
Abstract
Pulmonary arterial hypertension (PAH) is a progressive potentially fatal disease. Multiple pharmacologic options are now available, which facilitated transitions between different therapeutic options, although the evidence for such transitions has not been well described. We sought to review the evidence supporting the safety and/or efficacy of transitioning between PAH-specific medications. We performed a systematic review of all published studies in the Medline database between 1 January 2000 and 30 June 2016 reporting on any transition between the currently Food and Drug Administration (FDA)-approved PAH-specific medications. Studies reporting on three or more adult patients published in the English language reporting on transitions between FDA-approved PAH medications were extracted and tabulated. Forty-one studies met the selection criteria, nine of which included less than eight patients (and thus were reported separately in the supplement), for a total of 32 studies. Transitioning from parenteral epoprostenol to parenteral treprostinil appears to be safe and efficacious in patients who have less severe disease and more favorable hemodynamics. Transitioning from a prostacyclin analogue to an oral medication may be successful in patients who have favorable hemodynamics and stable disease. There is conflicting evidence supporting the transition from a parenteral to an inhaled prostacyclin analogue, even in patients who are on background oral therapy. Currently, the only evidence in support of transitioning between oral PDE5 inhibitors is from sildenafil to tadalafil. Patients on higher doses of sildenafil are more likely to fail. In patients with liver abnormalities due to bosentan or sitaxentan, the transition to ambrisentan appears to be safe and can result in clinical improvement. Studies regarding PAH medication transitions are limited. Patients who have less severe disease, better functional status, and are on lower medications doses may be more successful at transitioning.
Keywords
Introduction
Pulmonary arterial hypertension (PAH) is a progressive disease of the pulmonary vasculature that, if left untreated, has a very poor prognosis.1–3 Since the introduction of infused epoprostenol in 1996, the number and routes of PAH-specific therapies have dramatically increased.4,5 Currently, there are 14 therapies for PAH approved by the United States Food and Drug Administration (FDA) that are available through the intravenous (IV), subcutaneous (SQ), inhaled (IH), and oral routes. These drugs target three main pathways: the nitric oxide, endothelin-1, and prostacyclin pathways; and they currently include five families of drugs: phosphodiesterase type-5 inhibitors (PDE5-I), guanylate cyclase stimulator, endothelin receptor antagonists (ERA), prostacyclin analogues, and selective prostacyclin receptor agonists.5–7 The availability of different classes of medications, different routes, and total number of available PAH-specific medications makes the number of potential transitions within the same class or between classes relatively large. These transitions are already occurring not uncommonly in clinical practice, and there may be pressure by external forces (i.e. third-party payers) to switch medications, often in the absence of high quality data about long-term clinical outcomes/consequences.
Despite the development of newer oral and IH therapies, most patients with advanced disease or rapidly progressive disease still require continuously infused parenteral prostacyclin analogues. Additionally, there is new interest in both upfront and sequential combination therapies. 4 Over 50% of patients with PAH are on more than one PAH-specific therapy. 8 At several large PAH centers, approximately 10% of patients on parenteral prostacyclin have attempted to transition to other therapies.8,9 Typically, patients will attempt to transition therapies because of complications such as line infections 10 or vein stenosis in the case of IV therapies, site pain caused by SQ therapies, intolerable side effects from therapy, or to improve medication compliance relative to the simplicity of dosing with some newer agents.
To evaluate the evidence supporting the efficacy and safety of transitions between PAH-specific medications, we performed a systematic review of published studies of adult patients who were transitioned between the currently FDA-approved PAH therapies.
Materials and methods
Search and selection criteria
We utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 11 to perform a systematic review of all published studies in the Medline database between 1 January 2000 and 30 June 2016 reporting on any transition between the currently FDA-approved PAH-specific medications. Studies were identified using the following search strategy: [“switch” or “switched” or “switching” or “conversion” or “converted” or “transition” or “transitioned” or “transitioning”] AND “pulmonary” AND “hypertension”; dates limit: 01/01/2000 through 06/30/2016.
Intra-class PAH medication transitions: infused prostacyclin analogue to another infused prostacyclin analogue.

6MWD, 6-minute walk distance; FC, functional class; HRQoL, health-related quality of life; IV, intravenous; mPAP, mean pulmonary artery pressure; N/A, not applicable; NT-proBNP, N-terminal pro B-type natriuretic peptide; NYHA, New York Heart Association; QOL, quality of life; SF-36, short form (36) health survey; SQ, subcutaneous; TSQM, treatment satisfaction questionnaire for medication; WHO, World Health Organization.
