
Abstract
Intravenous prostacyclin-based therapy improves survival in children with pulmonary arterial hypertension (PAH), but is typically administered via an external infusion pump, which places a considerable burden on the patient. Implanted pumps may overcome some of the limitations of external pumps. We describe the first long-term use of an implanted pump for intravenous treprostinil delivery in a pediatric patient with PAH. Our patient was experiencing marked dyspnea on exertion despite triple combination therapy with bosentan, sildenafil, and inhaled iloprost. Parenteral prostacyclin-based therapy was discussed and the patient rejected options involving external pumps; she finally chose intravenous treprostinil delivery via an implanted pump (LENUS Pro®; fixed flow rate; 20 ml reservoir). The patient underwent pump implantation in July 2012 (aged 14 years) under general anesthesia with no peri- or postoperative complications. She showed marked improvements in fatigue and dyspnea over the subsequent weeks, and her inhaled iloprost regimen was slowly decreased and stopped after six months. During follow-up, the pump showed an unexpected, progressive increase in flow rate that allowed a treprostinil dose of 170 ng/kg/min to be achieved, but at the cost of shortened intervals between refills. The pump was therefore replaced in August 2017 with a newer model with an adjustable flow rate (Siromedes®). A catheter dislocation was corrected under local anesthesia one week after the replacement surgery. The patient is currently receiving treprostinil 170 ng/kg/min with percutaneous refills every 12–13 days. Thus, implantable pumps might be a valuable alternative to external pumps for treprostinil infusion in pediatric PAH.
Keywords
Introduction
Pulmonary arterial hypertension (PAH) is a life-threatening disease characterized by obliteration of the pulmonary vascular bed and right heart failure. 1 Intravenous (i.v.) prostacyclin therapy improves survival in children with PAH,2–6 but prostacyclin analogs require continuous infusion. This is typically achieved by use of an external infusion pump, which places a considerable burden on the patients and is associated with adverse effects such as local site pain (subcutaneous infusion) 7 and catheter/bloodstream infections (i.v. infusion).8–11 Fully implantable pumps may overcome some of these limitations. Studies in adult patients with pulmonary hypertension have demonstrated the feasibility of continuous i.v. treprostinil infusion via fully implantable pumps such as the gas-driven LENUS Pro® pump (Tricumed, Kiel, Germany),12–16 but to our knowledge, this approach has not yet been used in pediatric patients with PAH.
The LENUS Pro® pump is implanted in the upper abdominal wall and is connected to a tunneled catheter that ends at the entrance to the right atrium. The drug reservoir is refilled percutaneously via a silicon septum. Intervals between refills are 10–30 days, depending on the reservoir size (20 ml or 40 ml) and pump flow rate (which is fixed in the LENUS Pro® pump but adjustable in a newer battery-driven model (Siromedes®, Tricumed)). We describe the first implantation and long-term use of a fully implantable pump for i.v. delivery of treprostinil in a pediatric patient with PAH.
Case description
We report on a female patient who is now 19 years old. Written consent was obtained from the patient herself as she had already reached adulthood at the time the report was written. However, permission from the Research Ethics board was also obtained at the time of pump implantation, as this was a new therapeutic approach in children (approval number: BB 36/11). The patient underwent annual echocardiographic evaluation during her childhood because of a family history of pulmonary hypertension. Genetic testing was not performed because of the low penetrance of the genetic variations known to be associated with the onset of pulmonary hypertension. Following detection of an increase in her right ventricular pressure in 2008 (when the patient was 10 years old), she underwent right heart catheterization that revealed an invasively measured mean pulmonary arterial pressure (PAP) of 37 mmHg. She was diagnosed with hereditary idiopathic PAH. After a negative pulmonary vasoreactivity test, she began upfront combination therapy with bosentan (62.5 mg twice daily) and sildenafil (20 mg three times daily) at an external pediatric heart center.
