
Abstract
Trisomy 21 (T21) is associated in 40–45% of cases with heart defects, most commonly shunt lesions. These defects, if not repaired, can lead to irreversible shunt-induced pulmonary hypertension (i.e. Eisenmenger syndrome [ES]). In ES patients, intracardiac repair is no longer possible, but selective pulmonary vasodilators may increase exercise capacity and improve prognosis. This study aimed to estimate the prevalence of cardiac defects and ES in adult T21 patients and to assess the impact of T21 on treatment modalities and outcome in ES patients. A questionnaire was sent to 6906 Swiss physicians inviting them to indicate the number of adults with T21 under their care (survey report). We also analyzed all adults with ES (with and without T21) included in the Swiss Adult Congenital HEart disease Registry (SACHER) and studied the impact of T21 on the use of selective pulmonary vasodilators and survival. In the survey, 348 physicians cared for 695 adult T21 patients. Overall, 24% of T21 survey patients were known to have a cardiac defect, one in four with a defect had developed ES and 13% of those with ES were on specific pulmonary vasodilators. In SACHER, ES was present in 2% of adults with congenital heart disease and selective pulmonary vasodilators were used in 68% of ES patients with T21. In SACHER, survival during follow-up was worse with higher nt-proBNP levels (hazard ratio [HR] = 1.15 per 1000 units, 95% confidence interval [CI] = 1.02–1.29) and lower left ventricular ejection fraction (HR = 1.07 per percent decrease, 95% CI = 1.01–1.13). Age at inclusion and T21 did not affect survival. The prevalence of cardiac defects in adults with T21 in Switzerland is half the prevalence in children. T21 is over-represented among adults with ES. Raised awareness of the therapeutic options for T21 patients with ES is warranted.
Keywords
Trisomy 21 (T21) is the most common aneuploidy and affects one in 800–1000 live births.1,2 It is associated in 40–45% of cases with cardiovascular anomalies, most commonly an atrioventricular septal defect (40–45%), or a simple ventricular (30%) or atrial (15%) septal defect. 3 Infant mortality in T21 has decreased substantially in the past 50 years, partially due to the increasing use of cardiac surgery for repair of cardiovascular defects in early life. 4 As an example, mortality for infants with T21 in Sweden in the first year of life was 40% in 1970 and 4% in 2000. 5 At the same time, cardiac repair was offered to 39% of affected children with defects in 1973–1977 and to 97% in the years 1993–1997. 6 In Switzerland, a similar evolution took place: defect repair was the exception before the 1970s and became clinical routine in the last two decades.
Some T21 children with cardiac defects and no repair in early life survived to adult age and developed severe, irreversible shunt-induced pulmonary arterial hypertension (PAH), i.e. Eisenmenger syndrome (ES). 7 Intracardiac repair for shunt defects is no longer possible at this stage; therefore, families of adults with T21 and ES live with the perception that “nothing else can be done.” However, selective pulmonary vasodilators may increase exercise capacity and improve prognosis in ES patients, including those with T21.8,9
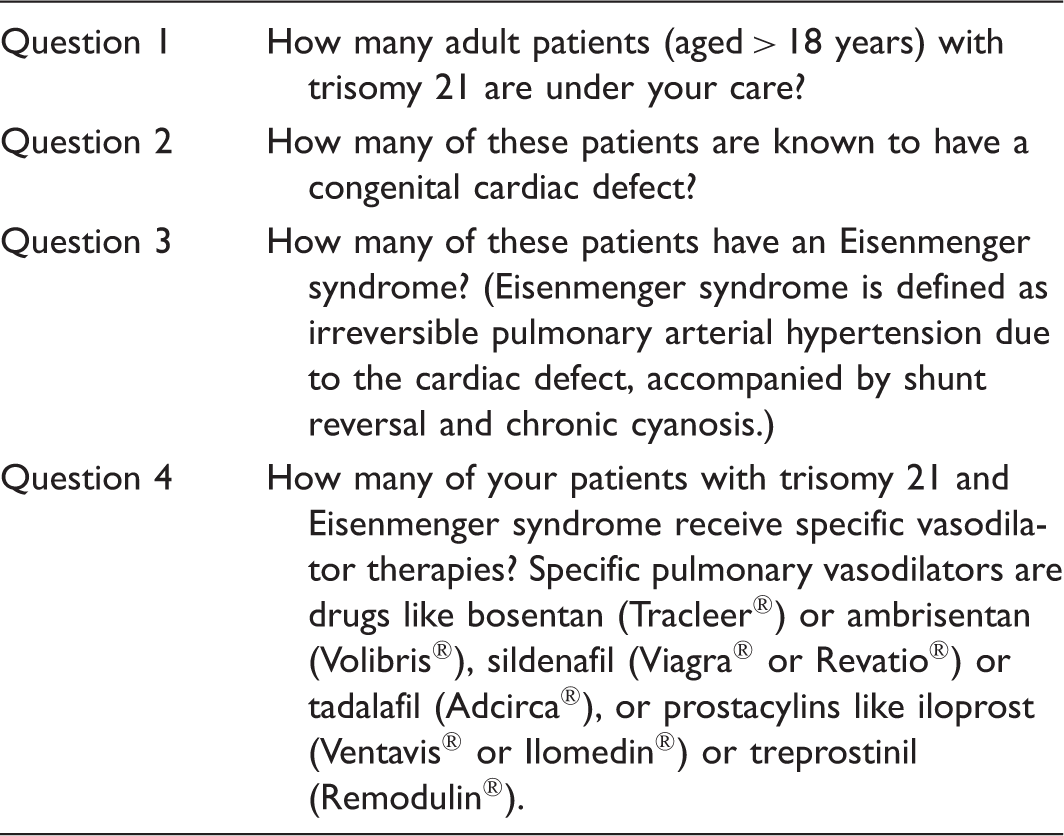
In 2013, the working group for adults and teenagers with congenital heart disease of the Swiss Society of Cardiology performed a nationwide survey among general practitioners in Switzerland, inviting them to indicate the estimated number of adults with T21 under their care, and the proportion of such patients with known cardiac defects, with ES, and on treatment with selective pulmonary vasodilators. In a second step, we identified adults with ES included in the Swiss Adult Congenital HEart disease Registry (SACHER) 10 followed at the University Hospitals Basel, Bern, or Zurich, and investigated their treatment modalities and outcome.
