
Abstract
Macrophage migration inhibitory factor (MIF) and 22 a priori selected biomarkers were measured from pulmonary arterial hypertension (PAH) patients. Significant positive correlations were found between MIF and several angiogenic factors suggesting a possible MIF regulation role in PAH angiogenesis and pathobiology, but simultaneously highlighting the biomarkers profiling complexity in PAH.
Introduction
Chronic inflammation contributes to endothelial dysfunction and the development of pulmonary arterial hypertension (PAH). 1 Implicated in the pathogenesis of PAH are endothelial-derived angiocrine and circulating pro-angiogenic factors which promote repopulating cells (e.g. endothelial cells in the case of PAH) in an organized functional way. The interaction between inflammation, angiogenic factors and pulmonary vascular disease has been well established.2–4
Macrophage migration inhibitory factor (MIF) is a pleiotropic cytokine that is ubiquitously expressed in many cell types including the endothelium and several types of immune-related cells, including macrophages and T-cells, playing a significant role in regulation of innate immunity. This cytokine is constitutively expressed in macrophages and other innate immune cells, rapidly upregulating the production of inflammatory cytokines in the presence pathogen. 5 Furthermore, it has been shown that the release of this cytokine promotes recruitment and transmigration of additional leukocytes to sites of injury. 6 Recently, elevated MIF plasma concentrations7,8 and over-expression of the MIF receptor CD74 in the pulmonary endothelium of PAH patients have been reported.8,9 Pharmacologic antagonism of MIF inhibits hypoxia-induced smooth cell proliferation, 10 and partially reverses the development of PAH in an experimental rat model. 9 In similar rat models, the influx of inflammatory cells and cytokines has been found to precede the development of vascular remodeling, and the phenotype of pulmonary hypertension (PH) is avoided altogether when depleting activated macrophages from these animals, suggesting that pro-inflammatory mechanisms lead to this maladaptive process. 1 As such, it could be assumed that MIF may play a role in promoting the inflammatory milieu seen in patients with PAH. In addition to MIF’s pro-inflammatory properties, MIF can also upregulate angiocrine and angiogenic growth factors, such as vascular endothelial growth factor (VEGF) and it has been demonstrated to have a proangiogenic effect, particularly in studies of tumorigenesis. 11 A pro-angiogenic role for MIF has not been identified in PAH. 12 We hypothesized that MIF and several angiogenic biomarkers are tightly interrelated in participants with PAH.
Methods
This is a secondary analysis of a prospective cohort study, the FREEDOM C-2 trial. 13 Most FREEDOM C-2 participants had either idiopathic PAH (IPAH) or connective-tissue disease associated PAH (CTD-PAH), and per trial protocol randomly received either oral treprostinil or placebo in addition to their baseline PAH therapy. Study participants consented to have blood drawn and banked in an anonymized biorepository. Concentrations of pre-specified biomarkers, including MIF, were assessed in EDTA plasma samples using multiplexed immunoassay (DiscoveryMAP® v. 3.0 assay, Myriad RBM, Inc., Austin, TX, USA).
For the current study, MIF and 22 known angiogenic biomarkers were selected a priori for analysis. Descriptive statistics were performed comparing these biomarkers in relationship to IPAH and CTD-PAH at baseline and at the conclusion of the trial 16 weeks later.
Spearman’s correlation method was used to assess associations between MIF and the other biomarkers, as well as with clinical characteristics such as participants’ functional class, BORG dyspnea score, and baseline 6-minute walk distance (6MWD). Both linear and logistic regression models were performed to identify relationships between plasma MIF concentrations and relevant clinical measures, such as change in 6MWD, or a composite clinical outcome (as defined by the original trial protocol 13 ) over the course of the treatment period.
Results
Of the 310 people who participated in FREEDOM-C2, 178 patients (76% women; 63% Caucasian; mean age = 51 ± 15 years) consented to blood-banking and had baseline MIF levels measured. The majority (62% of all participants) had either idiopathic or hereditary forms of PAH, with the CTD-PAH accounting for 35% of the population. Most participants were on a PDE-5 inhibitor (85%) and had a baseline 6MWD of 333 ± 70 m. The mean BORG dyspnea score was 3.8 ± 2.4. The mean baseline MIF level was 1.8 ± 3.2 ng/mL.
At baseline and at 16 weeks, several biomarkers were higher in the IPAH group compared with the CTD-PAH group. Specifically, at baseline the following biomarkers were higher in IPAH than in CTD-PAH patients: growth/differentiation factor-15 (1.2 versus 0.8 ng/mL; P < 0.001), interleukin-6 (IL-6) (6.2 versus 3.0 pg/mL; P = 0.001), placenta growth factor (PLGF) (19.1 versus 14.4 pg/mL; P = 0.008), stem cell factor (SCF) (329 versus 261 pg/mL; P < 0.001), thrombomodulin (4.6 versus 3.8 ng/mL; P =0.009), vascular endothelial growth factor (VEGF) (67.3 versus 56.8 pg/mL; P = 0.012), and VEGF-D (317 versus 266 pg/mL; P = 0.019). At 16 weeks, MIF was also significantly elevated in the IPAH compared with the CTD-PAH group (3.1 versus 2.3 ng/mL; P = 0.035).