Since April 2009, the patient has been followed in close cooperation with the Center for Transplantation (German Heart Center, Berlin, Germany) as well as the Center for Congenital Heart Disease (EMAH, Ernst-Moritz-Arndt University, Greifswald, Germany) at our own outpatient clinic (Ernst-Moritz-Arndt University, Greifswald, Germany) with evaluation of parameters including peak oxygen uptake (VO2), N-terminal pro-brain natriuretic peptide (NT-proBNP), and noninvasively measured systolic PAP (Fig. 1(a)). At the first encounter in our clinic after diagnosis, the patient was in functional class II and showed stable values in transthoracic echocardiography, but her quality of life was markedly limited by dyspnea under exertion during daily activities. In March 2010, inhaled iloprost (7.5 µg six times daily via an I-Neb® nebulizer (Philips Healthcare, Hamburg, Germany)) was initiated as add-on therapy. Over the following two years, her clinical course appeared stable, but from April 2011 her everyday life was affected by marked dyspnea under exertion, and in July 2011 the doses of bosentan and sildenafil were increased to 125 mg twice daily and 40 mg three times daily, respectively. The relatively high dosage of sildenafil did not follow the contemporary recommendations for PAH in pediatrics, but was an experimental approach that was later supported by the oral Sildenafil in Treatment-Naive Children, Aged 1 to 17 Years, With Pulmonary Arterial Hypertension (STARTS) trial publication, which stated that the dose of 40 mg three times daily was to be favored in children weighing more than 45 kg.
17
This experimental approach was taken considering the dramatic disease progression of the patient, to extend as much as possible the time to lung transplantation. An additional consideration was the fact that sildenafil and bosentan show a pharmacokinetic interaction leading to a decrease in the maximum plasma concentration of sildenafil.18,19
Treprostinil infusion via an implanted pump in pediatric pulmonary arterial hypertension. (a) Peak oxygen uptake (VO2), noninvasively measured systolic pulmonary arterial pressure (PAP), and N-terminal pro-brain natriuretic peptide (NT-proBNP) before and after first pump implantation. (b) Pump flow rate and treprostinil dose over time. (c) Pump replacement surgery and (d) diagram showing positions of first and second pumps and catheters. i.v.: intravenous.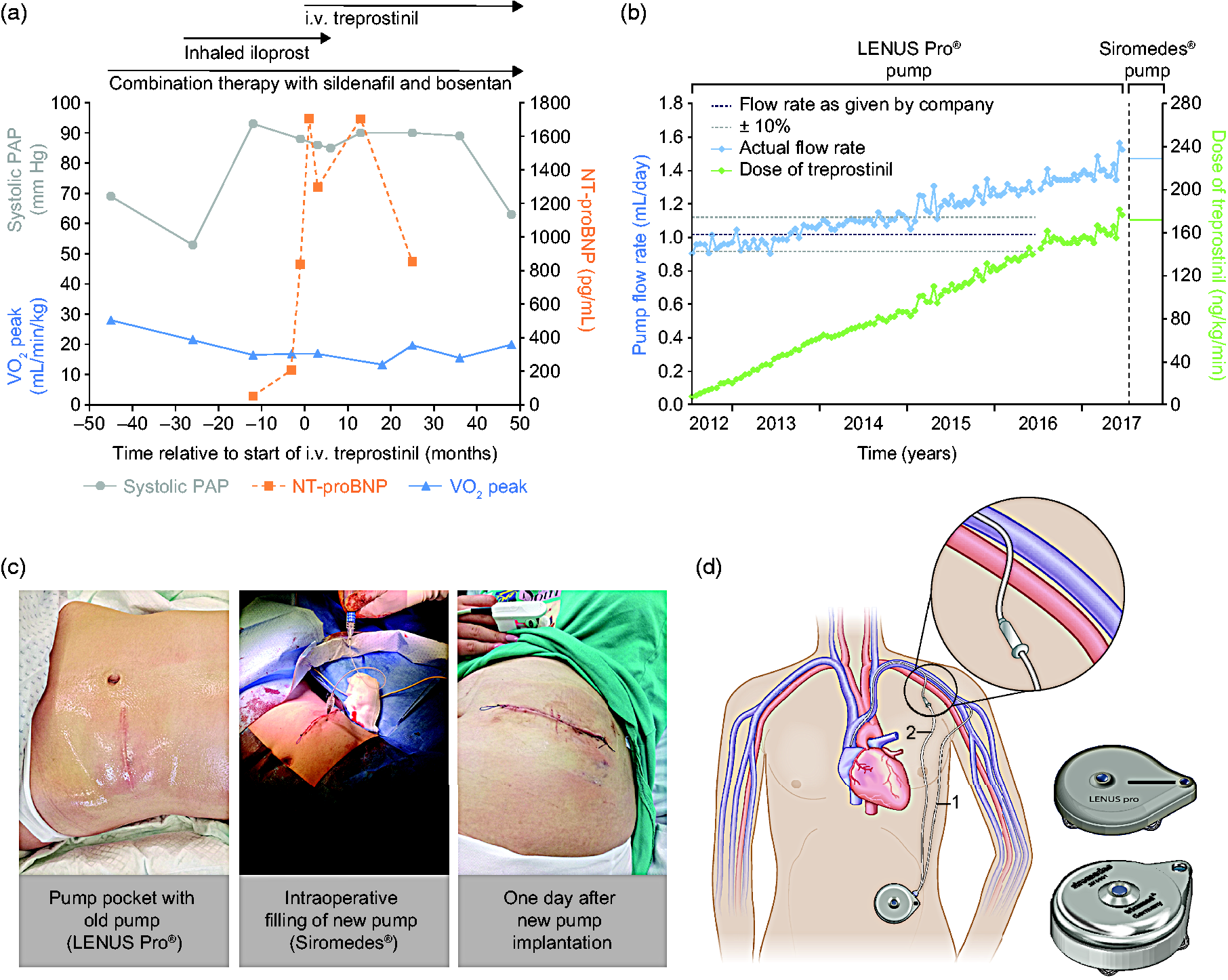
In 2012, after consultation with several German specialized centers for second opinions and after the patient showed a reduction in exercise capability paralleled by a marked increase in NT-proBNP, transition from inhaled to parenteral prostacyclin-based therapy was discussed. Subcutaneous administration and implantation of a Hickman catheter or port-a-cath system for i.v. administration were rejected by the patient because of the possible side effects and complications. Finally, the patient opted for i.v. delivery of treprostinil via a fully implantable pump (LENUS Pro®, Tricumed; 20 ml reservoir).