We hypothesized that treatment differences exist in ES patients with respect to selective pulmonary vasodilators, depending on whether they have T21 and whether they receive specialized care.
Methods
Trisomy 21 questionnaire.
SACHER analysis. The SACHER is a nationwide registry that was established in Switzerland in spring 2013 and prospectively follows adults with congenital heart disease. 10 Included are adults (aged >18 years) with structural congenital heart defects or Marfan syndrome. After informed consent was obtained, anonymized clinical data were entered in an online registry. The ethics review boards of all participating hospitals approved the registry and subsequent analysis of data. The SACHER contained a total of 3476 patients on 1 September 2017. We analyzed in detail data from 58 ES patients included at the GUCH units of the University Hospitals Basel, Bern, or Zurich. These three centers had included three of four SACHER patients (2552 of 3476) at that time and all centers have specialized programs for PAH on site. ES was defined as PAH with a non-restrictive intracardiac or extracardiac communication and chronic cyanosis due to shunt reversal. 11 The diagnosis has been established and confirmed in all cases by echocardiography. Cardiac catherization was not mandatory.
Patients' histories were assessed for the following parameters: baseline characteristics at the time of inclusion in the SACHER, survival status at 1 September 2017, defect anatomy and concomitant medication with a special focus on selective pulmonary vasodilators. Of note, no uniform criteria when to start selective pulmonary vasodilators were used in the participating centers. The decision was left to the treating physician. Nevertheless, all patients in New York Heart Association (NYHA) functional class (FC) III were offered specific drugs. Exercise capacity was assessed using the 6-min walking distance (6MWD) and the NYHA FC. Echo findings at the time of last follow-up were studied for the presence of right or left ventricular dysfunction, pericardial effusion, and the degree of tricuspid regurgitation. Any history of suspected or confirmed paradoxical embolism, hemoptysis, and sustained arrhythmia before or after inclusion in the SACHER was documented. Bloodwork including red blood count, renal function, thyroid function, and NT-proBNP at the time of inclusion was noted.
Continuous data are shown as mean with standard deviation or as median with the interquartile range (IQR), as appropriate. Comparison between baseline characteristics in ES patients with and without T21 were performed using the unpaired Student's t-test for normally distributed continuous variables or with the Mann–Whitney U test for non-normally distributed data. Distribution of categorical data between groups was compared using the chi-square test. Survival analysis was performed for all-cause mortality. We calculated survival curves using the Kaplan–Meier method; survival differences in ES patients with and without T21 after inclusion in SACHER were compared using the log-rank test. In a Cox proportional hazards model, age at inclusion in SACHER, T21, and univariate significant predictors of survival were entered in a multivariate regression model. In all analyses, the null hypothesis was rejected for P values < 0.05. All calculations were performed using STATA 12 statistical software.
