
Abstract
Background
A previous economic analysis of self-management, that is, self-monitoring with self-titration of antihypertensive medication evaluated cost-effectiveness among patients with uncomplicated hypertension. This study considered cost-effectiveness of self-management in those with raised blood pressure plus diabetes, chronic kidney disease and/or previous cardiovascular disease.
Design and methods
A Markov model-based economic evaluation was undertaken to estimate the long-term cost-effectiveness of self-management of blood pressure in a cohort of 70-year-old ‘high risk’ patients, compared with usual care. The model used the results of the TASMIN-SR trial. A cost–utility analysis was undertaken from a UK health and social care perspective, taking into account lifetime costs of treatment, cardiovascular events and quality adjusted life years. A subgroup analysis ran the model separately for men and women. Deterministic sensitivity analyses examined the effect of different time horizons and reduced effectiveness of self-management.
Results
Base-case results indicated that self-management was cost-effective compared with usual care, resulting in more quality adjusted life years (0.21) and cost savings (–£830) per patient. There was a 99% chance of the intervention being cost-effective at a willingness to pay threshold of £20,000 per quality adjusted life year gained. Similar results were found for separate cohorts of men and women. The results were robust to sensitivity analyses, provided that the blood pressure lowering effect of self-management was maintained for more than a year.
Conclusion
Self-management of blood pressure in high-risk people with poorly controlled hypertension not only reduces blood pressure, compared with usual care, but also represents a cost-effective use of healthcare resources.
Background
Hypertension is a leading risk factor for cardiovascular mortality and morbidity worldwide.1,2 Despite evidence of cost saving from antihypertensive treatment, 3 and improvements in blood pressure (BP) monitoring, management and treatment,3,4 significant numbers of people remain inadequately controlled hence new models of care are required. 5 Self-management of hypertension, in which an individual self-monitors their own BP and adjusts their own medication has been shown to lead to significantly lower BP in hypertension, including in those with higher cardiovascular risk.6,7
The only economic analysis of self-management in the control of hypertension to date demonstrated that tele-monitoring with self-titration in uncomplicated hypertension was highly cost-effective, with incremental cost-effectiveness ratios below £5000 per quality adjusted life year (QALY) gained for men and women, when modelled over patient lifetime. 8 However, subgroup analysis in the main trial suggested that the intervention might not be as effective in those with significant comorbidities, although patient numbers for this subgroup were small. 7 Therefore, the TASMIN-SR trial was undertaken to determine the effect of self-monitoring with self-titration of antihypertensive medication on systolic BP among hypertensive patients with suboptimal control and pre-existing cardiovascular disease, diabetes mellitus (DM) and/or chronic kidney disease (CKD), compared with usual care. A model-based probabilistic cost–utility analysis was undertaken as part of this study to assess the long-term cost-effectiveness of the self-management intervention in a ‘high risk’ patient population, compared with usual care.
Methods
A Markov cohort model, built in TreeAge Pro (TreeAge Software Inc, Williamstown, MA, USA), was developed to estimate the long-term cost-effectiveness of self-management of BP compared with usual care, in patients with hypertension and a history of stroke, coronary heart disease (CHD), DM or CKD. The analysis used the results of the TASMIN-SR trial on BP, extrapolating these to long-term risk of cardiovascular endpoints (see below). Full details of the trial methods and results have been described in detail elsewhere.6,9 The model was run over a lifetime (30 year) time horizon using a six-month time cycle, with results presented from a UK National Health Service (NHS) and personal social services perspective.
Study population
The base case analysis considered a cohort of 70-year-old patients (39% women) with suboptimal hypertension, BP ≥130/80 mmHg at baseline, combined with a history of stroke, CHD, DM or CKD. 6 Patients had at least one of four main underlying conditions (DM, stroke, CHD and CKD), to be eligible with 15 possible combinations of high risk conditions in total. Further details of the combined risk conditions are available in supplementary Table 2.
