
Abstract
Background
Cognitive ability (CA) is positively related to later health, health literacy, health behaviours and longevity. Accordingly, a lower CA is expected to be associated with poorer adherence to medication. We investigated the long-term role of CA in adherence to prescribed statins in male patients after a first myocardial infarction (MI).
Methods
CA was estimated at 18–20 years of age from Military Conscript Register data for first MI male patients (≤60 years) and was related to the one- and two-year post-MI statin adherence on average 30 years later. Background and clinical data were retrieved through register linkage with the unselected national quality register SWEDEHEART for acute coronary events (Register of Information and Knowledge about Swedish Heart Intensive Care Admissions) and secondary prevention (Secondary Prevention after Heart Intensive Care Admission). Previous and present statin prescription data were obtained from the Prescribed Drug Register and adherence was calculated as ≥80% of prescribed dispensations assuming standard dosage. Logistic regression was used to estimate crude and adjusted associations. The primary analyses used 2613 complete cases and imputing incomplete cases rendered a sample of 4061 cases for use in secondary (replicated) analyses.
Results
One standard deviation increase in CA was positively associated with both one-year (OR 1.15 (CI 1.01–1.31), P < 0.05) and two-year (OR 1.14 (CI 1.02–1.27), P < 0.05) adherence to prescribed statins. Only smoking attenuated the CA–adherence association after adjustment for a range of > 20 covariates. Imputed and complete case analyses yielded very similar results.
Conclusions
CA estimated on average 30 years earlier in young adulthood is a risk indicator for statin adherence in first MI male patients aged ≤60 years. Future research should include older and female patients and more socioeconomic variables.
Keywords
Introduction
Myocardial infarction (MI) is the most common acute cardiac event, annually affecting around seven million people globally. MI is a consequence of underlying coronary heart disease, the leading cause of death worldwide.1,2 Acute MI care has improved considerably and mortality has decreased by about 50% over the last 15–20 years. 3 Hence a clear majority of patients now survive their first MI, which has, in turn, increased the need to improve secondary prevention. 4 In Sweden, only 21% of all patients reached their four most important rehabilitation goals (Q4). 5 The low percentage of Q4 achievers suggests that the standard information-giving approach and other secondary preventive efforts might benefit from individual tailoring.
The Q4 goals involve smoking cessation, participation in a physical activity programme, reduced blood pressure <140/90 mmHg and lowering low-density lipoprotein cholesterol to either <1.8 mmol/L or a 50% reduction. Patient behaviour is crucial in achieving these goals, of which adherence to lipid-lowering statins plays a pivotal part. 5 Elevated blood lipids is one of the most important risk factors for MI, with a population attributable risk of 50% worldwide. 6 Appropriate statin treatment and adherence is effective in reducing blood lipids, leading to reduced post-MI mortality of up to 25%. 7 Almost all first MI patients are prescribed statins, yet only around 70–80% are adherent when defined as a dispensed out-take of 80% of the prescribed annual dose. 8 Non-adherence to cardiovascular medication is a multifactorial problem, influenced by symptom and disease severity, side-effects, health literacy, socioeconomic factors and personality. 9 There is still insufficient knowledge regarding what influences statin adherence – knowledge that, if gained, could improve tailored interventions aimed at improving statin adherence.
Over a century of research has shown that general cognitive ability (CA) is crucial in human behaviour.10–12 Evident in day-to-day information processing, memory and planning,11,13 CA is highly stable within an individual 14 yet varies considerably between individuals. 11 Specifically, Deary et al. 15 found that CA was positively associated with adherence to medication. This adds to a growing body of research into cardiovascular risk factors and outcomes showing that a higher CA renders a person more likely to be physically active, 16 eat healthier food, 16 possess a higher health literacy, 17 be a non-smoker, 18 not have hypertension, 19 not develop coronary heart disease 20 and to live longer. 21 It is, however, unknown whether CA in cardiovascular patients is associated with statin adherence.
We hypothesized that the CA estimated when patients were 18–20 years old would be positively associated with one-year statin adherence during secondary prevention after suffering their first MI “on average” 30 years later, and a similar association for two-year adherence. We also examined how robust these associations were when adjusting for a range of covariates.