Results
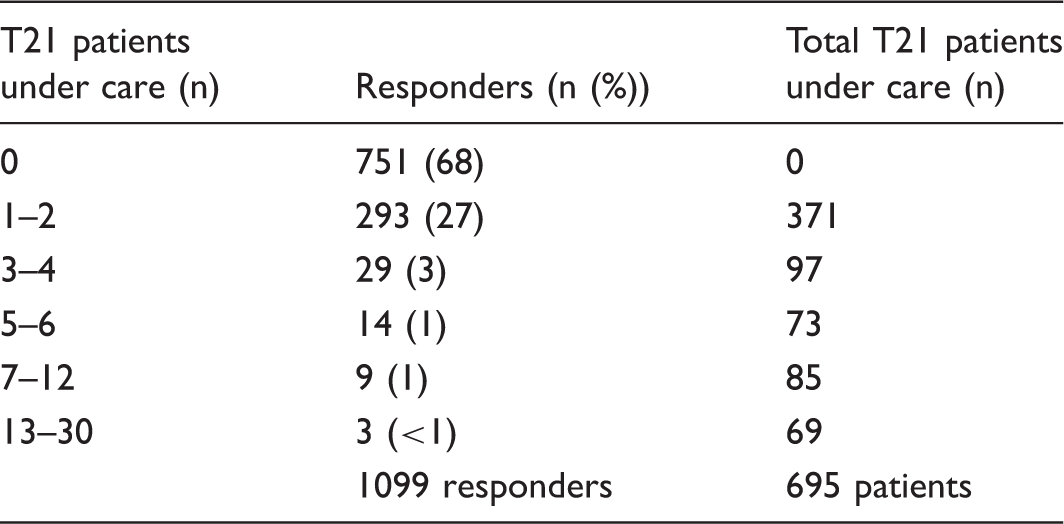
Trisomy 21 survey. A total of 6906 letters were sent out. After three months, 1097 responses were received (16% response rate). The response rate varied between 8% (region Appenzell Innerrhoden) and 32% (region Glarus), with no major differences between the different language regions and between urban or rural areas (Fig. 1). Of the responding physicians, 751 (68%) had no adult T21 patient under their care (Table 2). A total of 348 general practitioners cared for 695 adult T21 patients (median of one patient per physician; IQR = 1–2). Of these 695 patients, 165 (24%) were reported to have a cardiac defect. A total of 38 (23%) T21 patients (out of the 165 with a presumed cardiac defect) were diagnosed as ES and five of them (13%) were on specific pulmonary vasodilator therapies: three patients were on Bosentan; one patient was on Sildenafil; and one patient was on dual therapy with Bosentan and Iloprost inhalation at the time of the last visit.
Average response rate (in percent) to the T21 survey for different regions within Switzerland. The response rate was comparable in the Italian, French, and German speaking parts of the country. Number of adult T21 patients under care.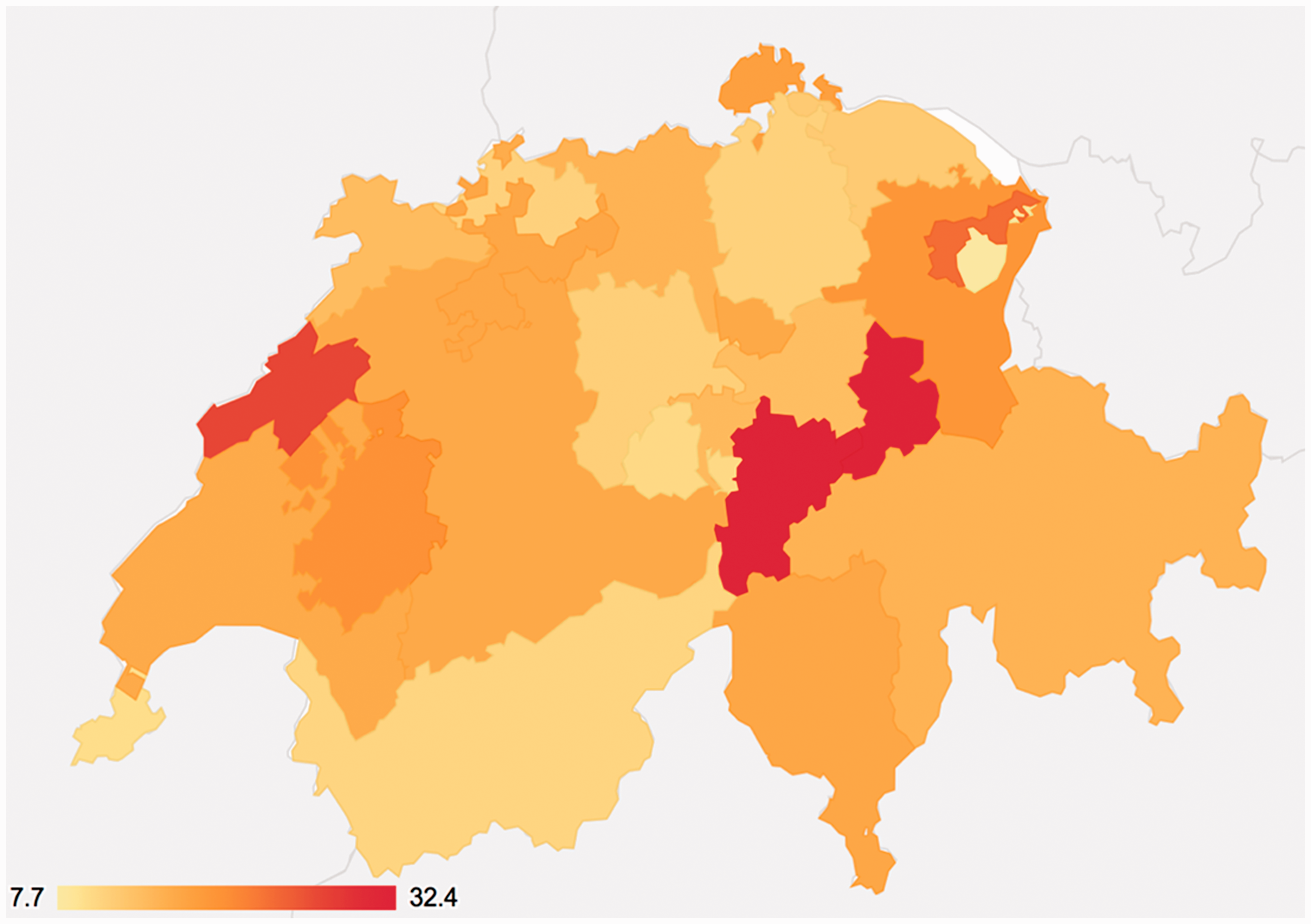
Characteristics of T21 vs. non-T21 patients in SACHER.