Interventions
Patients randomly assigned to usual care booked an appointment for a routine BP pressure check and medication review with the study general practitioner. Thereafter, usual care consisted of the participants seeing their general practitioner and or nurse for routine BP measurement and adjustment of medication at the discretion of the health professional. Patients randomly assigned to self-management were trained to self-monitor BP and to self-titrate their antihypertensive medication following a predetermined plan, in two or three sessions, each lasting around an hour. Following training, patients adjusted their antihypertensive medication based on their monthly self-monitored BP readings. 9
Model structure
A patient entered the model in the high-risk health state and could move to another health state if they experienced one of three possible cardiovascular events (stroke, myocardial infarction (MI), unstable angina (UA)), or died from other causes (Figure 1). After a cardiovascular event, individuals could survive from that event or die within the first six months. Those who survived an event subsequently moved to a chronic health state for that condition until death, with no recurrences of cardiovascular events. For each chronic health state, an ongoing healthcare cost was applied every time cycle and quality of life was permanently reduced. Movement between health states was defined by transition probabilities, which represented the risk of experiencing an event within each six-month time cycle.
Markov model.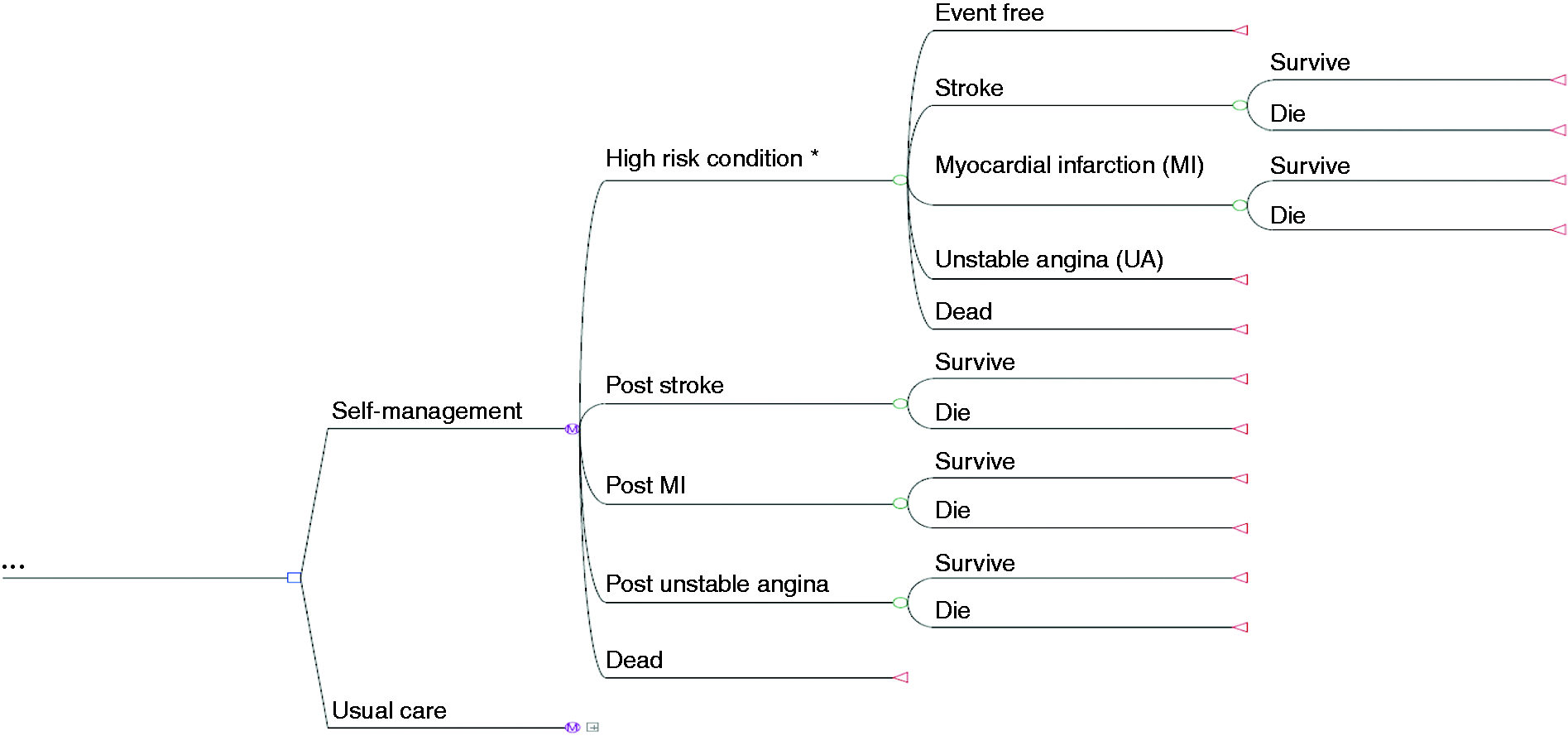
Model parameters
Model parameters.