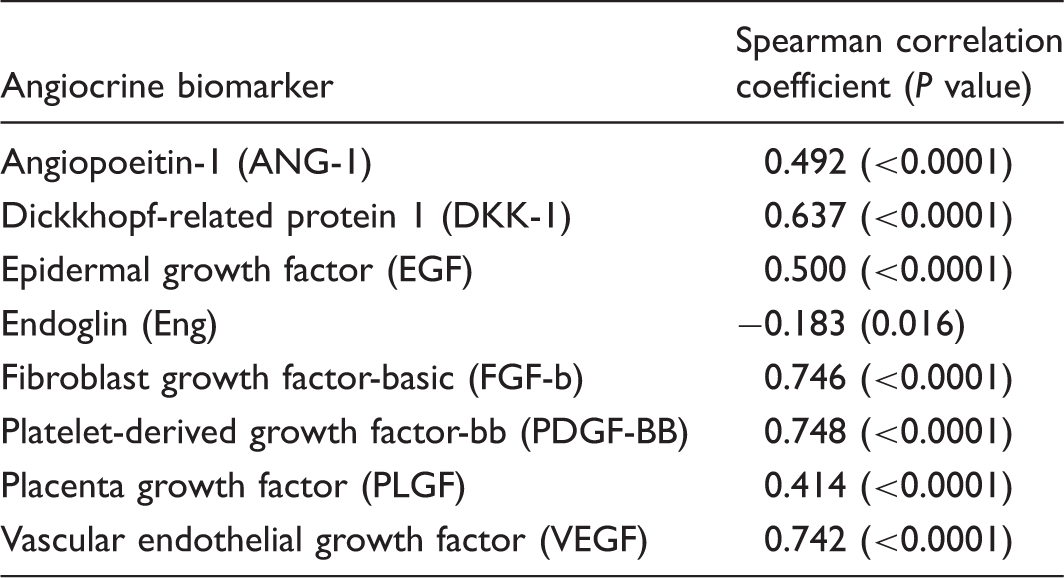
MIF concentrations correlate with angiogenic factors.
Discussion
Although prior investigations have identified important relationships between angiogenic growth factors and the development of PH,10,12 the current study establishes associations between circulating concentrations of specific angiogenic factors and MIF, while highlighting the complexity of biomarkers profiling in PAH. MIF is strongly correlated with well-known angiogenic factors implicated in PAH, including Angiopoietin 1 and VEGF. We also identify a relationship with MIF and other factors implicated in endothelial proliferation and PAH. Each of the following biomarkers, PDGF-BB, basic FGF-basic, EGF, PLGF, and Endoglin, have been independently found to play a role in PH;14–20 and DKK-1 is known to regulate angiogenesis in tumor cell proliferation. 21
Because MIF has been shown to upregulate angiogenic growth factors, MIF may play a role in the regulation of angiogenesis, and as such, its dysregulation may be a factor in the development of PAH. 22 The exact role with which MIF interacts with these various biomarkers, however, needs further investigation. Future studies will aim to further characterize the mechanisms underpinning these associations using in vitro models of human pulmonary endothelial cells, and in animal models of conditional MIF knock-outs in various inflammatory and hypoxic conditions known to promote the development of PH. A recent report showed a moderate correlation between MIF and relevant hemodynamic parameters in portopulmonary hypertension, 7 which further supports the role of MIF in different PAH subgroups. Unfortunately, this study did not find an association between clinical outcomes (such as 6MWD or rates of clinical decompensation) and plasma concentrations of MIF, though this may be a function of study design and not adequately powered sample size.
The current results emphasize the difficulty of studying network-based interactions of different proteins in a single -omics “layer” (proteomics in this case), and it would be overly simplistic to place too much weight on any one biomarker in the development of a complex disease state such as PAH. We hope to illustrate that there is evidence to add another component to the expanding spectrum of disease-promoting factors in the development of this illness, though the initiating or driving forces for these myriad biomarkers interactions are unclear, and these complex interactions need to be considered when evaluating the angiogenic activity in PAH. A profile-based approach, rather than one or a handful of proteins-based approach, would be a more accurate characterization of a PAH profile. Adding another -omic layer (e.g. metabolomics or genomics)23,24 to such analyses to account for the variability in the different biomarkers even when they move in the same direction would further enhance our understanding of PAH pathobiology. As such, future approaches to studying this question will need to be varied, with a continued focus on the linear mechanisms, as well as larger network-based approaches using a combination of proteomic and genomic profiling in both murine models and human participants with PAH.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.