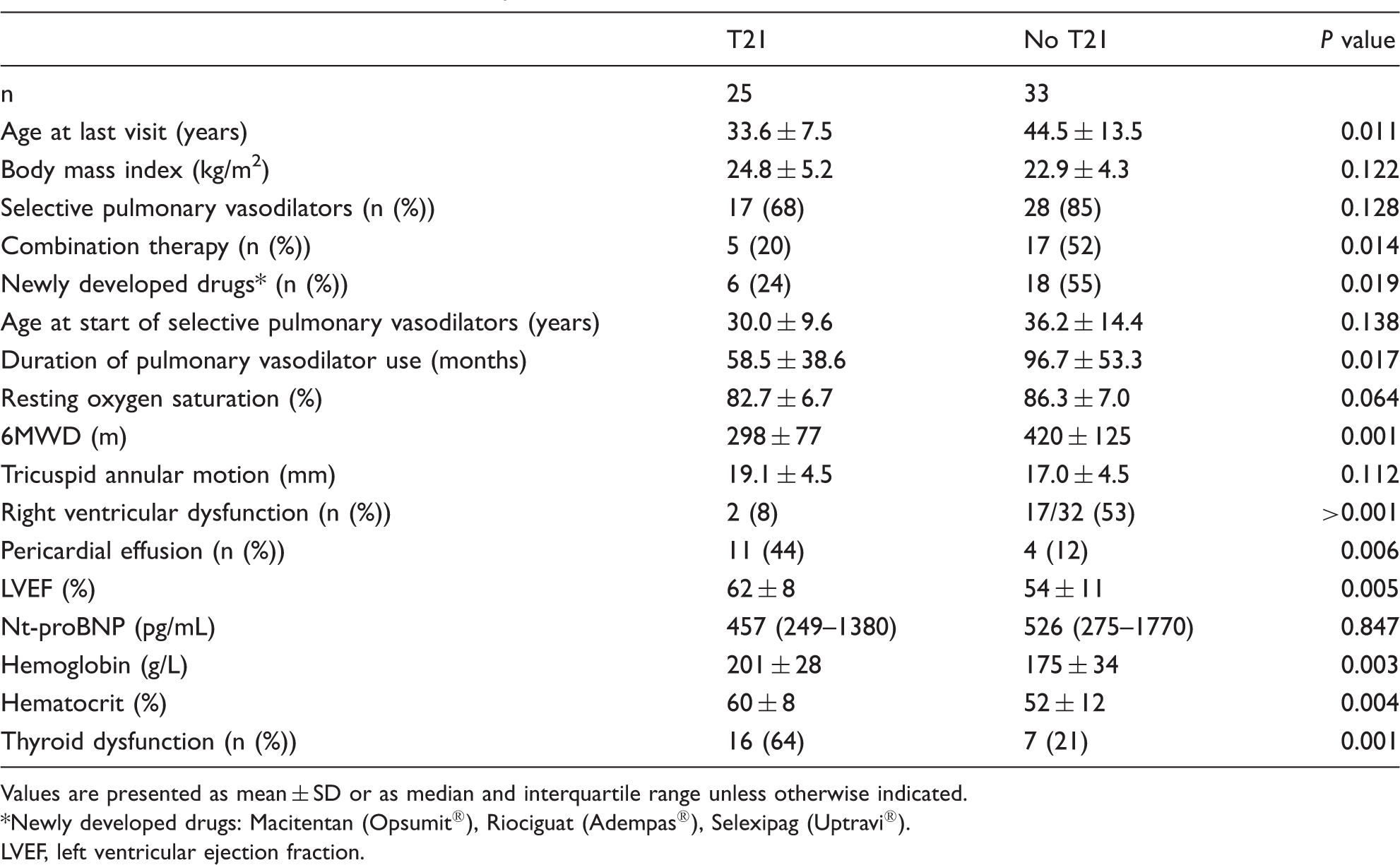
Values are presented as mean ± SD or as median and interquartile range unless otherwise indicated.
Newly developed drugs: Macitentan (Opsumit®), Riociguat (Adempas®), Selexipag (Uptravi®).
LVEF, left ventricular ejection fraction.