Included annual costs of drugs per patient, average general practitioner and practice nurse cost of consultation(s) and the costs of the intervention. The cost difference between self-monitoring and usual care was driven by the cost of the intervention
For greater detail see supplementary document.
CVD: cardiovascular disease; CKD: chronic kidney disease; DM: diabetes mellitus; MI: myocardial infarction; UA: unstable angina.
Systolic BP reductions recorded in the trial at six months (11.4 mmHg and 5.5 mmHg for the intervention and control arms) and at 12 months (15.0 mmHg and 5.8 mmHg for the intervention and control arms) were extrapolated to age-related risk reductions for CHD (comprising both MI and UA) and stroke, using Law et al. 18 (Table 1). Relative risks for CHD and stroke related to six and 12 month BP reductions are reported in Table 1. The model assumed that BP remained static for the first six-month cycle of the model, then reduced as per the six-month trial results for the second model cycle followed by the 12-month trial reductions thereafter with the between groups differences assumed constant in the base case. The probabilities of death from MI and stroke within a year of the event are reported in Table 1 and applied to the first year after an event (first two cycles in the model). Life tables were used to determine overall mortality, dependent on age and gender. 19
Resource use and costs
Costs are reported in UK pounds at 2011/2012 prices. Resource use related to ongoing BP monitoring in primary care, self-management and prescription of antihypertensive agents was obtained from the TASMIN-SR trial at 12 months follow-up. For self-management, equipment and training costs were annuitised at an annual rate of 3.5% and based on a lifetime of five years. 20 Replacement costs for the equipment and training were included at five yearly intervals over the lifetime of the model (see supplementary Table 3). Equipment used by individuals who died within any five-year interval was assumed to be discarded. Unit costs were applied to resource use and mean patient costs per six months were calculated for both randomly assigned groups, and applied to the initial high risk health state. Costs for acute and chronic cardiovascular event states were obtained from published studies14,21–23 (see Table 1).
Utility values
The primary outcome measure was QALYs. All utility scores used in the model are shown in Table 1. The utility values for the starting high risk health state were obtained from the TASMIN-SR trial, in which the overall mean EQ-5D score for hypertensive patients at baseline was used to estimate utilities. This was adjusted for age group using weights calculated from Ara and Brazier, 24 which allowed the overall reduction in quality of life with increasing age to be incorporated in the model. Acute events were assumed to happen approximately three months into a six-month cycle and individuals stayed in that acute state for three months before moving into a chronic state. Therefore, utilities for the acute state were applied mid-way through the six-month cycle and chronic health state utilities were applied at the start of the subsequent cycle (Table 1). Health state utilities for cardiovascular events were applied multiplicatively to the age-related high risk health state utility values.