The pump was implanted under general anesthesia in July 2012, when the patient was 14 years old. Treprostinil was started one day before implantation (administered through a peripheral vein and titrated up to 6 ng/kg/min) and was well tolerated. The pump was implanted in the abdominal pocket with a subcutaneous catheter to the vena cephalica sinistra; there were no peri- or postoperative complications. Initially, the pump was refilled with an increasing concentration of treprostinil every 16–19 days. The patient experienced a marked improvement of her fatigue and dyspnea in the first weeks after starting i.v. treprostinil. The multiple iloprost inhalations per day were slowly decreased and stopped after six months; the young patient considered this an important improvement in her quality of life.
Unexpectedly, the flow rate of the pump progressively increased during follow-up (Fig. 1(b)), resulting in shortened intervals between refills. The increase was not accompanied by treprostinil-related side effects, possibly because of the very gradual nature of the increase. A potential cause of this unexpected increase is the possible interaction between treprostinil and the glass capillary of the pump, causing an increase in the cross-section of the capillary canal and therefore an augmentation of flow by 10%, as declared by the Tricumed company after extensive research. This increase of the capillary canal cross-section is a slow process that occurs over several years. 21 Owing to the increased flow rate in our case, a dose of 170 ng/kg/min was achieved with the highest available concentration of treprostinil solution (10 mg/ml). However, to increase the dose further would have depended on further increases in flow rate and shortening of refill intervals. Therefore, we decided together with the patient to implant a new 20 ml pump with an adjustable flow rate of 0.25–3.0 ml/day (Siromedes®, Tricumed).
The pump replacement surgery was performed in August 2017 without complications (Fig. 1c and d). First, the former pump was removed and the new pump was brought into position. The distal catheter ending was reused. Radiological imaging after the intervention showed that the pump was correctly positioned, but the tip of the catheter was lying approximately in the subclavian vein. Adjustment of the catheter was discussed with the patient, who decided against immediate correction of the catheter position despite the possible risks. As there was no sign of catheter malposition or dislocation at that time, we accepted the modified position. However, a few days later the patient presented at the nearest hospital with pain and swelling of the left shoulder and adjacent thoracic region. Radiological imaging showed dislocation of the catheter, resulting in local dermal irritation due to treprostinil extravasation. There was no vessel perforation. We corrected the dislocation surgically under local anesthesia one week after the pump replacement. The catheter was extracted and a new one positioned with direct puncture of the vena subclavia sinistra (Fig. 1(d)). Fluoroscopy confirmed the correct positioning of the new catheter. After catheter replacement the vein was patent and the symptoms resolved completely.
A hematoma at the pump pocket required puncture and needle aspiration 13 days and 22 days after the pump replacement, with drainage of 100 ml and 80 ml of fluid, respectively. Subsequent refills were performed every 12–13 days without adverse events. The new pump currently has a flow rate of 1.47 ml/day, delivering a dose of 170 ng/kg/min. The patient has now overcome her initial doubts regarding lung transplantation and has agreed to be evaluated for future transplantation.