Data extraction and assessment of risk of bias
To avoid bias, three investigators (WHF, AS, and JAW) independently reviewed the literature and identified the potential studies for inclusion in this systematic review (e-Table 1). All five investigators performed data extraction/ abstraction.
Results
A total of 32 studies are included in the systematic review (Fig. 1). Additional nine studies had less than eight patients and thus were reported separately in the supplement (e-Tables 2–4).
PRISMA diagram of the selection of the studies included in the systematic review. Intra-class PAH medication transitions: prostacyclin analogue from one route to another route (i.e. infused, inhaled, or oral) (other than switched from infused to another infused medication or route). CAMPHOR, Cambridge Pulmonary Hypertension Outcome Review; IH, inhaled. Other abbreviations per Table 1 footnote.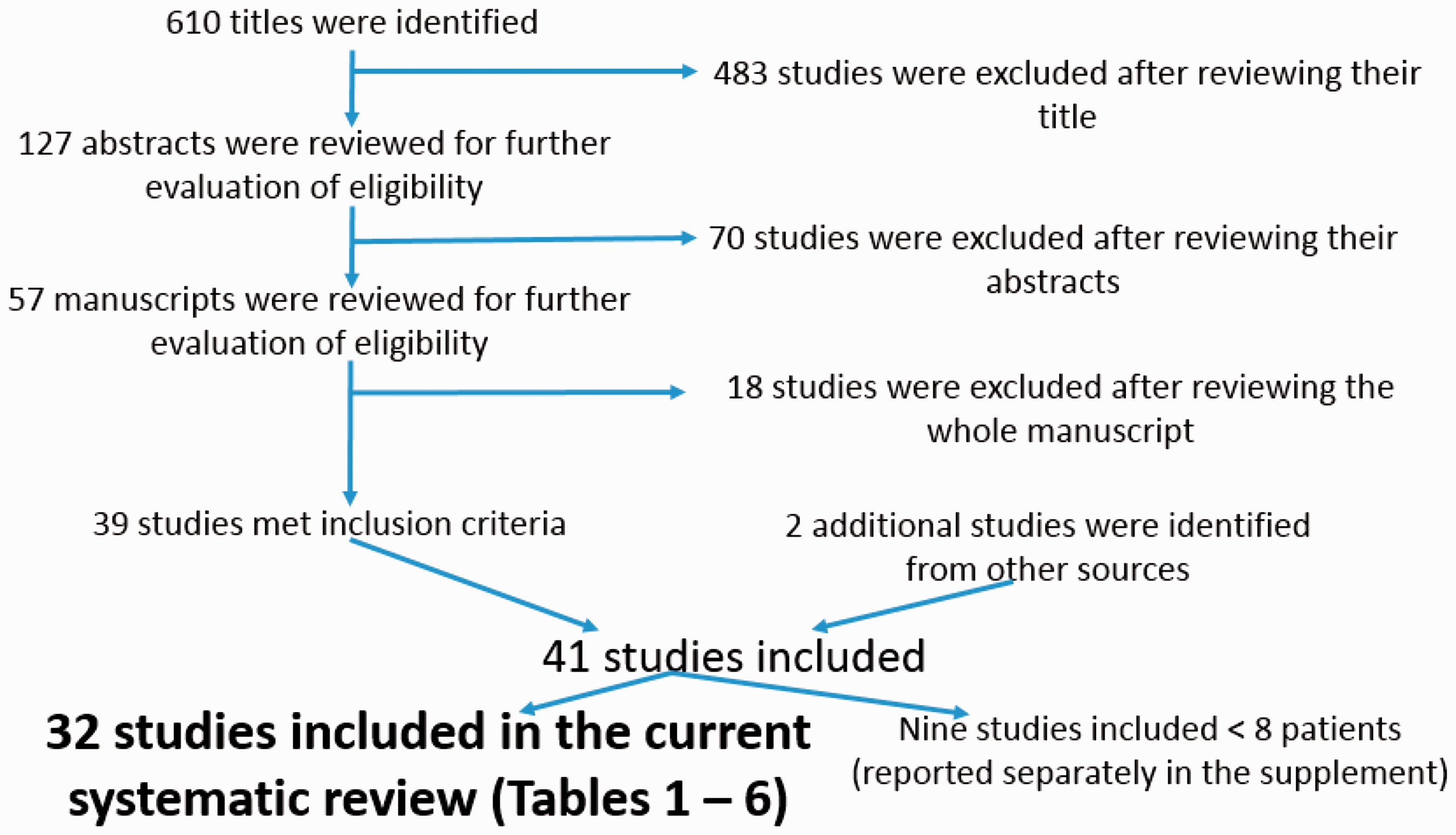
Intra-class PAH medication transitions: from one infused prostacyclin analogue to another infused prostacyclin analogue
There were 11 studies involving the transition from one infused prostacyclin analogue (either IV or SQ) to another infused prostacyclin analogue (Table 1), with a total of 377 patients studied. Two