
Abstract
Adult-onset Still’s disease (AOSD) is an inflammatory disorder characterized by recurrent fevers, arthralgia, leukocytosis, and a salmon-colored rash. Diagnosis is made based on the Yamaguchi criteria. Various cardiac and pulmonary manifestations have been described in association with AOSD, including acute respiratory distress syndrome (ARDS) and pulmonary arterial hypertension (PAH). We describe the first case of both PAH and ARDS in a patient with AOSD who, despite aggressive therapy, declined rapidly and ultimately died. There was concern for pulmonary veno-occlusive disease given the rate of her decompensation, but this was found not to be the case on autopsy. Treatment of AOSD with cardiopulmonary involvement requires rapid identification of AOSD followed by aggressive immunosuppression.
Keywords
Introduction
Adult-onset Still’s disease (AOSD) is an inflammatory disorder characterized by recurrent fevers, arthralgia, leukocytosis, and a salmon-colored rash. Diagnosis is made based on the Yamaguchi criteria. 1 Various cardiac and pulmonary manifestations have been described in association with AOSD, including acute respiratory distress syndrome (ARDS) and pulmonary arterial hypertension (PAH).2–5 We present a case of a young woman who developed PAH and ARDS as a consequence of her AOSD, where her clinical course was initially concerning for pulmonary veno-occlusive disease (PVOD), which was ruled out on autopsy.
Case presentation
A 31-year-old African American woman presented with a two-week history of rapidly progressive shortness of breath on exertion and leg swelling. Prior to her presentation, she could complete activities of daily living without any difficulty but experienced dyspnea while climbing stairs and lifting heavy objects for the last year. Despite multiple hospitalizations for these issues at an outside community institution, an etiology for these symptoms was never fully evaluated or determined. The patient was diagnosed with AOSD at the age of 24 years and had previously been managed with various immunosuppressive therapies including prednisone and mycophenolate mofetil. Upon presentation to our institution, she was receiving prednisone and methotrexate for the management of her AOSD symptoms and was prescribed trimethoprim-sulfamethoxazole for prophylaxis. Physical examination was notable for hyperpigmented macules of the bilateral upper arms, lower extremity pitting edema, distended jugular venous pulse with accentuated hepatojugular reflex, and a loud P2 on cardiac auscultation.
Her chest radiograph (CXR) is shown in Fig. 1. A transthoracic echocardiogram showed normal left ventricular size and function with an ejection fraction of 55–60%, severe enlargement of the right ventricle and atrium, flattening of the interventricular septum in systole and diastole, and severe tricuspid regurgitation (Fig. 2). Right ventricular systolic pressure was estimated at 70–80 mmHg and there was evidence of a small pericardial effusion. A non-contrasted CT of the chest on admission revealed extensive mediastinal and hilar lymphadenopathy with some axillary lymphadenopathy, an enlarged pulmonary artery of approximately 39 mm, and extensive mosaic attenuation throughout the bilateral lungs (Fig. 3) with no evidence of pulmonary embolism.