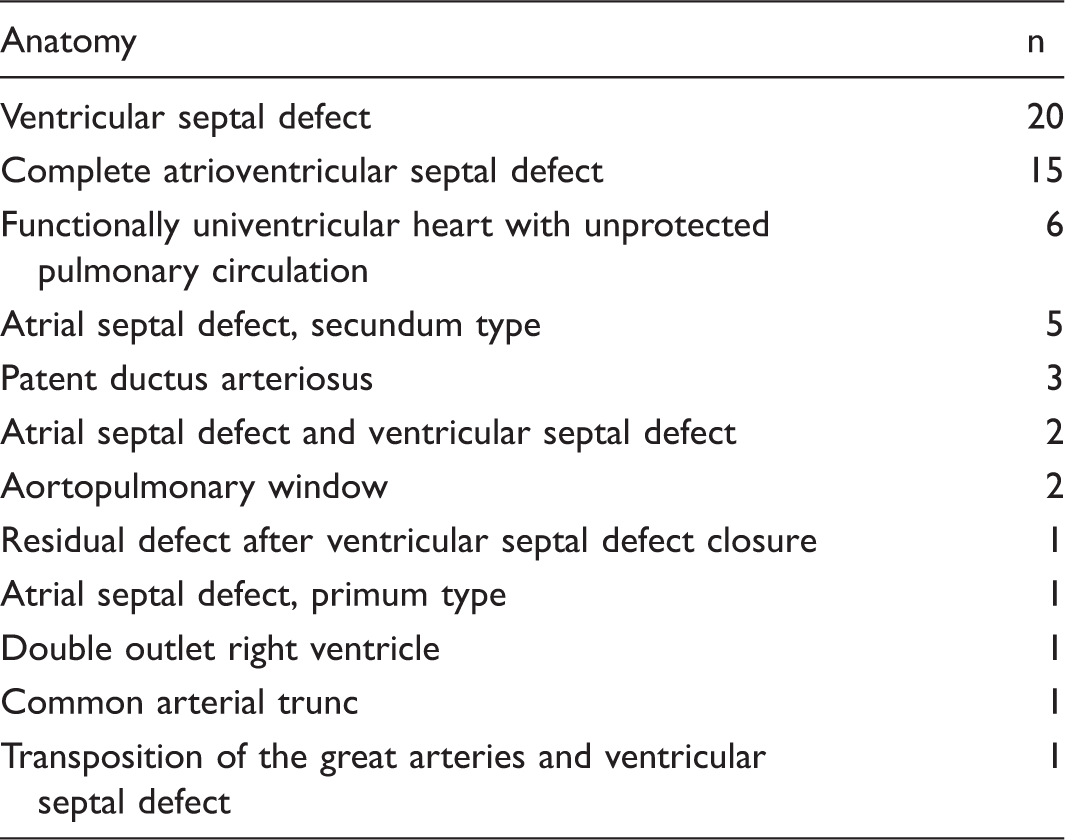
Anatomy of cardiac defects of Eisenmenger patients in SACHER.
A total of 45 SACHER ES patients (78%) were on selective pulmonary vasodilators: 23 patients were on single therapy; 18 on dual therapy; and four on triple therapy. The most commonly used vasodilators were endothelin-receptor antagonists (bosentan or macitentan, no patients were on ambrisentan) in 44 patients, followed by phosphodiesterase-5 (PDE5) inhibitors (sildenafil or tadalafil) in 26 patients. A total of five patients were put on riociguat; four of them were previously on sildenafil or tadalafil. Prostacylins or their analoga were used in seven patients (six were on inhalation iloprost, one was switched to selexipag, and another patient was newly started on selexipag). The mean age when patients were started on pulmonary vasodilators was 33.8 ± 13.0 years and the mean duration of drug therapy was 81.8 ± 51.0 months. In SACHER, the presence of T21 had no effect on the proportion of patients on selective pulmonary vasodilators, nor on the age when this therapy was started (Table 3). ES patients without T21 were, however, more often on combination therapy or on one of the newly developed pulmonary vasodilators, i.e. macitentan, riociguat, or selexipag. The proportion of T21 patients with ES treated with selective pulmonary vasodilators was significantly higher in SACHER compared to the T21 population reported in the nationwide survey (17/25 vs. 5/38, P = 0.011).
Eleven patients (19%) had a history of presumed or documented paradoxical embolism and 13 (22%) had sustained atrial arrhythmias. The CHA2DS2-VASc score did not differ between patients with and without T21 (mean = 1.8 ± 0.8) but was significantly higher in patients with a history of presumed paradoxical embolism (2.7 ± 0.6) compared to patients without such an event (1.7 ± 0.7; P = 0.001). None of the 11 patients with an event had a score < 2. A total of 20 ES patients (35%) had bleeding complications, most of the time hemoptysis (14 patients) or gastrointestinal bleeding (three patients). There was no difference in bleeding events between patients with and without T21. The HAS-Bled score was significantly higher in patients with a bleeding history (2.0 ± 1.0 vs. 0.7 ± 0.9; P < 0.001). None of the 20 (35%) ES patients with a HAS-Bled score 0 suffered bleeding complications.