of the 11 studies were retrospective; eight of the studies were prospective open-label studies; and one study 12 was a prospective, randomized controlled trial. The duration of the studies were in the range of 1–12 months. Five out of the nine prospective studies involved transition from IV epoprostenol to either IV or SQ treprostinil, with a total of 108 transition patients studied. The rate of successful transition in these five studies was 86/108 (80%). In general, patients who were successfully transitioned had less severe disease (New York Heart Association [NYHA]) functional class I or II, or World Health Organization [WHO] functional class II or III) and more favorable hemodynamics at baseline. Overall, there was no worsening in WHO functional class or significant differences in 6-minute walk distance (6MWD) in patients who completed the transition.
Only three small studies involved the transition from either SQ or IV treprostinil to IV epoprostenol (Table 1 and e-Table 2), with a total of 18 patients studied and a success rate of 67%. In one of these studies, 13 two of the four “transition” patients died; however, these four patients were transitioned (escalation of care) specifically to try to mitigate clinical worsening of their PAH, rather than for reasons of intractable medication side effects or non-adherence.
Four out of the 11 studies involved the transition from a traditional formulation of IV epoprostenol to a thermostable form, with a total of 254 patients studied and a success rate of 76%. Patients who transitioned successfully tended to have improved quality of life and treatment satisfaction scores. In one of these studies, 14 which was a prospective, open-label registry, freedom from hospitalization rates were higher in patients who transitioned to thermostable IV epoprostenol.
There were no significant safety events in the majority of the studies. In the study by Benza et al., 15 in which 31 patients were transitioned from IV epoprostenol to IV treprostinil, a total of eight transition patients died or discontinued the drug; however, the authors concluded that none of the deaths were related to treprostinil.
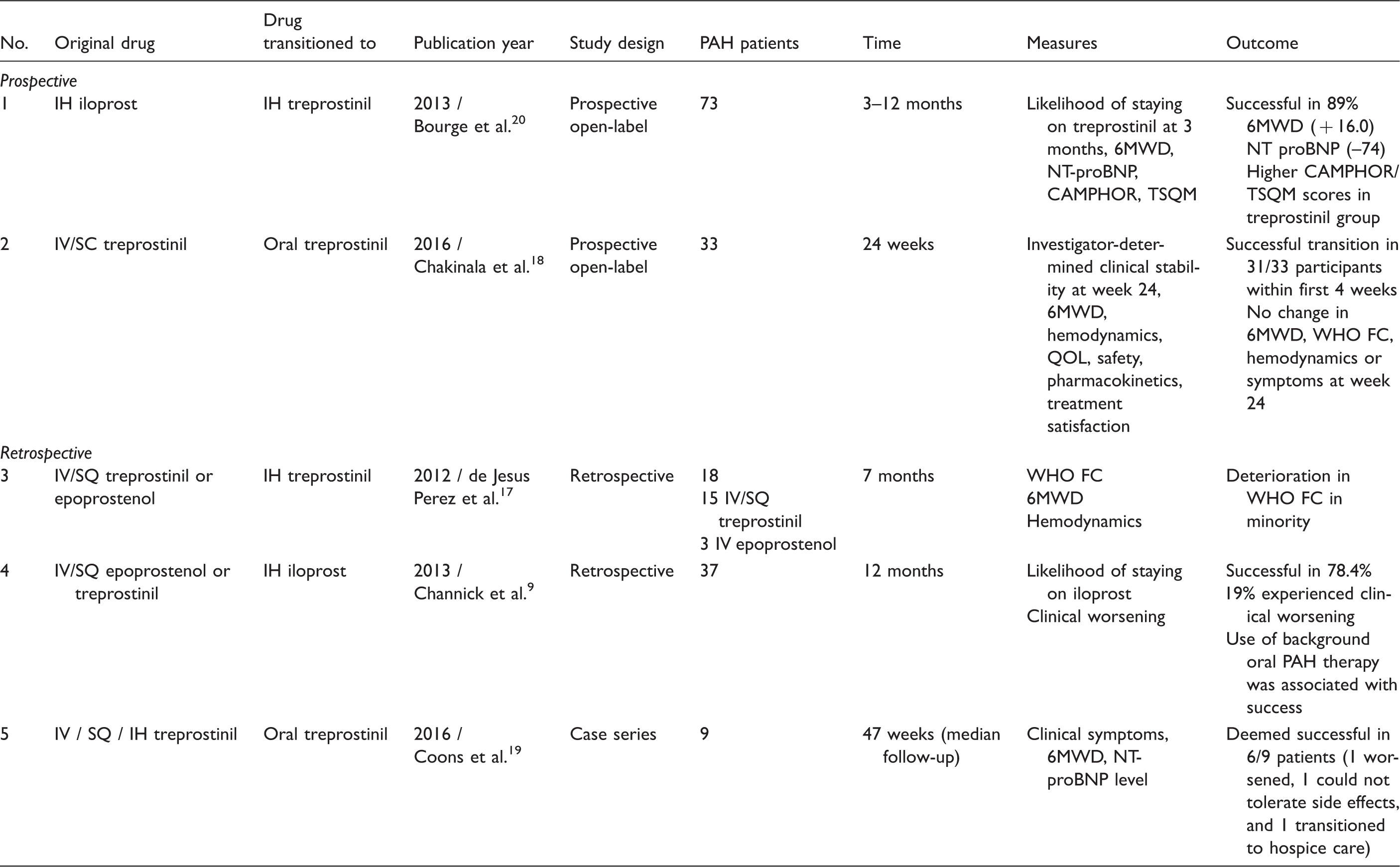
Intra-class PAH medication transitions: from a prostacyclin analogue via one route to a prostacyclin analogue via another route
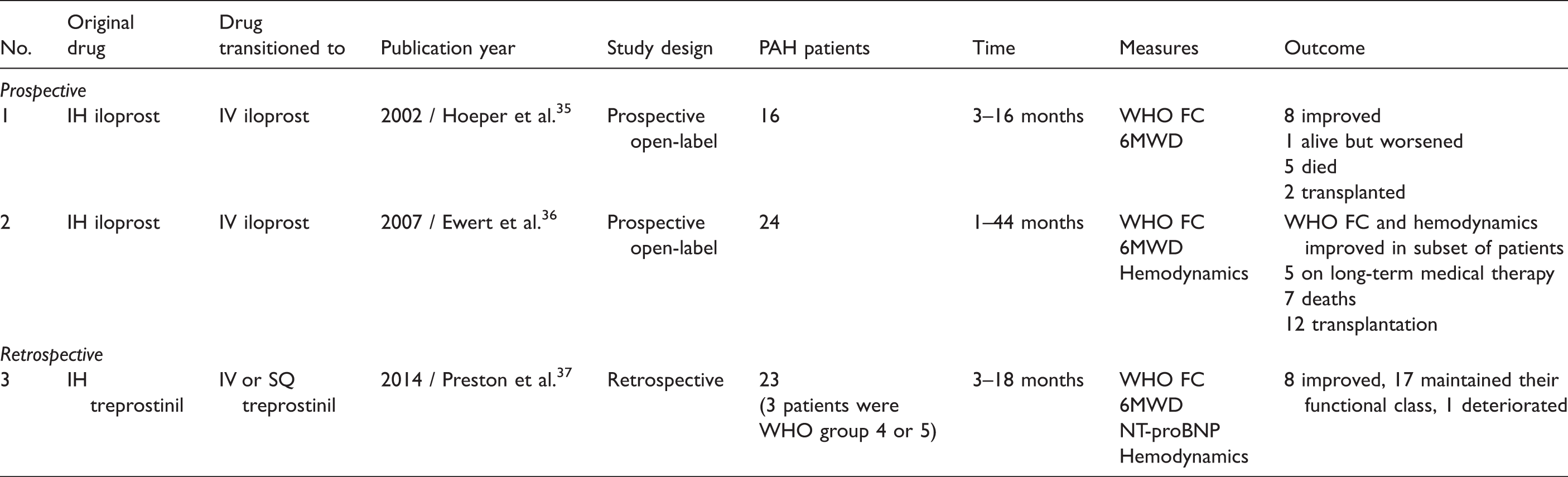
Intra-class PAH medication escalations: prostacyclin analogue from inhaled route to infused route.