CXR on day of admission showing clear lung fields, cardiomegaly, and a slightly widened mediastinum. Apical four-chamber view showing right atrial and ventricle dilation and a small pericardial effusion. Chest CT without contrast performed on day of admission showing evidence of mild bilateral mosaic attenuation throughout the lungs.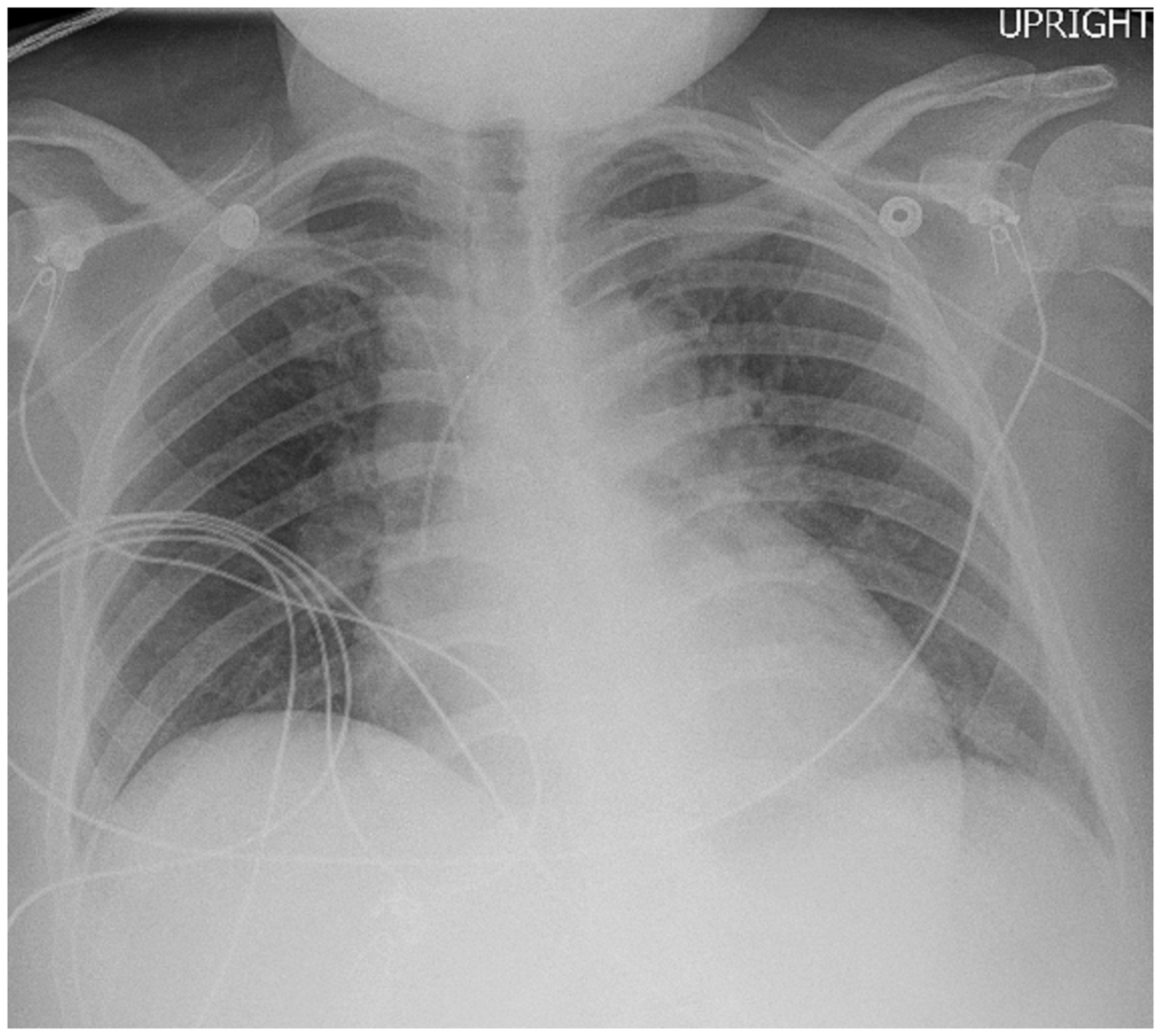


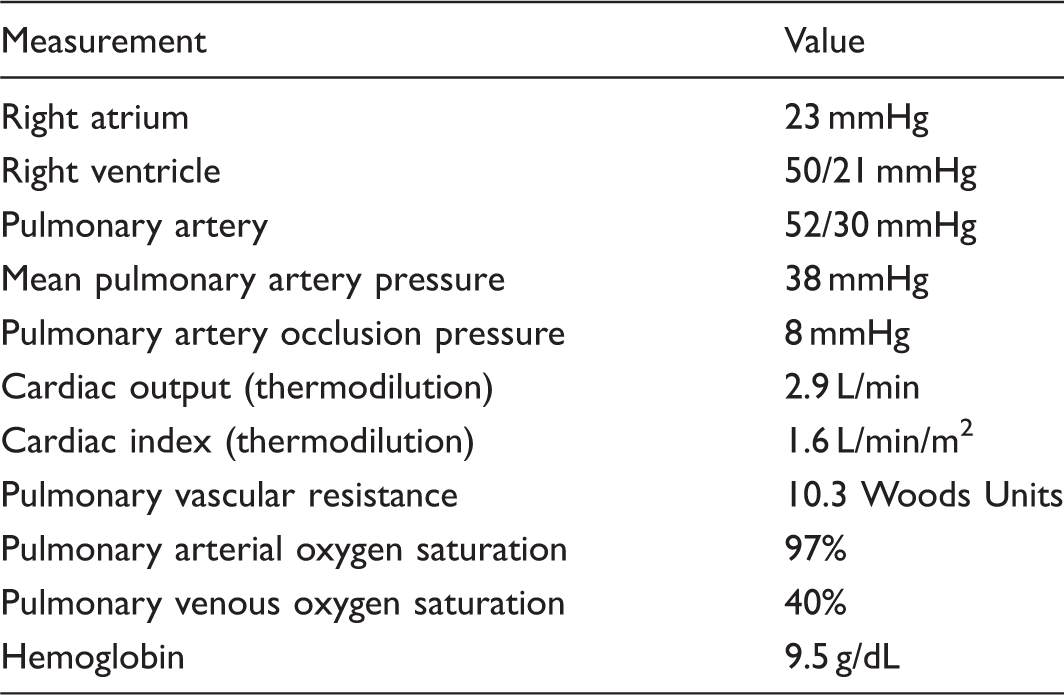
Right heart catheterization.
Over the subsequent three days, the patient began to decline, exhibiting symptoms of right ventricular failure. Inhaled epoprostenol at 50 ng/kg/min was initiated and epoprostenol infusion was gradually increased to a rate of 8 ng/kg/min. Despite this, she exhibited worsening hypoxia on serial arterial blood gas measurements despite increasing her inhaled FiO2. Due to her hemodynamic instability, the patient was worked up for an infectious etiology and broad-spectrum antimicrobial coverage was initiated.
Despite these interventions, the patient continued to deteriorate. She ultimately required endotracheal intubation and mechanical ventilation due to her worsening hypoxia (desaturations as low as 70% on 100% inhaled FiO2 non-rebreather mask) in conjunction with tachycardia to 160 beats per minute. Her lactic acidosis returned as well, peaking at 3.6 mmol/L. Complete blood count revealed a worsening leukocytosis 24.9 thou/cu mm with 15% bands. The patient’s CXR prior to intubation (Fig. 4) and clinical picture at the time of this decompensation was consistent with ARDS. Shortly after intubation, the patient experienced pulseless electrical activity and despite advanced cardiovascular life support she ultimately died. The rapid decline after initiating pulmonary arterial hypertension therapy was concerning for possible underlying pulmonary veno-occlusive disease (PVOD) or pulmonary capillary hemagiomatosis (PCH). Additionally, her rapid decline precluded the possibility of any repeat imaging or advanced monitoring of cardiac output.