Overall, disease-related morbidity consisting of arrhythmias, paradoxical embolism, or bleeding was observed in 33 (57%) patients. In a logistic regression model, disease-related morbidity was only related to age (per 10 years of age: odds ratio [OR] = 2.2, 95% confidence interval [CI] = 1.2–4.1), but not to T21 nor defect complexity.
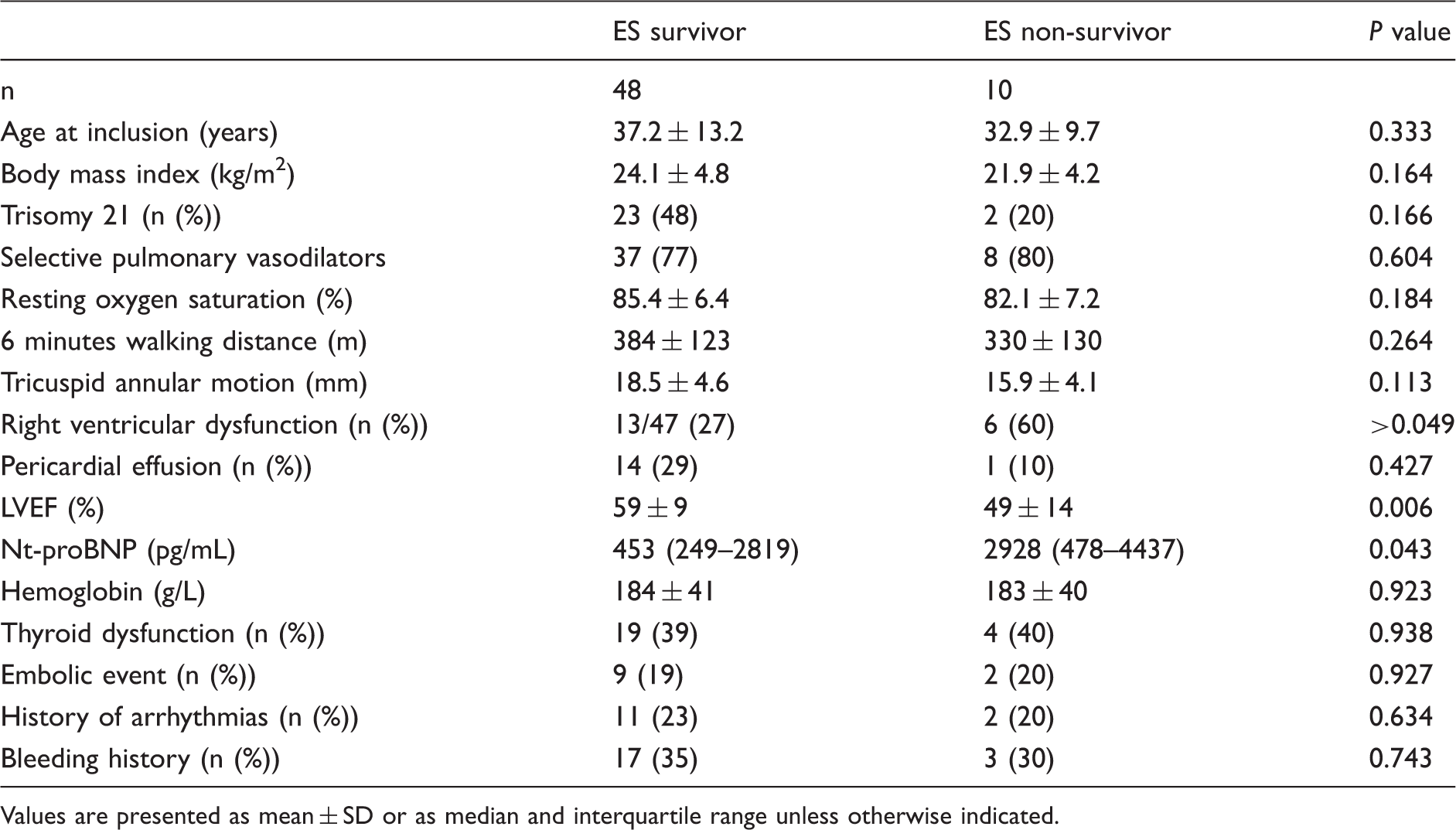
A total of 10 (18%) ES patients died at a mean age of 34.1 ± 10.1 years during the follow-up period after inclusion in SACHER. There was no difference with respect to gender, defect anatomy, the proportion of patients treated with selective pulmonary vasodilators, supplemental oxygen therapy, 6MWD, resting oxygen saturation, hemoglobin or hematocrit, thyroid dysfunction, paradoxical embolism, bleeding history, or arrhythmias between survivors and non-survivors. However, echocardiography showed more often right ventricular dysfunction and lower left ventricular ejection fraction (LVEF) in non-survivors compared to survivors, and also the NT-proBNP differed significantly (Table 5). In a Cox regression analysis corrected for age, with T21, nt-proBNP levels and LVEF as predictors of death during follow-up, only higher nt-proBNP levels (hazard ratio [HR] = 1.15 per 1000 units, 95% CI = 1.02–1.29) and lower ejection fraction (HR = 1.07 per percent decrease, 95% CI = 1.01–1.13) were independent predictors of outcome. In a Kaplan–Meier survival analysis, there was again no survival difference in ES patients with and without T21 (Fig. 4, P = 0.553).