Methods
Data sources
The Mandatory Conscript Register contains data from Swedish men who performed standardised military psychometric testing at age 18–20 years. 22 We obtained these data from 1969 to 1997 for men registered in the national quality Register of Information and Knowledge about Swedish Heart Intensive Care Admissions (RIKS-HIA). RIKS-HIA contains data on >100 historical, acute care and discharge variables from patients admitted to any cardiac care unit in Sweden for symptoms of acute coronary syndrome. RIKS-HIA has excellent coverage of the Swedish MI population (about 90% of all patients ages <80 years with MI). Patients become eligible after the local hospital cardiologist has decided a discharge diagnosis according to ICD codes 23 I21–I23 based on electrocardiogram results, clinical symptoms and other information. 3
The national quality registry for Secondary Prevention after Heart Intensive Care Admission (SEPHIA) seeks to register all surviving patients with MI (≤75 years old) in Sweden. SEPHIA collects information on >40 variables, including behavioural interventions, treatment goal fulfilment, cardiovascular disease status and psychological status. The SEPHIA national coverage is very good (>80%). In 2014, SEPHIA included eligible patients from 97% of all Swedish hospitals. 5 SEPHIA has two follow-up visits, SEPHIA 1 (6–10 weeks after the MI) and SEPHIA 2 (12–14 months after the MI), of which we used SEPHIA 1. The Swedish National Board of Health and Welfare maintains the Prescribed Drug Register, which contains data on all prescribed medication out-takes from pharmacies.
The registers were linked and anonymized by the Swedish National Board of Health and Welfare. The study was approved by the regional ethics committee in Uppsala, Sweden (Dnr 2013/478).
Sample selection
The MI data extraction was from 1 January 2006 to 31 December 2013. We selected all first MI male patients prescribed statins for the first time at hospital discharge and still alive to be registered in SEPHIA 1 up until 31 December 2011, which provided adequate time for statin adherence follow-up. The oldest patients who possibly also had digitized and available conscription data were born in 1949, conscripted in 1969 at the age of 20 years and had a first MI in 2011 at the age of 62 years. Implementation delays in the conscript procedure and very few 20-year-old conscripts rendered a sample that was aged 60 years or younger. Our primary sample therefore consisted of 2613 relatively young first MI complete cases. Imputing incomplete cases rendered a sample of 4061 cases used in secondary (replicated) analyses (Figure 1).
Flowchart of patient inclusion and exclusion with counts in parentheses.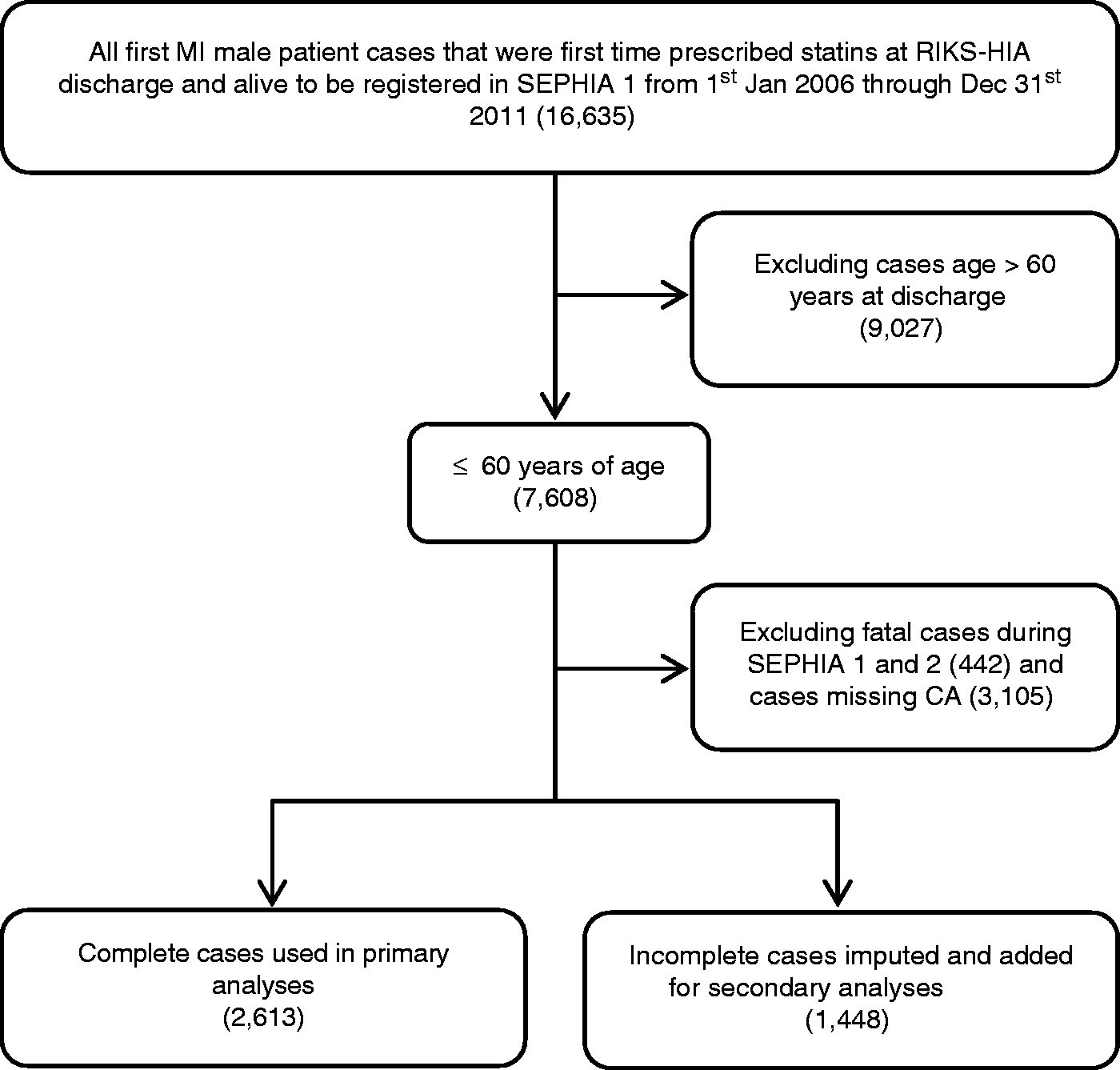
Statin adherence
We selected statin prescriptions from all patients for the two years following their MI and assumed a standard dosage of one pill per day, which reflects about 98% of all prescriptions in Sweden.
8
Patients with automatic medication administration were removed to avoid artificial adherence. Each patient’s medication possession ratio (MPR) percentage for the one-year and two-year adherence periods was calculated as:

Two observation periods were used in this study: one and two years after the SEPHIA 1 measurement. As the SEPHIA 1 follow-up occurred between 6 and 10 weeks after the MI, there was a period of time prior to our observation period when patients could pick up medication. Swedish reimbursement practices allow for up to three months’ supply to be picked up at one time. Therefore it is possible that patients could have leftover pills when going into our observation periods. To account for this, we calculated the number of pills dispensed between the MI and SEPHIA 1 and subtracted from this the number of days in that time period. Any leftover pills were added to the total for the observation period. No pills were added if patients did not adhere to treatment. To be adherent, a person had to have an MPR of at least 80%, the cut-off most commonly used in previously published work. 7
Cognitive ability
Data from the four psychometric tests in the Swedish Enlistment Battery were obtained as Stanine scores from the Mandatory Conscript Register. These tests estimate verbal ability, logical reasoning, spatial/non-verbal ability and technical understanding. 24 The most general index of CA is general intelligence (g), defined as the common inter-individual variance across several tests of specific cognitive abilities. 11 This was computed as the first unrotated factor in a principal components analysis. This factor exhibited substantial and similar loadings across the four subtests (loadings range −0.54 to −0.47) and explained 64.6% of the variance in test scores with an eigenvalue >1 (1.61). This satisfied all assumptions of g and the mean across the four subtest scores was used in the following analyses, in line with previous research. 14
Additional variables
As non-adherence may have multiple causes, 9 we sought to liberally include covariates. Some covariates are known to influence adherence, but not young adulthood CA (e.g. previous stroke) and were adjusted for in the model. Other covariates had previously been shown to be partial proxies of CA (e.g. smoking 18 ) and were adjusted for, expecting that this would reduce the CA–statin adherence association. The following covariates from RIKS-HIA were used: age, smoking, diabetes, hypertension, body mass index (BMI), previous stroke, employment status (employed/retired/other), systolic blood pressure (SBP), heart rate (HR) and discharge β blockers, A2 blockers, angiotensin-converting enzyme (ACE) inhibitors and diabetes medication. From SEPHIA 1, we used: self-reported exercise, physical activity programme participation, self-reported mobility, self-care, usual activity, pain/discomfort and anxiety/depression symptoms via the European Quality of Life Five Dimensions Questionnaire (EQ-5D). 25
Statistical analyses
Continuous variables are described as mean ± SD values and categorical variables as n (%). Statistical significance was set to 5% (two-tailed). Binomial and multinomial logistic regression was used to estimate associations. We report odds ratios (ORs) with 95% confidence intervals (CIs). Units of CA were rescaled to represent 1 SD per unit. Our modelling procedure was additive, beginning with a crude CA–adherence model and adding groups of covariates in the order: background cardiovascular risk factors (age, age 2 , weight, comorbid conditions and employment status); discharge medications; and health-related behaviours (smoking, participation in secondary prevention programmes and self-rated EQ-5D pain/discomfort, usual activities and anxiety/depression). As our primary hypothesis was that young adulthood CA would function as a long-term risk indicator for future non-adherence, the crude estimate was the main result.