CXR three days after admission revealing diffuse bilateral infiltrates.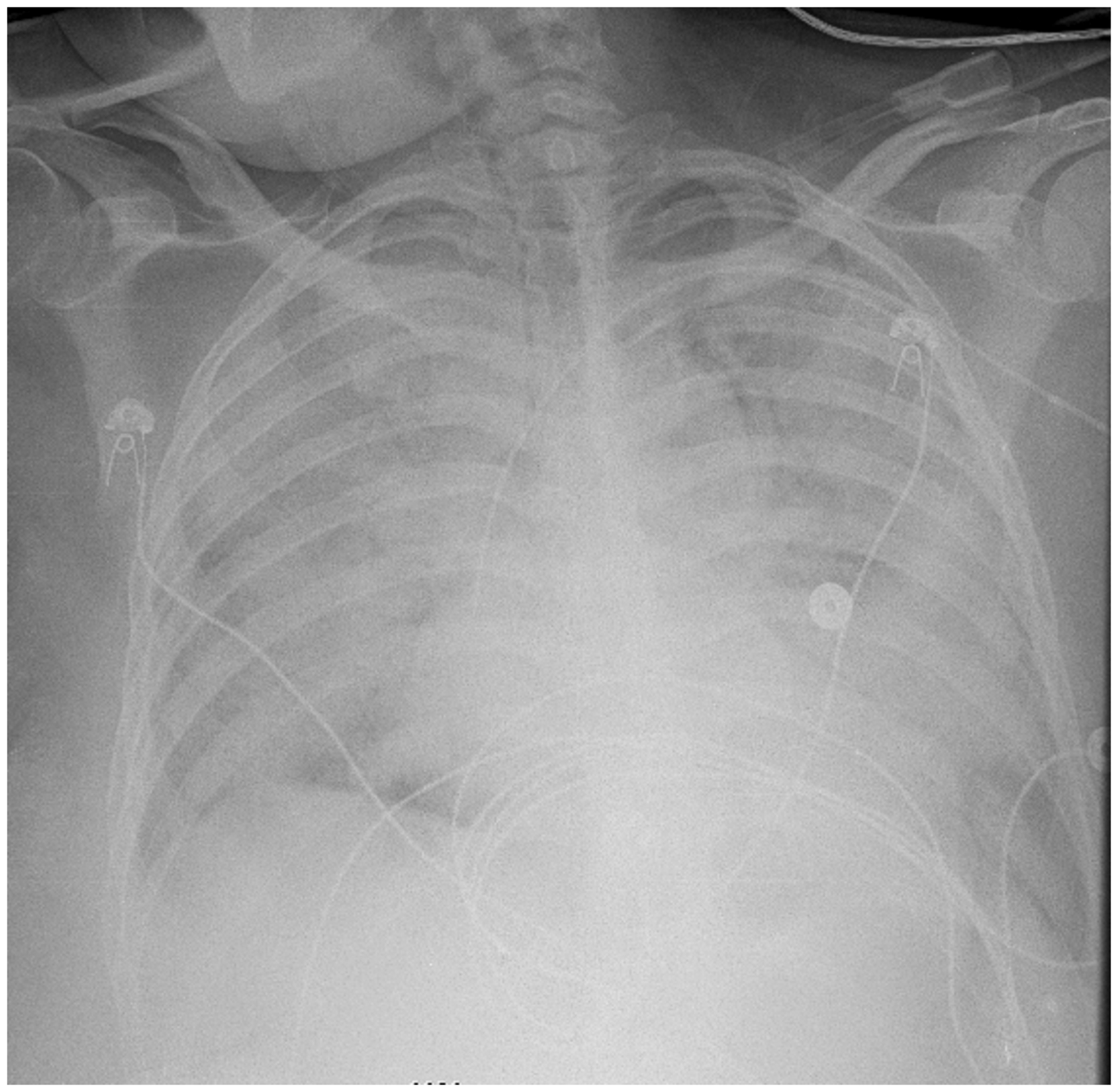
Autopsy revealed right ventricular hypertrophy and moderately dilated right ventricle and right atrium. Additionally, the patient’s lungs were significant for diffuse alveolar damage with prominent hyaline membrane formation with edema and a prominent neutrophilic alveolar infiltrate. There was both intimal thickening of the pulmonary arteries and arterioles (Fig. 5). Features suggestive of the presence of PVOD and PCH were not present on pathological examination. Pathology slides were sent out for a second opinion that confirmed the initial report. Regardless, all cultures and staining performed on lung samples did not identify any infectious organisms. The final diagnosis was PAH and ARDS in the setting of AOSD. Considering the right ventricular hypertrophy present on autopsy and her report of dyspnea on exertion for the year prior to her decompensation, it is likely the patient’s PAH had been present for some time and not recognized during her previous hospitalizations.
