluminal coronary angioplasty), cerebrovascular events (occlusion or stenosis of the precerebral or cerebral arteries or subarachnoid haemorrhage) and peripheral events (other vascular interventions such as percutaneous transluminal angioplasty or bypass grafting of the aorta and peripheral vessels).
All studies were cohort designs, eight with prospective timing. Confounding by age, gender, baseline cardiovascular disease and cardiac risk factors was adjusted for in multivariate analysis (Supplementary Appendix 4). In general, the studies were judged as being of a good quality (Supplementary Appendix 5).
Inclusion criteria and results in the 15 studies included in the meta-analysis.
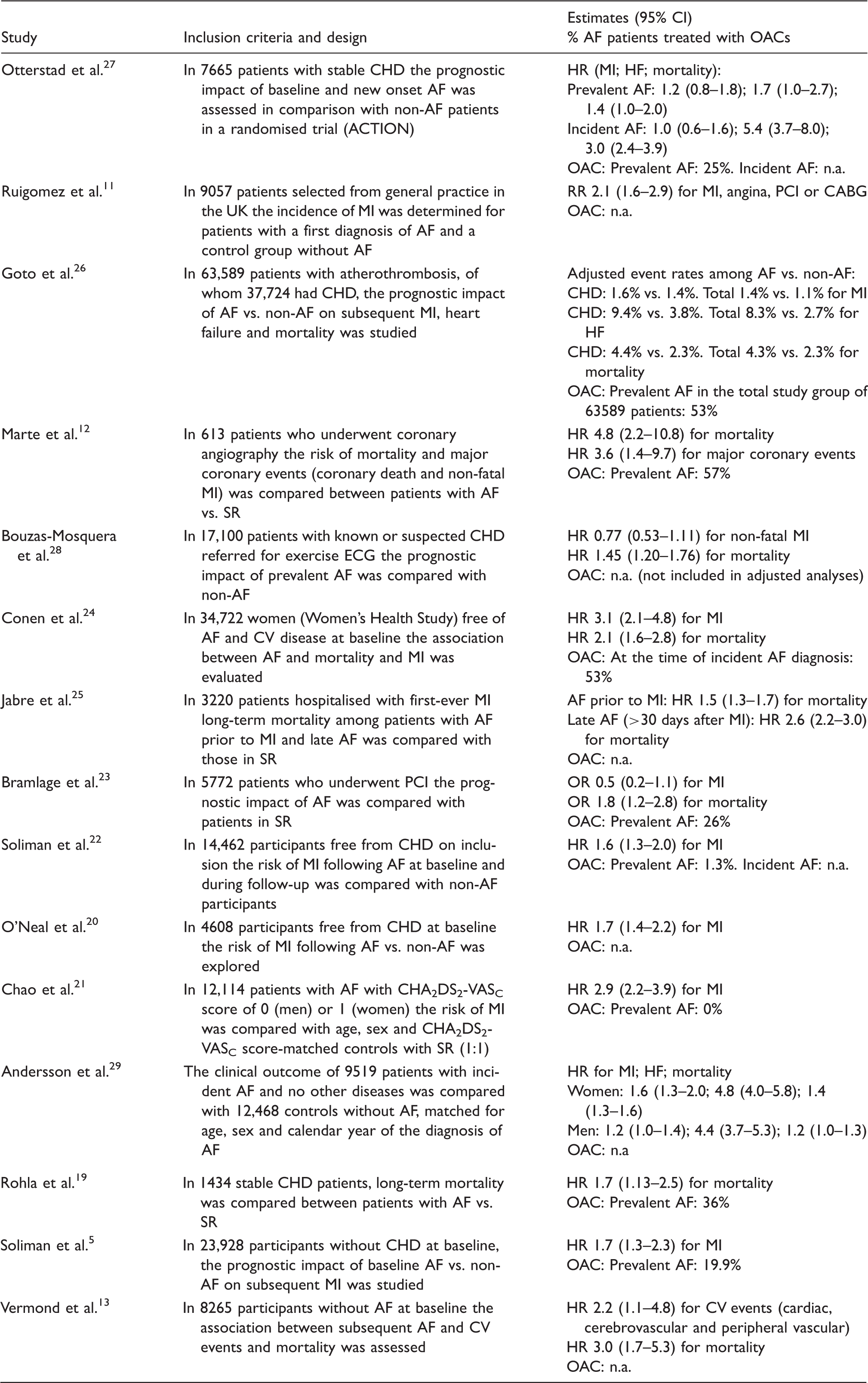
CI: confidence interval; OAC: oral anticoagulation; AF: atrial fibrillation; CHD: coronary heart disease; HR: hazard ratio; MI: myocardial infarction; HF: heart failure; n.a.: not available; UK: United Kingdom; RR: relative risk; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; SR: sinus rhythm; ECG: electrocardiogram; CV: cardiovascular; OR: odds ratio.