Inter-class PAH medication transitions: prostacyclin analogues to oral non-prostacyclin analogue agents.

mPAP, mean pulmonary artery pressure; PG, prostaglandin; PASP, pulmonary artery systolic pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVSP, right ventricular systolic pressure; SDH, subdural hematoma; WU, Wood units.
Two retrospective studies involved the transition from either IV or SQ prostacyclin analogue to an inhaled form, with 55 patients studied. The transition was considered successful in one of these studies.9,16 In a study by Channick et al., 9 in which 81% of patients remained free of clinical symptoms one year after transitioning, one of the major predictors of transition success was the use of background oral PAH therapy. In a small study by Enderby et al. 16 (e-Table 3), in which the transition was considered successful in 3/3 patients, all three patients were on oral PAH therapy prior to the transition. By contrast, in the study by de Jesus Perez et al., 17 in which 18 patients on infused prostanoids as well as background oral PAH therapy were transitioned to IH treprostinil, there was a deterioration in WHO functional class as well as worsening of the 6MWD and NT-proBNP level in a minority of the patients. The authors raised concerns over the “amount of therapeutic control that can be achieved with inhaled therapies.”
Two studies18,19 (Table 2) examined the transition from either IV, SQ, or IH treprostinil to oral treprostinil in a carefully selected, stable cohort of patients. The transition was deemed successful in 37/42 patients (88%).
One study (20) involved the transition from IH iloprost to IH treprostinil. The authors reported an 89% “success” rate and concluded that the transition was “safe and well-tolerated with no apparent loss of clinical status,” and resulted in an average time savings of approximately 1.4 h per day.
Inter-class PAH medication transitions: from a prostacyclin analogue to an oral non-prostacyclin analogue
There were seven studies involving the transition from a prostacyclin analogue to an oral non-prostacyclin analogue (Table 4). Two of the seven studies were prospective, open-label studies, five were retrospective studies. The duration of the studies was in the range of 3–60 months. All seven of these studies involved the transition from a parenterally administered prostanoid to either oral bosentan or sildenafil, with a total of 126 patients studied. In general, patients who were able to transition successfully had a more favorable hemodynamic profile and WHO functional class and were on lower doses of prostacyclin analogues prior to transitioning.
In a study 21 examining transitioning from SQ treprostinil to oral sildenafil, the change was deemed successful in 71% of 14 patients based upon improvements in NHYA functional class and quality of life. In another study 22 of six patients (e-Table 4) with PAH due to Eisenmenger’s syndrome who were transitioned from SQ treprostinil (n = 5) or oral beraprost (n = 1) to oral bosentan, patients had a non-significant decrease in 6MWD and no significant change in WHO functional class.
Intra-class oral PAH medication transitions: from one phosphodiesterase type5 (PDE5) inhibitor to another
Intra-class oral PAH medication transitions: PDE5 inhibitors.