Analysis
A cost–utility analysis was undertaken from a UK NHS and personal social services perspective. For the base-case analysis, 15 separate cost-effectiveness analyses were run, one for each combination of high risk conditions assessed in the model. The final cost-effectiveness results correspond to the trial population-weighted average of costs and QALYs and are reported in terms of the incremental cost per QALY gained. 25 Analyses were also separately run for men and women. Costs and outcomes were discounted at an annual rate of 3.5%. 26
Uncertainty in the model results was assessed using sensitivity analyses. Deterministic sensitivity analysis was undertaken around key parameters and assumptions. The time horizon for the model was varied from 30 years (lifetime) to between one year and 20 years, to determine whether the intervention was cost-effective in the shorter term. The assumption regarding the long-term effectiveness of the intervention was tested by assessing the impact of limiting the additional effect on BP lowering to years of self-management.1,2,5,10 Additional sensitivity analyses altered long-term cardiovascular event costs by 30% (up and down). Finally, all analyses were re-run using the unadjusted trial data, which showed marginally smaller reductions in BP (11.4 mmHg and 5.8 mmHg for the intervention and control arms at six months and 14.9 mmHg and 6.0 mmHg, respectively, at 12 months). When possible, data were entered into the model as distributions in order that a probabilistic sensitivity analysis could be undertaken to incorporate parameter uncertainty. Gamma distributions were fitted to all costs obtained from the TASMIN-SR trial and beta distributions were applied to the utility values. The parameters used for these distributions are shown in Table 1. The probabilistic sensitivity analysis was run with 10,000 second-order Monte Carlo simulations and cost-effectiveness planes and cost-effectiveness acceptability curves constructed to estimate the probability of self-management being cost-effective at different willingness-to-pay thresholds. 20
Results
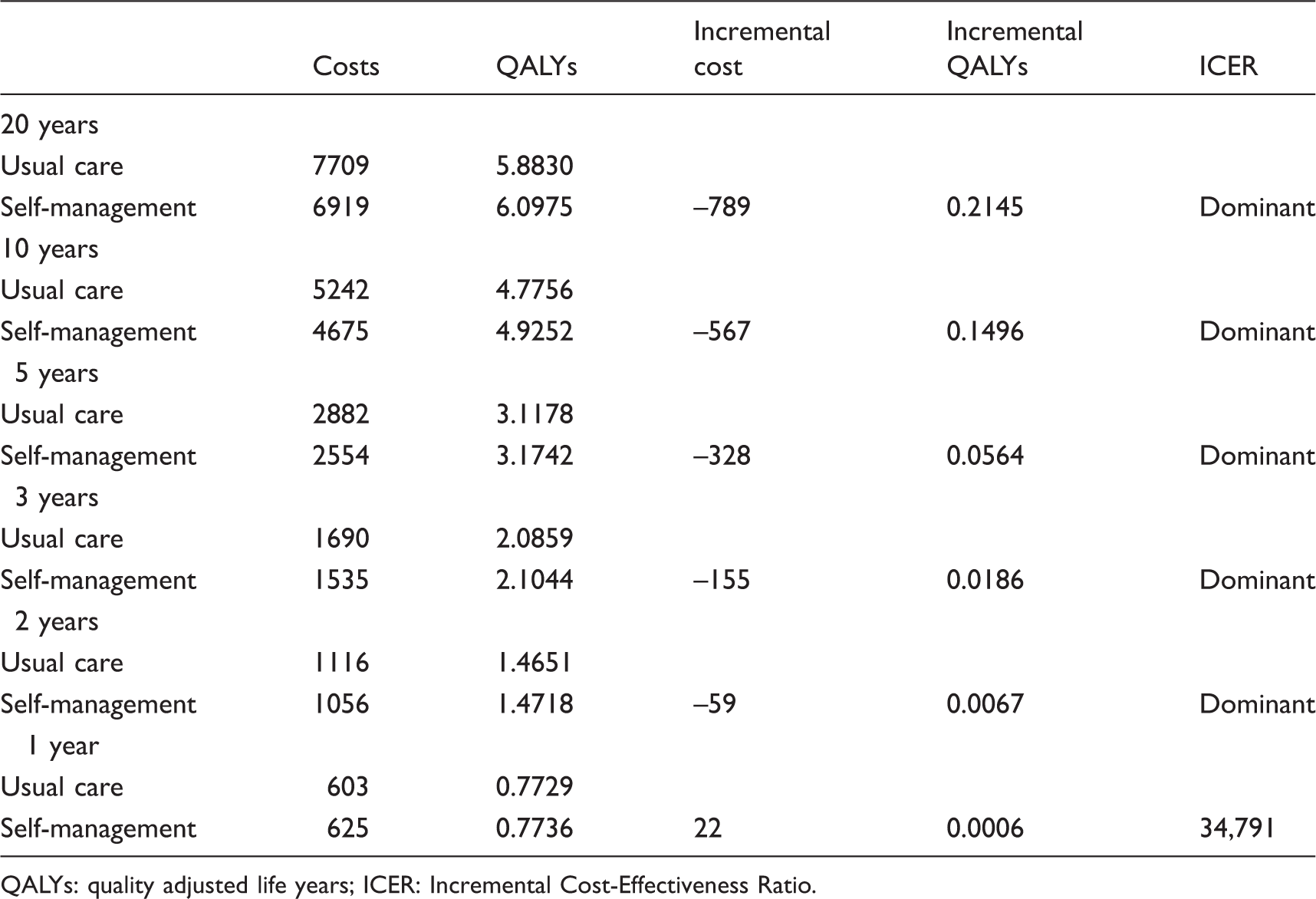
Results of cost-effectiveness analysis.