Pulmonary histology showing evidence of pulmonary arteriole intimal thickening (blue arrow) and hypertrophy as well as prominent alveolar edema and neutrophilic alveolar infiltrate (red arrow).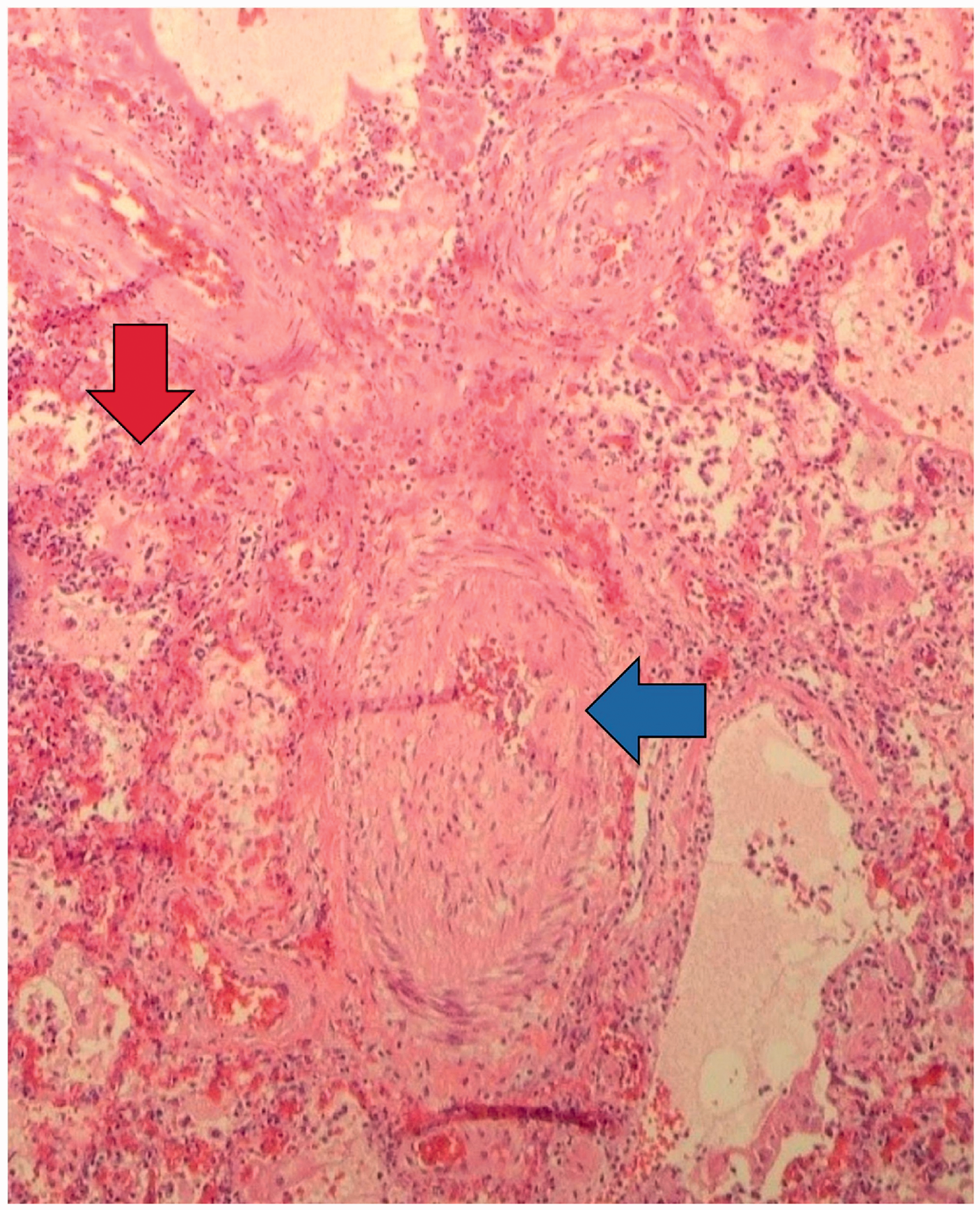
Discussion
Cases of AOSD and PAH.