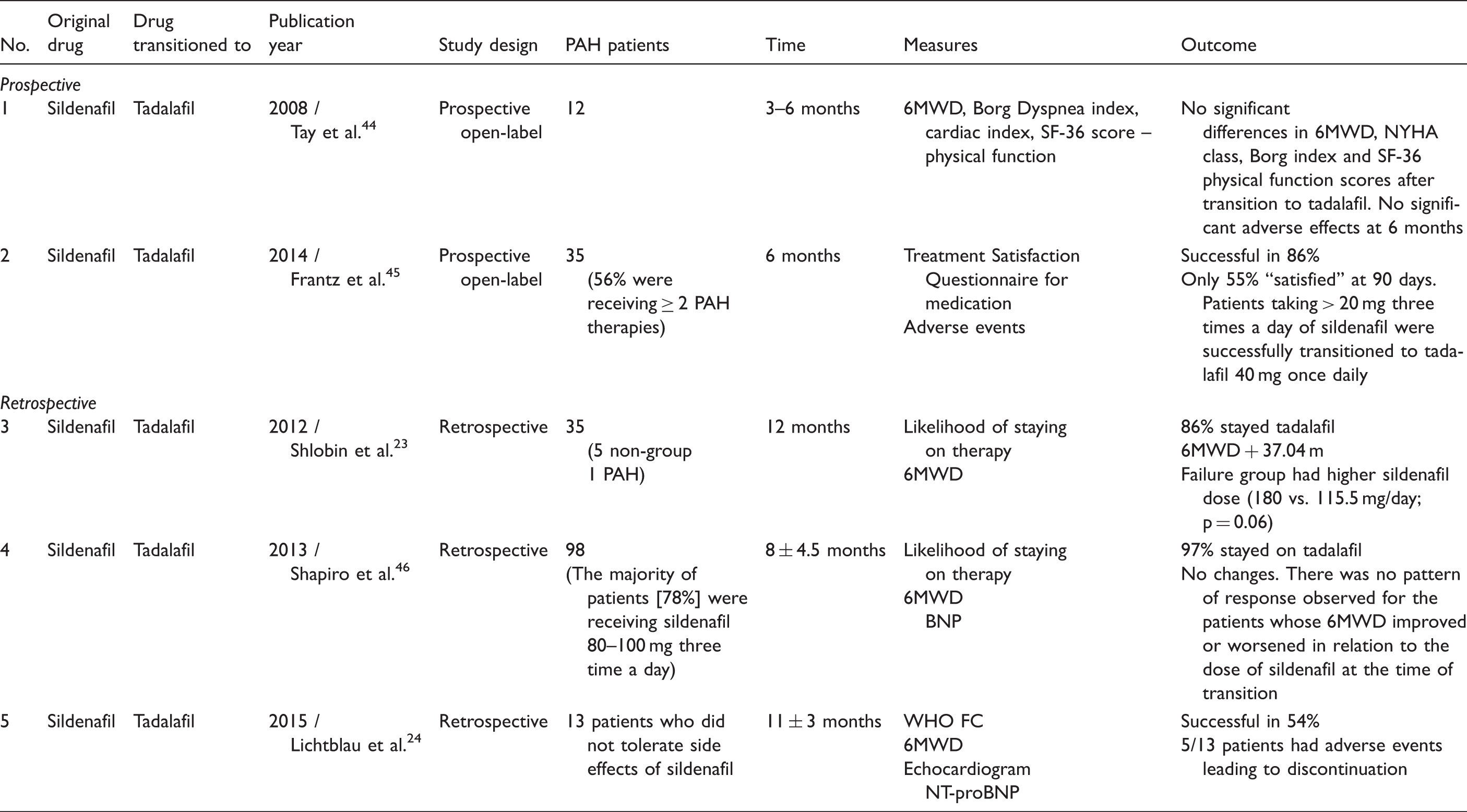
In the study by Lichtblau et al., 24 in which 13 patients who could not tolerate the side effects of sildenafil attempted to transition to tadalafil, the transition success rate was only 54%. Patients who were unable to transition successfully had discontinued the drug due to adverse events. The authors noted that “in almost half of these cases, adverse reactions were similar to those with sildenafil, in the other half, different side effects led to discontinuation of treatment.”
Intra-class oral PAH medication transitions: from one endothelin receptor antagonist (ERA) to another
Intra-class oral PAH medication transitions: endothelin receptor antagonists.

LFT, liver function tests; ULN, upper limit of normal.
Discussion
Certain PAH therapies, particularly those requiring parenteral administration, can pose a significant burden to patients. With the availability of newer and more convenient treatment options for PAH, there has been an increase in the number of patients transitioned between therapies. Despite this increase, there have been a limited number of studies examining the safety and/or efficacy of these transitions. To our knowledge, this is the first systematic review examining transitions between PAH-specific therapies.
The majority of the studies we reviewed involved the transition from a prostacyclin analogue to another medication (Tables 1–4). The studies consisted of both retrospective and prospective open-label studies. The transition from parenteral epoprostenol to parenteral treprostinil was successful in 80% of patients and generally well tolerated. Patients who were successfully transitioned tended to have less severe disease and more favorable hemodynamics at baseline. Overall, there was no worsening in WHO functional class or significant differences in 6MWD in patients who completed the transition. Conversely, there were only few studies reporting on the transition from parenteral treprostinil to parenteral epoprostenol; these studies had a lower success rate for transitioning; however, some of the patients were transitioned (from parenteral treprostinil to parenteral epoprostenol) to address clinical worsening rather than mitigation of drug side effects.