The proportion of incomplete cases (36.7%) motivated a secondary sensitivity analyses through repeating the regression modelling after multivariate imputation via fully specified chained equations and predictive mean matching. 26 All variables except CA were imputed and the number of imputations set to five. Variables with the most missing values were two-year adherence (21.3% of total cases), obesity (10.1%), weight (3.7%), employment status (2.9%) and smoking (1.7%). Primary and secondary analyses rendered very similar results and the latter are reported in the Supplementary material (available online). Analyses were performed by JW in R. 27
Results
Patient characteristics
Patient characteristics as registered in SWEDEHEART/RIKS-HIA during the first hospital admission for myocardial infarction for all complete cases and by one-year and two-year statin adherence.
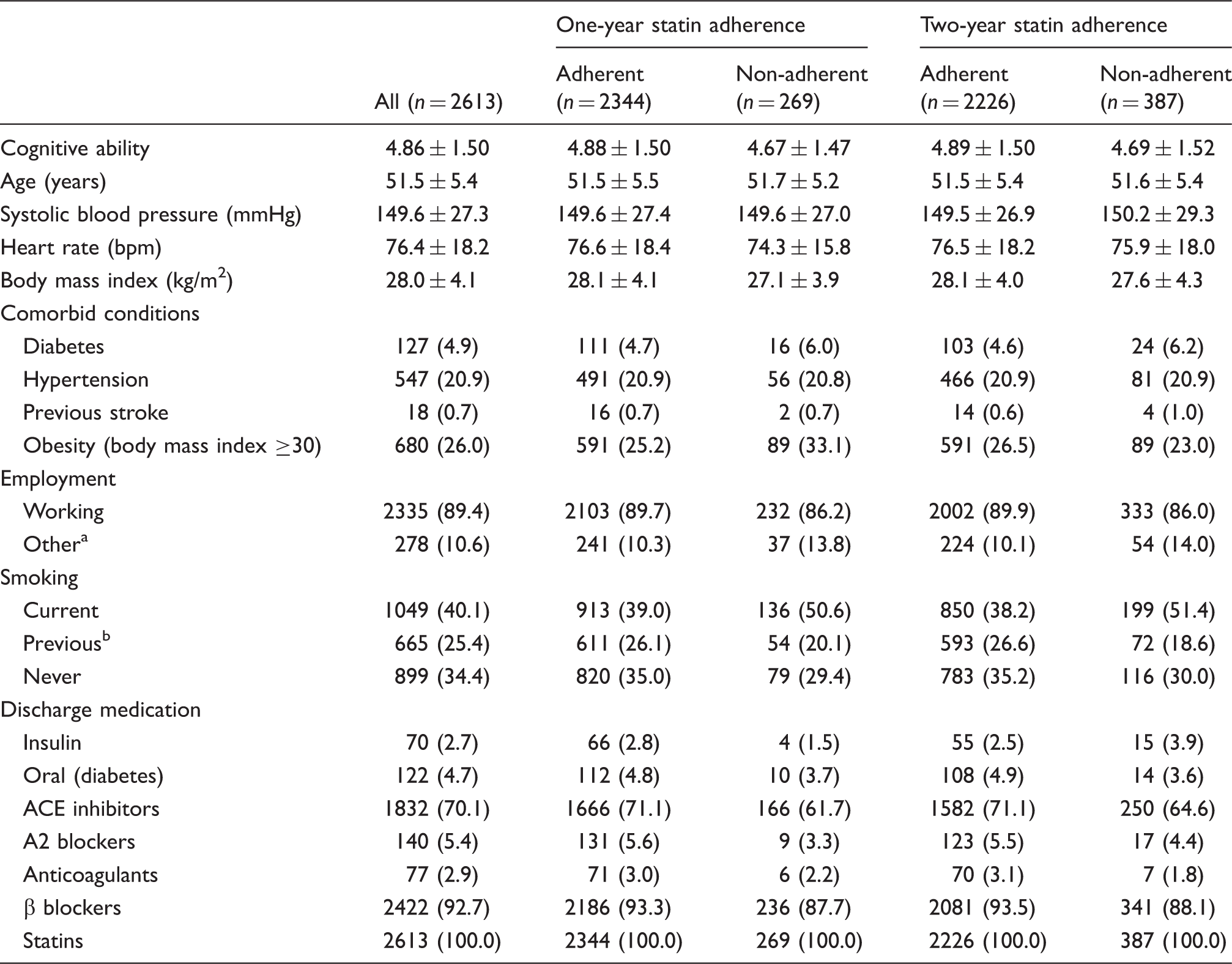
Data presented as mean ± SD values or n (%).
Includes sick leave, unemployment and premature retirement.
Reportedly quit smoking >1 month before myocardial infarction.
Secondary prevention characteristics as registered in SWEDEHEART/SEPHIA 6–10 weeks after the first hospital admission for myocardial infarction for all complete cases and by one-year and two-year statin adherence.