Endpoint MI
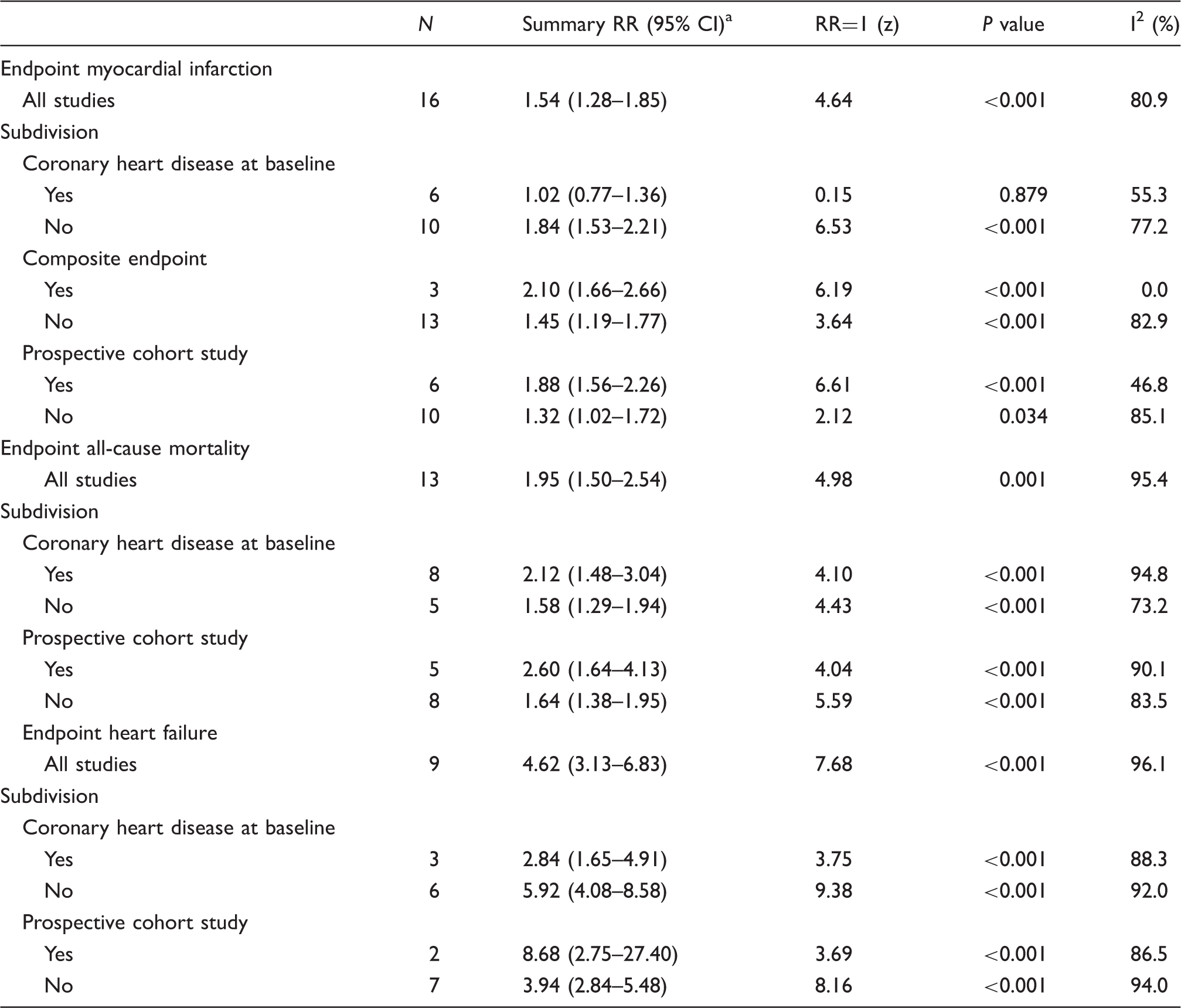
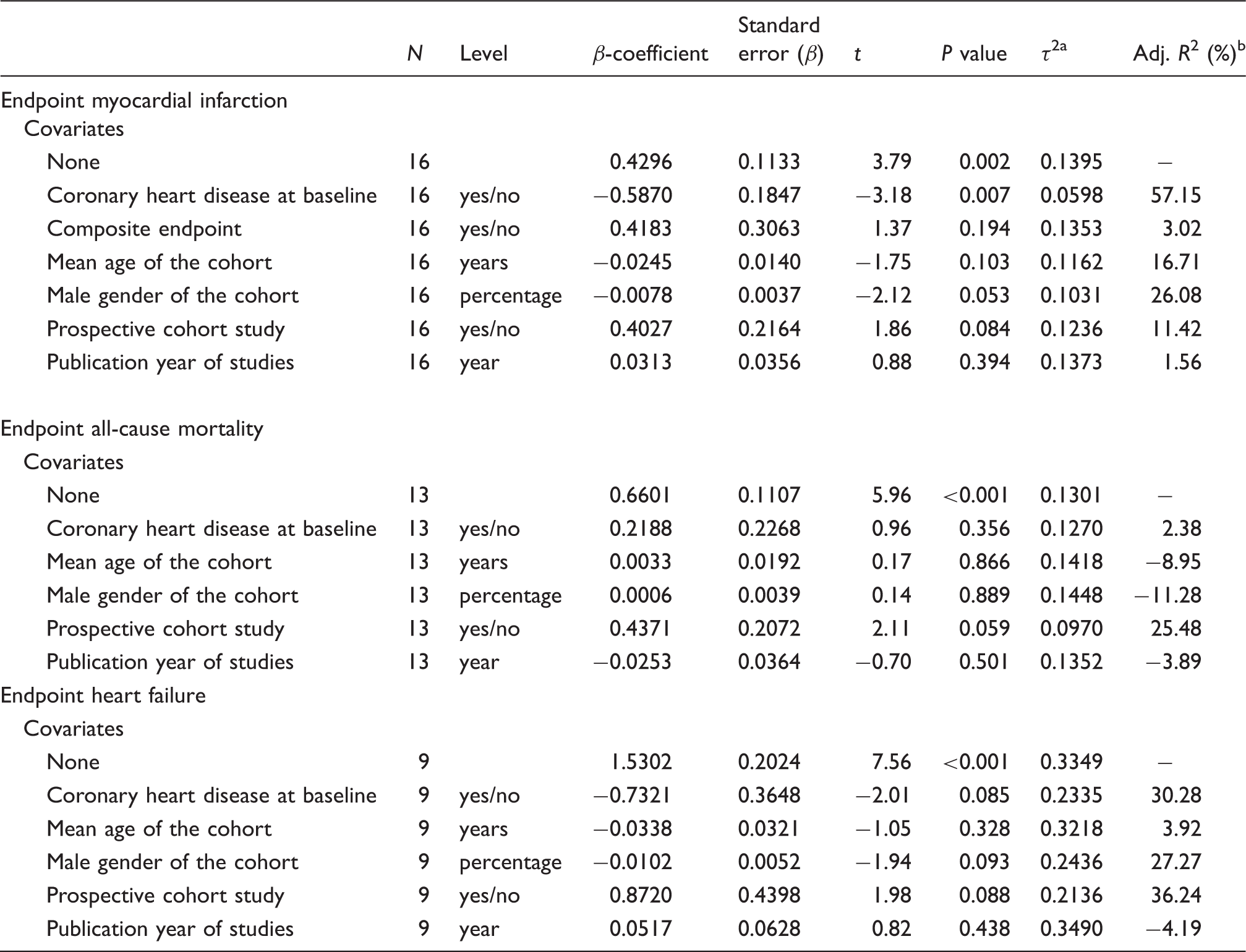
The pooled estimate including 16 studies (Figure 1(a)) showed an increased risk of MI in subjects with AF as compared to no AF (RR 1.54, 95% CI 1.28–1.85, I2 = 80.9%). CHD at baseline and the frequency of men were associated with a reduced risk of MI and explained 57% and 26% of heterogeneity, respectively (Tables 3 and 4). Furthermore, the timing of the study was borderline significant and explained 11% of heterogeneity. The effect of these three covariates was not investigated simultaneously in meta-regression both due to the correlation between CHD and gender (R = 0.5325) and few studies. In sensitivity analyses the results appeared to be robust to the influence of individual studies (Supplementary Appendix 7(a)). Publication bias was not indicated (Egger test, P = 0.967).