The transition from parenteral epoprostenol to a thermostable form was generally successful, and patients who transitioned tended to have improved quality of life, treatment satisfaction scores, and freedom from hospitalization.
There were limited studies examining the transition from an IH prostacyclin analogue to a parenteral prostanoid. Patients in these studies generally had more severe disease and were “transitioned” as a form of rescue therapy. Most of these patients were able to achieve short-term clinical and hemodynamic stabilization but had subsequent disease progression, including death or lung transplantation.
There is conflicting evidence involving the transition from a parenteral prostacyclin analogue to an IH form. Two studies examining this transition9,16 in patients who were on background oral PAH therapy reported success, whereas one study 17 reported clinical deterioration in a minority of patients. Therefore, clinicians should carefully discuss the risks and benefits of this particular transition with their patients and ensure close monitoring during and after the transition period. The transition from parenteral to oral treprostinil was evaluated in two studies18,19 and it appears to be feasible and safe in low-risk, clinically stable patients. The transition from inhaled iloprost to inhaled treprostinil was evaluated in one study 20 and appears to be safe and well tolerated, and can result in modest time savings.
The transition from a parenteral prostacyclin analogue to an oral non-prostacyclin analogue was evaluated in seven studies (Table 4), with variable success rates. Most of these patients were transitioned from either epoprostenol or treprostinil to bosentan or sildenafil. Patients who successfully transitioned tended to have more favorable hemodynamics, better functional class and higher 6MWD at baseline compared with those who failed, and were on lower doses of prostacyclin analogues prior to transitioning.
In terms of intra-class oral PAH medication transitions, only sildenafil to tadalafil and bosentan or sitaxsentan to ambrisentan are supported by the available evidence. Most patients successfully transitioned from oral sildenafil to once daily tadalafil; patients who failed to do so were on a higher dose of sildenafil at baseline, thus raising concerns about the safety and efficacy of transitioning patients on higher doses of sildenafil. Other patients who may not transition successfully are those who have experienced intolerable side effects from sildenafil.
Limitations and potential biases
One major limitation of this systematic review is the heterogeneity of the studies reviewed and the heterogeneity of the patients included in these studies; including reasons for transitioning, inconsistency in defining “successful transition,” variable length of follow-up, and lack of standardized protocols for transitioning patients from one drug to another, especially in the case of infused prostanoids. For example, patients may have transitioned to a different medication as a form of rescue therapy in some studies rather than to reduce unwanted side effects of initial therapy, which would lead to significant bias. In addition, the PAH subtype and severity of disease, as well as background therapy and combination therapy are confounders that could not be accounted for in this analysis as they were not well described or characterized in many of the above studies. Additionally, most of these studies were retrospective reviews with small sample sizes (only one study was a prospective trial) limiting the generalizability of the data. It is also difficult to generalize our findings to the pediatric population, in which studies are severely limited. In addition, publication bias could not be accounted for, as unsuccessful transitions would be unlikely to be published.
Implications for clinical practice
Patients and clinicians may wish to transition between PAH therapies for a variety of reasons. We have provided a comprehensive review of the available evidence to guide clinicians in discussing transitions between PAH-specific therapies with their patients, as well as patient-specific characteristics that may help predict the likelihood of a successful transition. More studies 26 are expected to further guide clinicians when considering transitions between PAH medications.
Conclusion
In summary, data regarding transitions between PAH-specific therapies are limited and the quality of the available evidence is variable. Certain patient characteristics, such as severity of disease as well as baseline hemodynamic profile and clinical parameters may help clinicians predict the likelihood of a successful transition between different PAH therapies. Patients will require careful monitoring during and after the transition period to ensure clinical stability and to monitor for adverse effects.
Footnotes
Conflict of interest
WHF is on the Speakers Bureau of Actelion, Gilead, & United Therapeutics/Lung; and advisory Board of Actelion, Bayer, Gilead, and United Therapeutics. JAW (Principal Investigator for Actelion, Bayer, Gilead, Lung LLC, and United Therapeutics). RJT serves as a hemodynamic core-lab for a Actelion phase II study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.