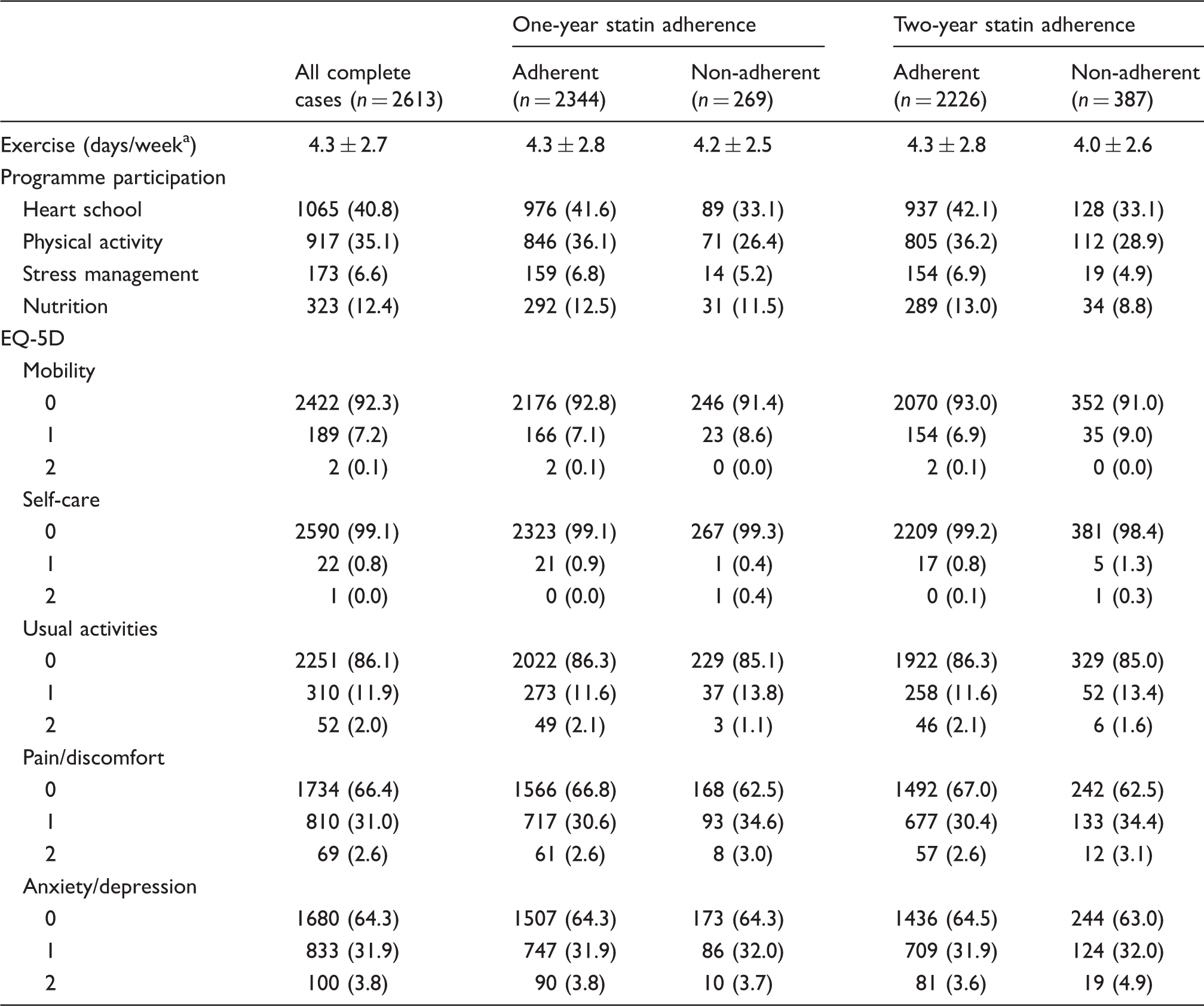
EQ-5D: European Quality of Life Five Dimensions Questionnaire.
Data presented as mean ± SD values or n (%).
Number of days with ≥30 minutes of moderately intense exercise during the previous week.
Main (crude) and exploratory (adjusted) results as odds ratios of one-year and two-year statin adherence for one standard deviation increase in young adulthood cognitive ability (complete cases).
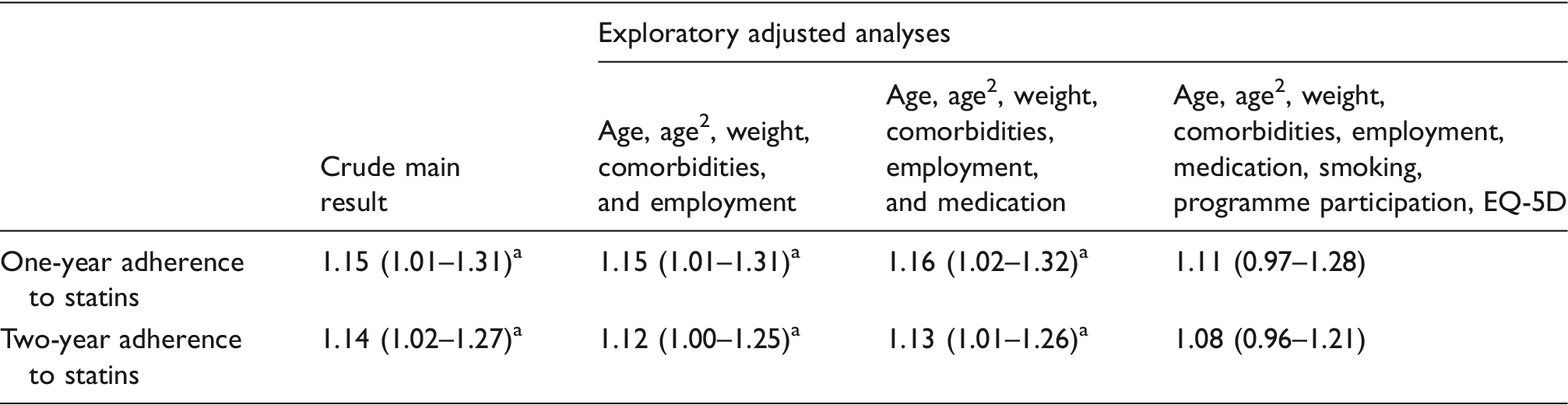
EQ-5D: European Quality of Life Five Dimensions Questionnaire.
Data presented as odds ratios (95% confidence intervals) for complete cases (n = 2613).
P < 0.05.