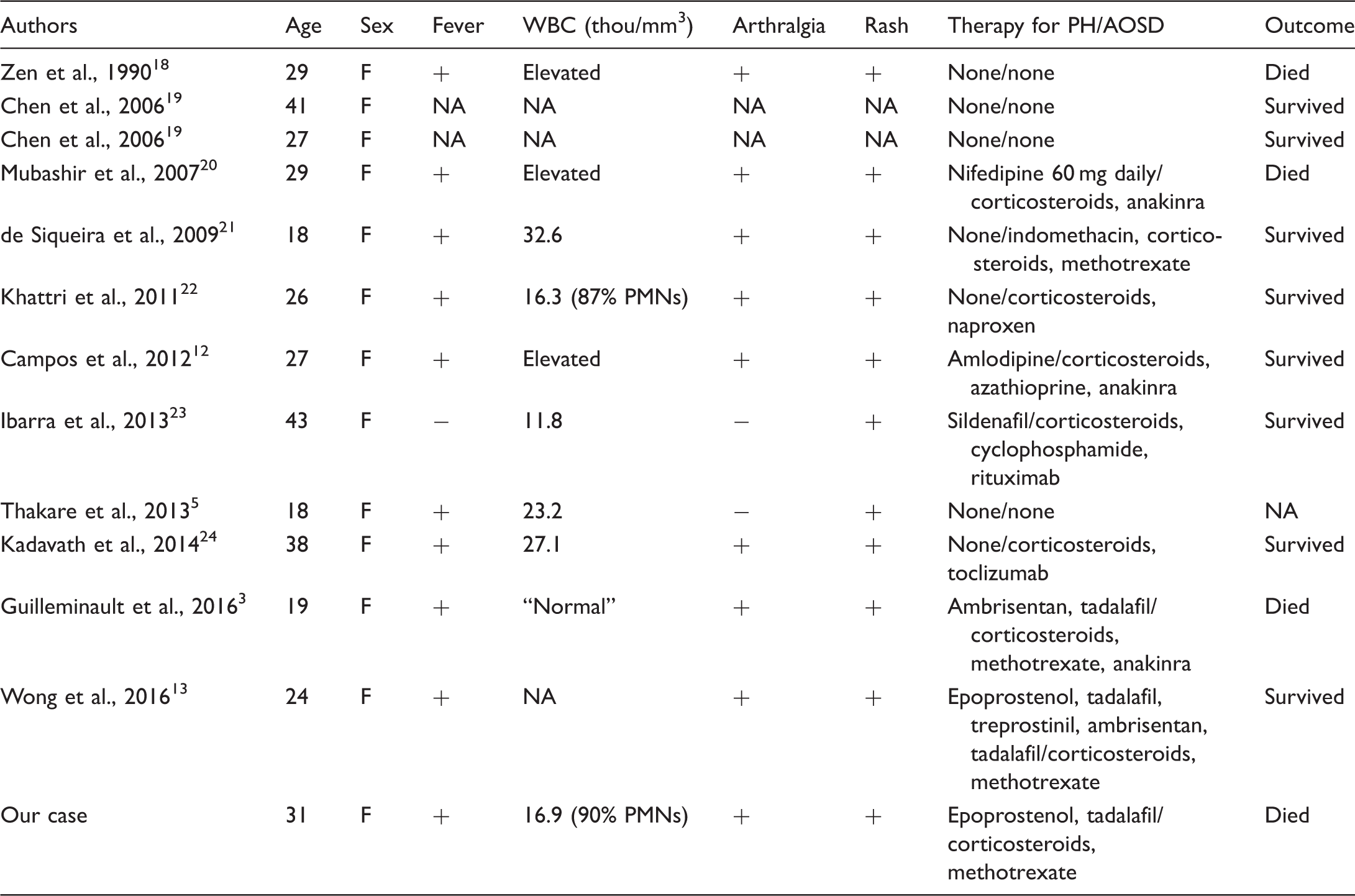
F, female; +, present; −, not present; NA, not available.