QALYs: quality adjusted life years; ICER: Incremental Cost-Effectiveness Ratio.
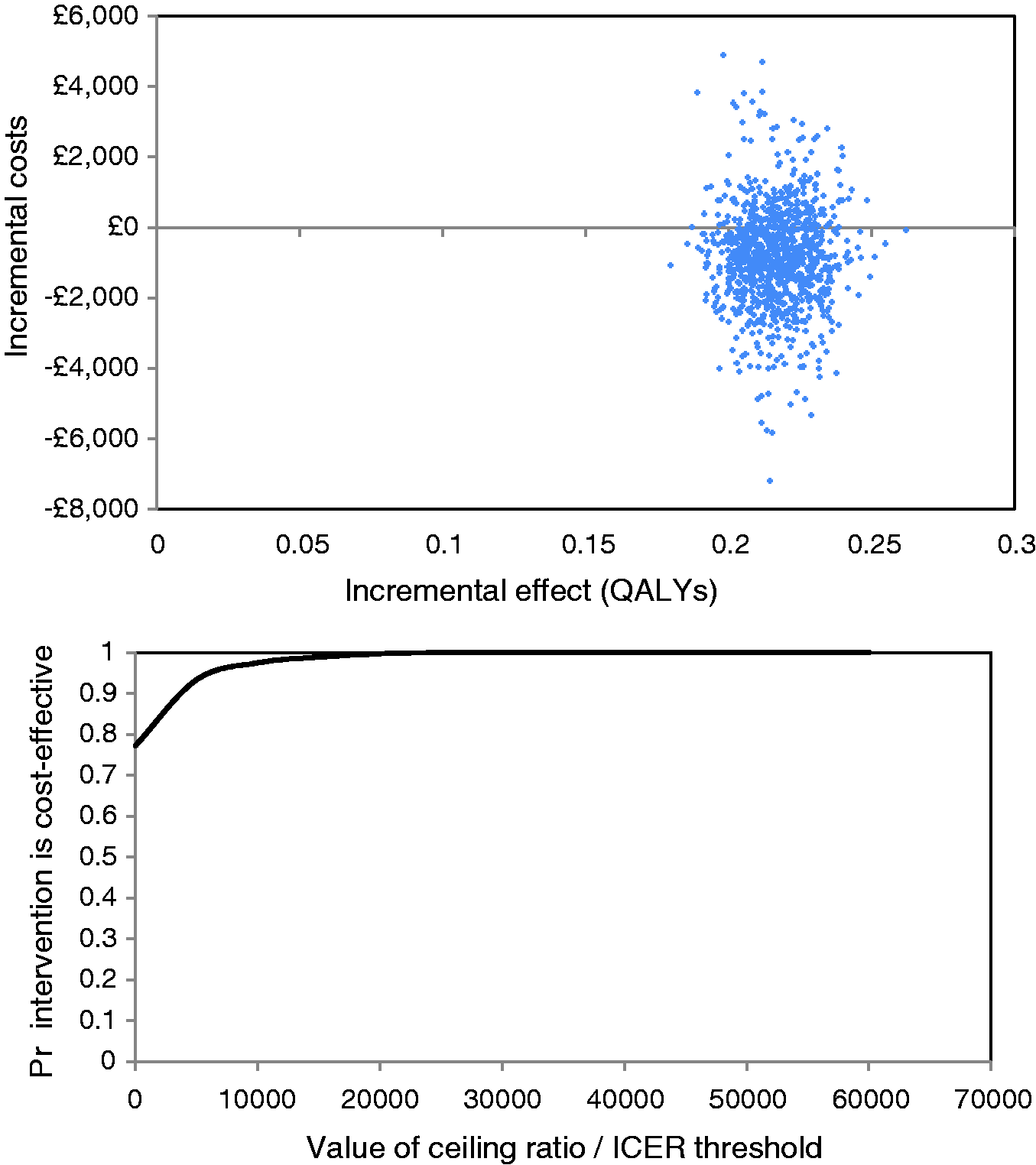
Base-case results.