Health-related behaviours were the only covariates that markedly altered the CA–adherence associations and were therefore explored in depth. After separate adjustment for self-reported days of exercise during the previous week (OR 1.14 (CI 1.02–1.27), P = 0.021), participation in secondary prevention programmes (OR 1.12 (CI 1.00–1.25), P = 0.041) and EQ-5D scores (OR 1.13 (CI 1.02–1.26), P = 0.025), smoking was the only substantial modifier of the one-year CA–statin adherence association (OR 1.09 (CI 0.98–1.22), P = 0.119). We therefore modelled CA on smoking using multinomial logistic regression with never-smoker as the reference category. This rendered substantial negative associations (OR for being a current smoker 0.60 (CI 0.55–0.66), P < 0.001; for being a previous smoker OR 0.79 (CI 0.71–0.88), P < 0.001) per 1 SD increase in CA.
Discussion
The main findings of this study were that CA assessed in young adulthood was associated with both one-year and two-year statin adherence about 30 years later in a large sample of first MI male patients who were prescribed statins for the first time. Except for smoking, these associations remained significant after adjusting for more than 20 covariates.
Only smoking substantially attenuated the CA–statin adherence association. Smoking could not reasonably have had any effect on CA estimated 30 years earlier and was highly unlikely to influence current statin adherence. We therefore suggest that this attenuation is not causal, but instead a selection effect. Previous studies have also shown that smokers have a lower childhood CA 28 and lower adult CA. 18 As CA is a distillate of fundamental cognitive functions such as memory and executive function,10,11 a reasonable interpretation is that lower levels in these functions affect both persistence in taking statins and the tendency to smoke.
Previous research has suggested that patients with a low CA early in life are less likely to manage their lifestyle risk factors.15–17,20,29–32 Our study adds new knowledge that extends this pattern to first MI men and statin medication.
Strengths, limitations and future research
The risk of confounding through selection bias due to patients with a lower CA not seeking appropriate care or cooperation or self-reporting bias was substantially reduced by using data registered by health professionals in national quality registers. This suggests a high generalizability of findings to the subpopulation under study, supported by high data quality and accuracy of estimates due to highly standardized data collection procedures. Although residual confounding cannot be excluded a priori, the 30-year time lag between exposure and outcome and extensive covariate control indicates a causal link from CA to statin adherence. CA was estimated post-puberty in young adulthood when individual CA has largely fixated, before CA starts to degenerate due to ageing and when growth-fixated CA holds a minimum chance of confounding by physical trauma. The outcome and covariates were measured at or before 60 years of age when abnormal age-related cognitive decline is rare.
However, this limits the conclusions to relatively young first MI males. Future research should also include older and female patients and patients with re-infarction. Another limitation was that measurements were analysed at fixed time-points. Complementary time to event designs might shed more light on the present findings. It might also be beneficial to investigate which attitudes are related to adherence. 15 Potential biases demand further investigation and future research may include additional socioeconomic status variables, preferably education, job status and income, simultaneously keeping in mind that these variables are, to a substantial extent, proxies for CA that lie in the causal pathway of CA and health/risk behaviour.11,17,32–36 Following established epidemiological practice, adjusting for socioeconomic status variables is therefore probably incorrect. 37 With such adjustments, we would expect attenuation of the CA–adherence association. Such over-adjustment bias probably occurred when we adjusted for smoking. Military pre-selection, i.e. less frequent psychometric testing of those with very low CA, might also have attenuated the CA–adherence association.
Clinical implications
Our findings and the accumulated knowledge within cognitive epidemiology suggests that clinicians should be aware that CA is a stable risk indicator for a range of cardiovascular risk-reducing behaviours and for statin adherence. Secondary prevention might therefore benefit from considering CA as informing tailored care. Although we cannot change CA directly, it might be possible to tailor the context and treatment with respect to patients’ CA.
Conclusions
CA estimated in young adulthood is a substantial risk indicator for one- and two-year statin adherence 30 years later in first MI man aged ≤60 years. CA assessment might prove valuable for further targeting of secondary prevention efforts seeking to improve statin adherence. Future research should include other socioeconomic variables and also older and female patients.
Footnotes
Acknowledgement
We are deeply grateful to the SWEDEHEART patients.
Author contribution
JW, CL, GM, CH, and EO designed the study, interpreted the findings, revised the manuscript and approved its final form and submission. JW analysed the data and drafted the manuscript. All authors agreed to be held accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The Swedish Research Council for Health, Working Life, and Welfare (2014-4947), the Vårdal Foundation (2014-0114) and U-CARE (2009-1093) supported this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.