Although the mortality in AOSD is low, 10 it increases dramatically in cases where the disease is complicated by cardiopulmonary abnormalities. 11 PAH and ARDS are rare complications of AOSD. We report the first case where both complications occurred in a patient with AOSD. The presence of mediastinal adenopathy on chest imaging and the patient’s clinical decline after initiation of PAH-specific therapy was concerning for PVOD/PCH. However, autopsy failed to show evidence suggestive of either. To date, there have been no cases of PVOD/PCH reported in association with AOSD.
The exact pathophysiology of AOSD is unknown, but much of the disease seems to involve macrophage and neutrophil activation. Furthermore, therapy for AOSD can involve inhibition of IL-1, IL-18, and TNFα, implicating their role in the disease.12–14 With regards to PAH, there is a consensus that dysregulation of these cytokines plays a role in the remodeling of the pulmonary vasculature via recruiting of inflammatory cells. It seems reasonable to conclude that this similarity between AOSD and PAH could represent a reasonable mechanism for the pathophysiology of the disease; however, more research is necessary.
The mainstay of treatment of AOSD involves immunosuppression. Specifically, inhibition of IL-1 with anakinra has been associated with improved outcomes in AOSD and PAH.12,14 In this case, the patient was continued on her prior immunosuppressive regimen for AOSD. Escalation of her immunosuppressive therapy was considered; however, due to her rapid hemodynamic decline and the possibility of an infectious etiology, we decided the benefit did not outweigh the risk at that time. Furthermore, the choice was made to prioritize treatment of the patient’s right-sided heart failure as a consequence of her PAH given her rapidly progressing hemodynamic instability and eventual hypoxic respiratory failure.
Cases of AOSD and ARDS.