Survival in Eisenmenger patients with and without T21 with the corresponding CIs, after inclusion in SACHER. The timeline denotes follow-up duration in months. Clinical characteristics of ES survivors vs. non-survivors in SACHER. Values are presented as mean ± SD or as median and interquartile range unless otherwise indicated.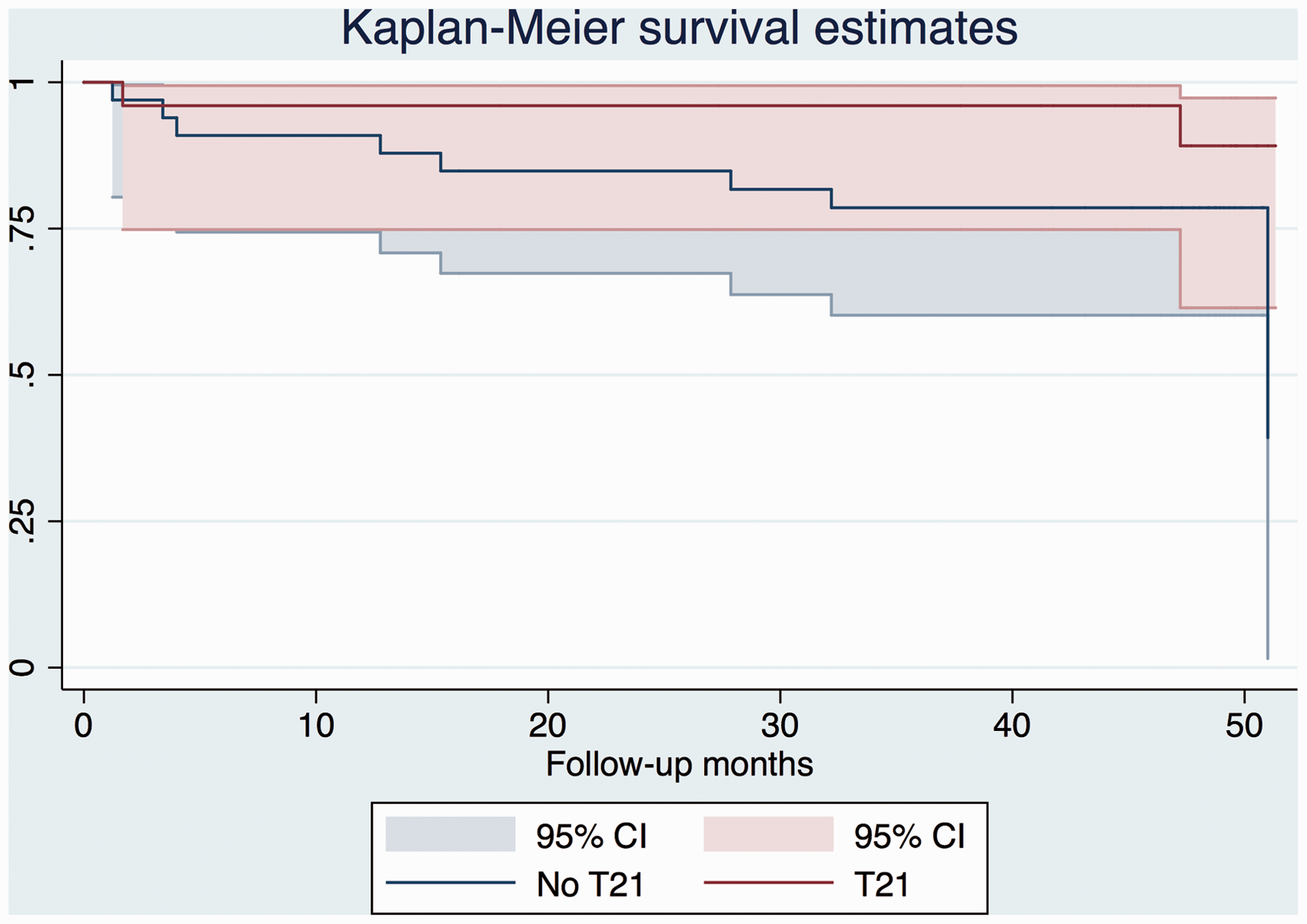
Discussion
The reported prevalence of cardiac defects in Swiss adult T21 patients in our survey is half of the documented prevalence in contemporary children with T21. 3 In addition, T21 patients are over-represented in SACHER among patients with ES. If T21 ES patients are followed in specialized clinics, they are as likely as the non-trisomy patients to receive selective pulmonary vasodilators and the survival rates are comparable between these two groups of ES patients. In the SACHER ES cohort, survival during follow-up was mainly dependent on cardiac function, i.e. the degree of neurohormonal activation and particularly of LVEF.