Forest plots for the risk of: (a) myocardial infarction; (b) all-cause mortality; and (c) heart failure associated with atrial fibrillation. ES (95% CI): risk ratio (95% confidence interval). Subgroup analysis performed with patient and study-level characteristics considered as potential sources of heterogeneity. RR (95% CI): relative risk with its 95% confidence interval. Estimates from random effects model. Results from the random effects meta-regression model considering the different patient and study-level variables. τ2, between-study variance. Proportion of between-study variance (heterogeneity) explained by the covariate.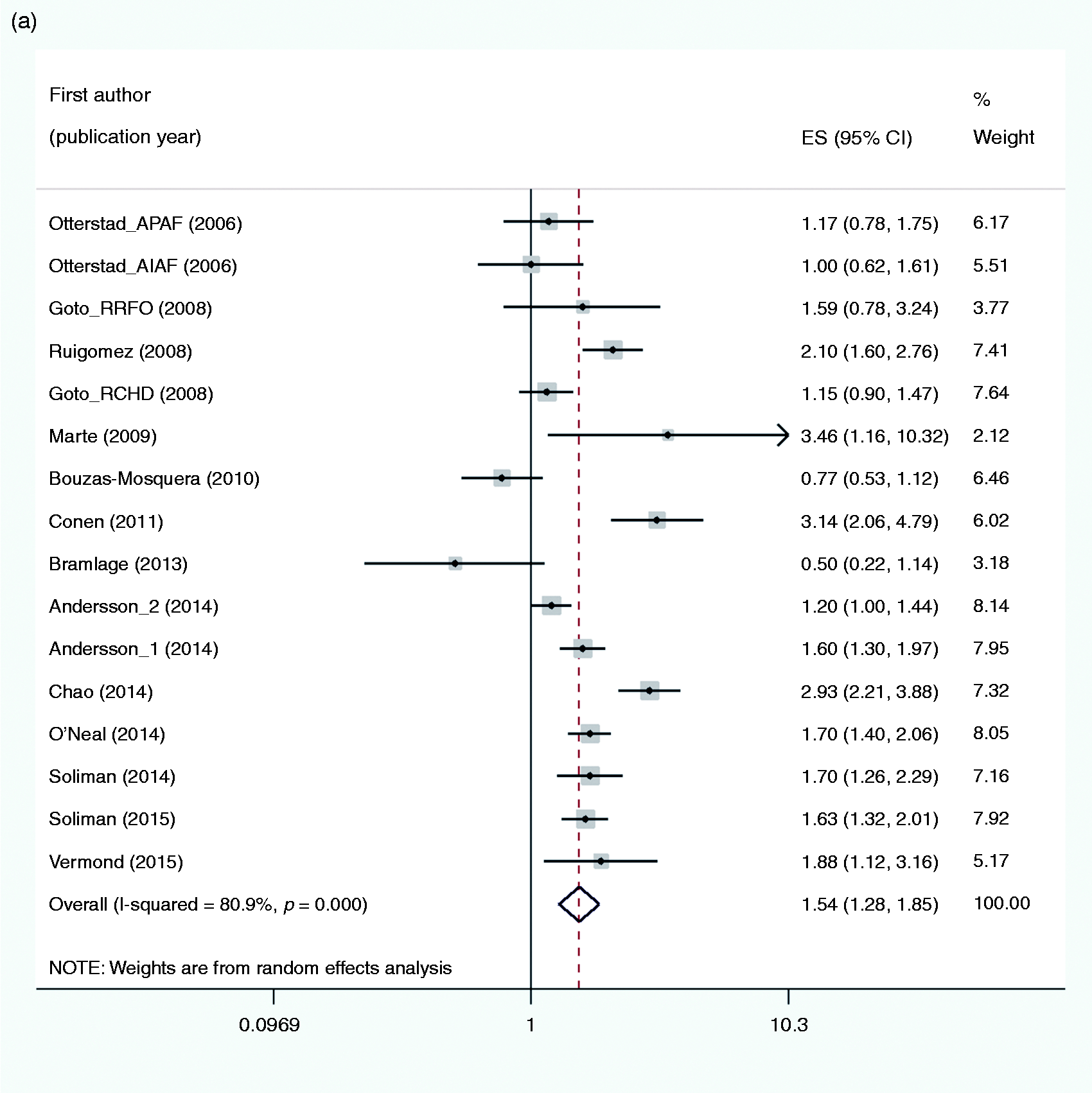
Endpoint all-cause mortality
The pooled estimate of 13 studies (Figure 1(b)) showed an increased risk of all-cause mortality in subjects with AF as compared to no AF (RR 1.95, 95% CI 1.50–2.54, I2 = 95.4%). Only the study characteristic timing was borderline significant associated with the outcome and explained 25% of heterogeneity (Table 4). In sensitivity analyses the results appeared to be robust (Supplementary Appendix 7(b)). Publication bias was not indicated (Eggers test, P = 0.619).