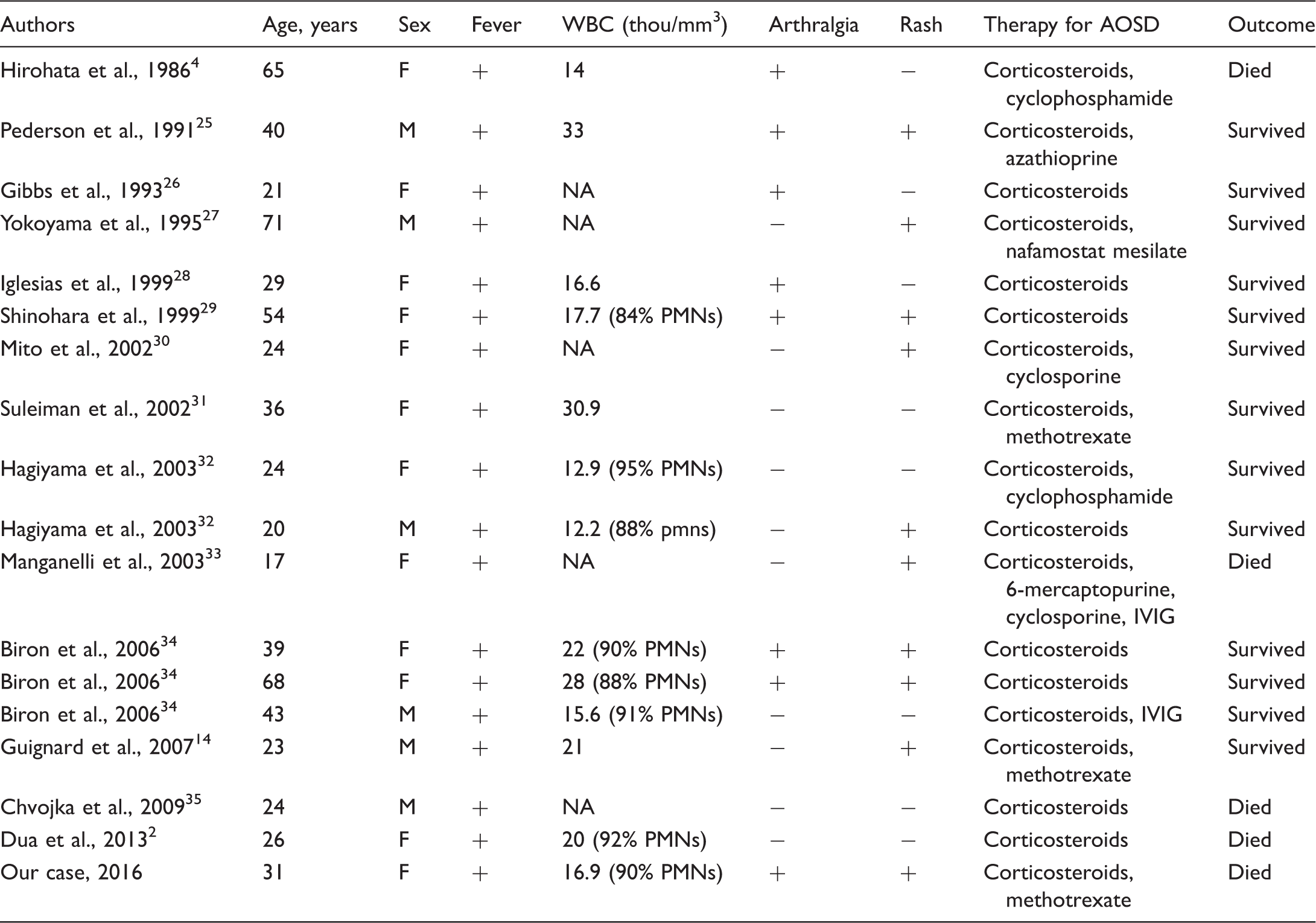
F, female; M, male; +, present; −, not present; NA, not available.
What is not clear is why, exactly, ARDS and PAH tends to be so fulminant in cases of AOSD. It has been noted that any pulmonary complication has been associated with a poorer outcome and our patient experienced two concomitant severe pulmonary complications. 11 Considering the pathophysiology of extremely rapid decline is unclear, it perhaps highlights avenues for further research to elucidate a mechanism beyond that of the release of cytokines.
As in our case, patients with AOSD are frequently empirically treated with broad-spectrum antimicrobial therapy, but tend to ultimately be transitioned to aggressive immunosuppression. Our case differs in that the patient’s clinical status was more fulminant given her severe right heart failure due to PAH. This precluded the possibility of definitively excluding infectious etiologies and allowing for adequate and timely treatment with immunosuppression.
Conclusion
We describe the first case of both PAH and ARDS in a patient with AOSD who, despite aggressive therapy, declined rapidly and ultimately died. Treatment of AOSD with cardiopulmonary involvement requires rapid identification of AOSD as the etiology for decompensation followed by aggressive immunosuppression. Considering this, we recommend early involvement of rheumatology specialists in cases where patients present with new onset respiratory failure with a history of rheumatologic disease in which pulmonary hypertension is in the differential diagnosis. This case also highlights how the concomitant presentation of these two conditions may be mimicking the clinical presentation of PVOD or PCH. No standard of care for the management of these conditions currently exist.
Footnotes
Conflict of interest
The author(s) declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.