Based on these observations one may conclude that 30–40 years ago, as in other countries, children born in Switzerland with T21 and a cardiac defect were less likely to undergo cardiac surgery than children without T21, and therefore faced increased childhood mortality and morbidity. Another reason for the low prevalence of reported congenital heart disease in contemporary adults with T21 is the possibility of under-diagnosis of such defects. Currently, children born with T21 undergo routine echocardiography after birth, even in the absence of a heart murmur. 14 Many adult T21 patients may not have undergone an echocardiography in their childhood. Therefore, cardiac defects with minor clinical findings and a paucity of symptoms in the first decades of life may yet not have been diagnosed. In a recent Dutch study of 1158 adults with T21 living in residential centers, the prevalence of cardiac defects documented in the chart records was 16%, even lower than the reported number of 23% in our survey. 16 After performing an echocardiography in 138 adults without any known defect, 24 new cardiac lesions were detected. The majority of cardiac defects were valvular lesions, but EIGHT patients (7%) had shunt lesions (secundum atrial or partial atrioventricular septal defects, patent ductus arteriosus), requiring further evaluation and treatment. Taking these undiagnosed defects into account, the prevalence of cardiac defects in the Dutch study of adults with T21 rose by 40%. No such study has yet been performed in Switzerland, but it is also likely that Swiss adults with Down's syndrome have unrecognized congenital heart defects. One might consider a routine echocardiography in adult T21 patients with no previous cardiac evaluation, as offered to newborn children with Down's syndrome.
In patients with advanced pulmonary vasculopathy, selective pulmonary vasodilator therapies are recommended in pediatric and adult PAH guidelines,19,20 including combination therapies. None of the guidelines deny such treatment to T21 patients. In a recent multicenter study investigating the outcome of > 1000 ES patients from Europe and North America, two-third of patients were on selective pulmonary vasodilator therapies at the end of follow-up. 11 In this large survey, 30% of all ES patients had T21. A similar prevalence of T21 among ES patients was also observed in Germany (33%). 21 In the German National Register for congenital heart defects, 58% of patients with ES were treated with selective pulmonary vasodilators and their use was independently associated with better survival (HR = 0.44, 95% CI = 0.19–0.96). Treatment-naïve ES patients faced a 60–70% mortality at 10 years of follow-up. Similar to our study, there was no difference in survival observed between ES with and without T21.
Our study highlights the morbidity encountered in ES patients: paradoxical embolism; arrhythmias; or bleeding complications due to hemoptysis occurred in more than half of all ES patients. As in other GUCH patients, also in the SACHER ES patients with arrhythmias, the CHA2DS2-VASc score was not predictive of stroke events.22,23 However, the HAS-Bled score allowed to define a subgroup of patients with low bleeding risks, i.e. the ones with a score of 0. These findings need to be confirmed in a larger study cohort before they can be used to guide our decision on anticoagulation strategies in ES patients. In many ES patients, we face the dilemma of significant disease-related morbidity and mortality and missing evidence-based treatment pathways. Management based on expert opinions may be all we can offer to improve outcome. Therefore, referral of such complex patients to specialized GUCH centers is recommended.
Our study has several limitations. In the nationwide survey, the response rate was only 16%. We cannot exclude an important bias; physicians without adult T21 patients under their care may have had less interest to respond. In addition, some patients may have been reported twice by different practitioners. We could also not verify if they diagnostic criteria for ES were correctly applied in the survey patients. Assuming that the responding physicians are representative for the whole country, 4000–4500 adult T21 patients are expected to live in Switzerland, yielding a prevalence of 5–5.5/10,000 inhabitants. As comparison, a prevalence study in 2011 from England and Wales estimated 26,600 adult T21 patients among 56 million inhabitants, resulting in a prevalence of 4.8/10,000 inhabitants. 24 Our extrapolated prevalence is therefore comparable with other reports from Europe, supporting the credibility of our findings. Another limitation of this study is the small number of ES patients included in SACHER. Analyzing multiple predictors of outcome was only possible with statistical limitations. It is, however, reassuring to see that most of our observations are in line with reports from larger multicenter registries. It is likely that some of the reported T21 patients with heart defects in this survey were also included in SACHER. Due to the anonymous nature of the survey, no cross-linking was possible.
In conclusion, the prevalence of congenital heart disease in adult patients with T21 living in Switzerland is half the expected prevalence. In the past, these patients were undertreated or not timely diagnosed with congenital heart disease. As a consequence, adults with T21 and unrepaired congenital heart disease patients face increased morbidity and mortality. Raised awareness of potentially undiagnosed congenital defects in such patients and of the therapeutic options for T21 patients with ES is warranted.
Footnotes
Conflict of interest
The author(s) declare that there is no conflict of interest.
Funding
The mailing of the questionnaire to members of the “Schweizerische Gesellschaft für Allgemeinmedizin (SGAM)” and of the “Schweizerische Gesellschaft für Innere Medizin (SGIM)” was organized and financed by the pharmaceutical company Actelion Pharma Schweiz (Baden, Switzerland). Actelion Pharma Schweiz was at no time involved in the design and analysis of this study, nor in the drafting of this article. They had no access to the data.