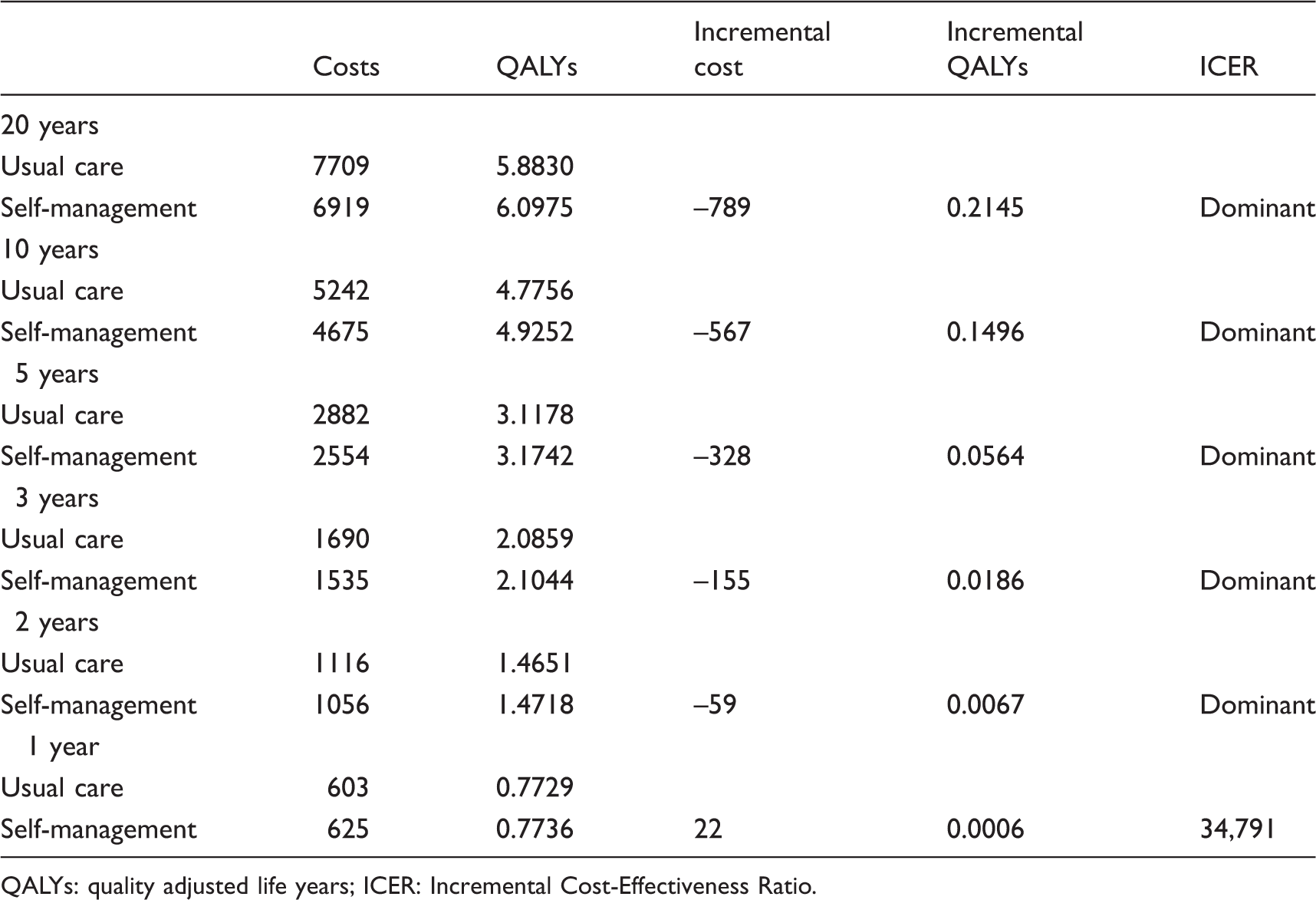
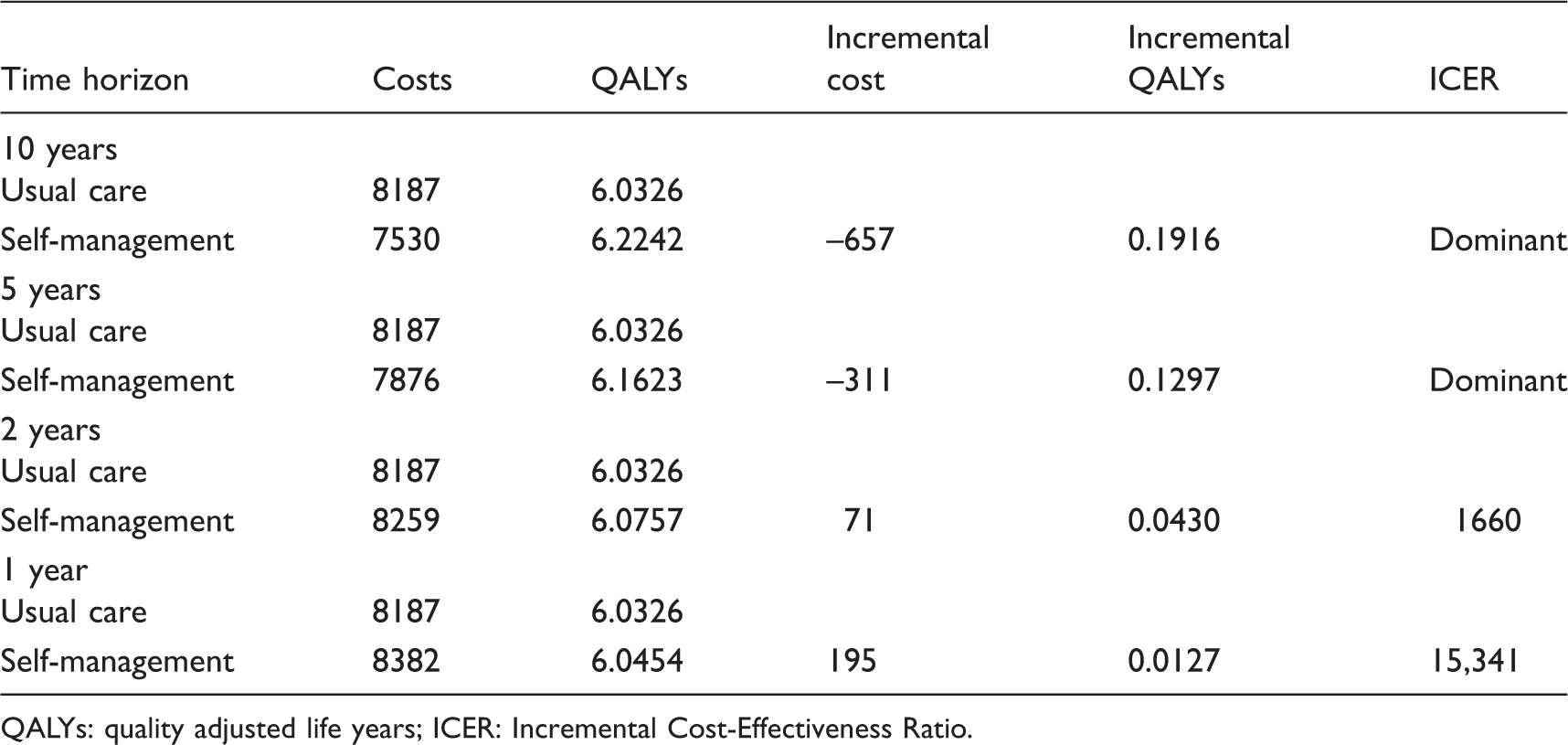
Sensitivity analyses: cost-effectiveness by time horizon.
QALYs: quality adjusted life years; ICER: Incremental Cost-Effectiveness Ratio.
Sensitivity analyses: cost-effectiveness by reducing the additional effect of self-management to blood pressure lowering at four different time points.
QALYs: quality adjusted life years; ICER: Incremental Cost-Effectiveness Ratio.
Discussion
This is the first study to present results of the cost-effectiveness of self-management of BP compared with usual care in a high risk population with suboptimally managed hypertension and significant cardiovascular comorbidity. The base-case analysis suggests that self-management of BP is cost-effective and is likely to be dominant (i.e. it is less costly and produces more QALYs) compared to usual care.