Endpoint HF
The pooled estimate of nine studies (Figure 1(c)) showed an increased risk of HF in subjects with AF as compared to no AF (RR 4.62, 95% CI 3.13–6.83, I2 = 96.1%). The presence of CHD at baseline, the frequency of men and timing of the study explained 30%, 27% and 36% of heterogeneity, respectively (Table 4). The borderline significance might be due to power deficiency because of the scarce number of studies. In sensitivity analyses the results appeared robust (Supplementary Appendix 7(c)). Publication bias was not examined given the number of studies.
Discussion
Prevalent and incident AF appear to be significantly associated with MI, HF and all-cause mortality. Meta-regression analyses indicated that heterogeneity could be explained by patient and study characteristics related to the presence or absence of CHD, gender and study design being retrospective or prospective.
For the endpoint MI, heterogeneity was first of all explained by pre-existing CHD; AF patients without pre-existent CHD demonstrated a significantly higher risk of MI when compared to non-AF patients as opposed to stable CHD patients.
We judged all included studies to be of satisfactory methodological quality. A retrospective design was a major limitation and differences in data quality might explain the tendency towards a higher risk of all endpoints related to a prospective design, as seen in Table 3. This review is based on a comprehensive literature search designed to avoid a large heterogeneity related to comorbidities and acute stage scenarios of CHD manifestations and interventions, and the meta-analysis is based on comprehensively study-level adjusted estimates. However, the probability of unmeasured confounding cannot be excluded in observational studies.
In a very recent meta-analysis of cohort studies, Odutayo et al. 30 reported an increased risk for a range of different outcomes when exposed to AF, with a high level of heterogeneity. In contrast to our study, not only stable individuals with or without CHD were included, but also a variety of study populations, such as post-acute MI and post-cardiac surgery. The present meta-analysis differs substantially, as we have narrowed the spectra of patient inclusions and performed a literature search which includes text words and subject headings. Odutayo et al. did not provide detailed information on OACs given to patients with versus without CHD, but sensitivity analysis revealed lower all-cause mortality in studies with a higher proportion of participants receiving OACs.
In a recent meta-analysis of 12 studies, Guo et al. 31 reported the same increased risk of MI in AF patients as in the present study. The risk of HF and death was not studied. Interestingly, and in line with the present study, AF was associated with a significantly increased risk of MI in patients free from CHD at baseline. Stroke prevention is a major public health priority 32 and it is of interest that a greater proportion of CHD patients were treated with an OAC than CHD-free patients, which might be explanatory for their reduced risk of MI as seen in both the study of Guo et al. and in the present analysis.
Supporting the trend towards a higher female risk of MI among AF patients in our study. Emdin et al. 33 reported an association with a higher risk of fatal and non-fatal cardiovascular events in women.
This systematic review/meta-analysis demonstrates a relationship between AF and an increased risk of CEs and mortality, but causal evidence cannot be established. In a recent study, the presence of AF has been shown to be independently associated with a heightened risk of MI despite a lower baseline burden and progression rate of coronary atheroma. 34 Similar cardiovascular risk factors of AF and MI may reflect a common pathway of underlying disease and act as confounders such that AF may not be regarded as a causal risk factor for MI, HF and death, but a surrogate of more severe disease. In view of this, Wijesurendra et al. 35 performed magnetic resonance imaging before and after catheter ablation for AF, and stated that AF may be the consequence (rather than the cause) of an occult cardiomyopathy which persists despite a significant reduction in AF burden after ablation.
Conclusions
AF seems to be associated with an increased risk of subsequent MI in patients without CHD and with an increased risk of all-cause mortality and HF whatever the coronary status. However, AF should not be regarded as a causal risk factor for these conditions.
Footnotes
Author contribution
VR, IS and JEO contributed to the conception and design of the work and drafted the manuscript. JM and TE contributed to the design. JS contributed to acquisition, JM and TE contributed to interpretation and VR, IS and JEO to both. All authors critically revised the manuscript, gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
The authors would like to thank Matthew McGee, Morbid Obesity Center, Vestfold Hospital Trust, for proofreading the manuscript. Funding source: Vestfold Hospital Trust and University of Oslo, Norway.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.