Discussion
We have reported our first long-term experience of using a fully implantable pump for i.v. treprostinil infusion in a pediatric patient with PAH. The patient showed clinical improvement after initiating i.v. treprostinil on top of background combination therapy, consistent with previous studies in which children with PAH receiving i.v. prostacyclin showed improvements from baseline in pulmonary hemodynamics and/or functional capacity.2–6
Our patient had no infections associated with the implanted system. Studies of fully implantable pumps in adults with PAH have also shown no catheter-related bloodstream infections.12,14,15 By contrast, i.v. therapies administered via external pumps have a well-documented risk of catheter-related bloodstream infections. 8 For example, incidences of 0.25–0.54 and 0.19–1.95 per 1000 catheter-days have been reported in pediatric patients receiving i.v. prostacyclin and treprostinil, respectively.21,22
In our patient, the LENUS Pro® pump showed an increase in flow rate, leading to a substantial increase in the treprostinil dose. This dose increase was well tolerated and may have helped to stabilize the clinical course of the patient, allowing her to lead a full life with participation in most of the usual social activities of adolescents. However, given the limitations of the maximum treprostinil concentration, the reservoir size, the frequent refills, and the unknown cause and uncontrollable nature of the increase in flow rate, a decision was made to replace the LENUS Pro® pump with the Siromedes® pump.
Although the second pump implantation itself was well tolerated, catheter dislocation occurred that required surgical revision. Catheter dislocations requiring surgical revision have also been reported in adult patients with PAH treated via fully implantable pumps (3/30 patients in a European study 14 and 3/60 US-based patients (0.14 cases per 1000 patient-days)),12,15 and in pediatric patients with PAH treated via external pumps (0.32 cases per 1000 catheter-days). 21 The reason for the catheter migration and subsequent dislocation in the current case is uncertain. Owing to the physical maturity of the patient at the time of the first pump implantation (her weight did not change and her height increased by only 1 cm between the first implantation and the time of writing), the likelihood of her outgrowing the catheter is considered negligible, but additional radiological imaging before the second pump implantation (which would have allowed us to exclude this possibility) was not performed. The proximity in time of the catheter dislocation to the pump replacement suggests an acute event during the surgical procedure (e.g. inadvertent traction on the line) as the most likely cause. As a result of this episode, we are now adopting radiological assessment of the position of the catheter tip as a standard procedure before pump replacement. Further standardization of the implantation procedure may help to reduce the occurrence of such events. Our patient also developed a hematoma at the pump pocket; hematomas/seromas have been observed previously in adult patients following pump implantation and are usually minor and easily treated with local compression/cooling or with puncture and needle aspiration.12,14,15
As a 14-year-old girl, our patient was almost fully grown, weighing 57 kg with a height of 167 cm. Almost six years later, at the time of writing this report, the girl was 19 years old and still weighed 57 kg with a height of 168 cm. In our case, the decision to use an implantable pump was facilitated by the physical constitution and maturity of the patient. Additionally, at the time of pump implantation, the therapeutic options that were acceptable to the patient were limited. The continuous delivery of treprostinil was the most promising possibility to delay the inevitable lung transplantation, and the risk-to-need ratio was therefore in favor of the experimental approach in this case.
In smaller children, the use of a fully implantable pump must be regarded more critically because of the body-to-pump volume ratio. Owing to the increasing flow rates required during progression of the disease and as the child grows, switching to a larger reservoir will become inevitable as time passes. However, this outgrowing of the reservoir is to be expected only in smaller children. Higher numbers of complications are also to be expected in smaller children.23,24 Further data are needed to assess the limitations of treprostinil infusion via a fully implantable pump in smaller infants.
To summarize, we show for the first time that fully implantable pumps might be a valuable alternative to external pumps for i.v. treprostinil infusion as a bridge to lung transplantation in pediatric patients with PAH. Similar to adult patients, pediatric patients could benefit from the long refilling intervals, improved quality of life, and reduced infectious complications and site pain compared with traditional external pump systems. However, it must be noted that our patient was almost fully grown at the time of pump implantation; therefore, this case report does not provide information on the potential complications of this approach in small children who are still growing.
Footnotes
Conflict of interest
Dr Richter has received support from United Therapeutics and Bayer Pharma AG, and speaker fees from Actelion, Bayer Pharma AG, Mundipharma, Roche, and OMT, outside the submitted work. Dr Ewert has received speaker fees and fees for participation in advisory boards from United Therapeutics, OMT, Pfizer, GlaxoSmithKline (GSK), Actelion, Novartis, Bayer HealthCare, and Encysive/Pfizer; grants from Actelion and Boehringer Ingelheim; and publication support and industry-sponsored grants from OMT, outside the submitted work. The other authors have nothing to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.