The main driver of this result is the estimated decline in the risk of cardiovascular events associated with the observed additional BP lowering achieved with self-management, and this explanation also holds for the greater benefit seen for men. This result was robust to sensitivity analysis unless the time horizon was reduced below two years or the observed BP lowering effect of self-management did not continue beyond a year.
Relationship with other literature
Previous economic studies have evaluated the cost-effectiveness of self-monitoring rather than self-management (self-monitoring plus self-titration of antihypertensive medication) and only one previous economic analysis of self-management has been undertaken (TASMINH2), 8 which found self-management to be cost-effective (£1624 and £4923 per QALY gained for men and women, respectively). 8 In this analysis, we found self-management to be even more cost-effective, reflecting the higher number of cardiovascular events predicted to have been prevented in the higher risk population, and the slightly greater reductions in BP that were observed in the TASMIN-SR trial.
Strengths and limitations
This study used cost and outcome data of trial participants, 6 who may differ from similar patients not taking part in the trial for instance being more adherent and healthier. 27 The strongly positive results, however, suggest that such an intervention would be cost-effective even in a less compliant population. The costs of long-term and acute care were taken from estimates in the literature and a number of assumptions were made about the annual probabilities of cardiovascular events by risk conditions based on best published information. A key assumption was that of the prolonged effectiveness of the intervention. In both TASMINH2 and TASMIN-SR, the difference in BP reduction between trial arms continued to diverge between six and 12 months, suggesting that the effect may be maintained over time. Indeed, an 18 month post-trial follow-up of the HSM self-management trial found that BP continued to diverge over time, suggesting our assumption of maintenance of effect may even be conservative. 28 The sensitivity analyses showed that even if BP differences lasted only one further year and then returned to the effectiveness of usual care, self-management is still likely to be cost-effective. For simplicity, the model did not include subsequent cardiovascular events. Given that the main driver of costs was events and the main driver of events was BP, it would be expected that a model including secondary and subsequent events would show self-management to be even more cost-effective than usual care. The model considers patients with comorbidities and additional risk factors (e.g. age, gender). Arguably, a more complex model such as individual patient level simulation could be more appropriate in this situation, as this type of model can incorporate patient history more efficiently, overcoming the limitations of Markov models. 29 Finally, an assumption has been made regarding the differential effect of BP lowering between the intervention and control groups. Systematic reviews suggest that lowering BP below 140/90 mmHg is as effective as lowering BP to 140/90 mm Hg, 18 but it is fair to say that the evidence of benefit is stronger in stroke and DM than in CHD or CKD.10,30–32
Clinical implications
These results suggest that the benefits of BP reduction seen in the trial can be achieved in a highly cost-effective manner. The up-front costs of implementation of self-management of hypertension in high risk groups are relatively modest (£14.6 equipment and £20.0 training), and are soon repaid by future maintenance of quality of life and reductions in costs from reduced cardiovascular events. The very high likelihood of cost-effectiveness from both this and the previous analyses suggest that self-management is a strong candidate for implementation.
Conclusions
The results of this model-based economic evaluation suggest that self-management of hypertension in high risk patients is a cost-effective strategy in the short and long term, resulting in QALY gains and cost savings. Self-management of BP in high risk patients represents an important new addition to the management of hypertension in primary care.
Footnotes
Acknowledgements
The authors would like to thank Dr Billy Kaambwa for kindly sharing all the information from the TASMINH2 cost-effectiveness study with the team and Amanda Davies and Fran Palmer for administrative work on the project.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RJM has received research equipment from Omron and Lloyds Pharmacies. BW has worked in academic collaboration with Healthstats, Singapore, in developing novel blood pressure monitoring approaches. FDRH has received limited research support in terms of blood pressure devices from Microlife and BP TRU. No other disclosures were reported.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper presents independent research funded by the National Institute for Health Research (NIHR) under its programme grants for applied research programme (grant reference number RP-PG 0606-1153) and by the NIHR National School of Primary Care Research (NSPCR 16). The views expressed in this paper are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. Service support costs were administered through the primary care research network and collaborating comprehensive local research networks. RJM was supported by NIHR career development and professional fellowships, FDRH, PL and BW are NIHR senior investigators. RJM and FDRH receive support from the NIHR CLAHRC Oxford. FDRH also receives support from the NIHR School for Primary Care Research and the NIHR Oxford BRC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.