
Abstract
Background:
Modafinil is a wakefulness-promoting agent widely used for narcolepsy and other sleep disorders. Although considered relatively safe, psychotic episodes associated with its use have been reported. However, no systematic review has focused on modafinil-associated psychosis.
Objectives:
To synthesize and describe the clinical characteristics, diagnostic backgrounds, and treatment outcomes of modafinil-associated psychosis through a systematic review of case reports and series.
Design:
Systematic review of published case reports and case series.
Data sources and methods:
A systematic literature search was conducted using PubMed and Web of Science. Case reports and series in English describing psychosis related to modafinil or armodafinil use were included. Age, sex, dose, diagnosis, symptoms, treatment, and outcomes were extracted and descriptively analyzed.
Results:
Twenty-four patients (13 men and 11 women, mean age 37.4 years) from 21 articles were included. The most common symptoms were hallucinations (66.7%) and delusions (58.3%). Median modafinil dose was 250 mg/day; however, some patients received excessive doses. The diagnoses included narcolepsy (33.3%), schizophrenia (20.8%), and depression (20.8%). Eighteen patients (75.0%) were treated with antipsychotics, and 16 (66.7%) discontinued modafinil. Most patients (70.8%) showed marked improvement.
Conclusion:
Modafinil-associated psychosis can develop across wide diagnostic and age ranges, and sometimes even at therapeutic doses. Although the potential risk factors remain unclear, caution should be exercised regarding the drug’s use at high doses, in patients with comorbid psychiatric conditions, and in cases of off-label usage for cognitive enhancement. Long-term follow-up is necessary to monitor outcomes and transition to schizophrenia. Further research is needed to identify the predictive factors and elucidate the underlying neurobiological mechanisms.
Trial registration:
Not registered.
Introduction
Modafinil is a wakefulness-promoting agent to treat excessive daytime sleepiness in patients with narcolepsy and other sleep disorders. The clinical guidelines of the American Academy of Sleep Medicine (AASM) recommend modafinil for treating narcolepsy and idiopathic hypersomnia. 1 The guidelines strongly favor modafinil because of its favorable balance between efficacy and adverse effects. However, psychotic episodes associated with modafinil use have been reported in patients with sleep disorders such as narcolepsy,2–4 idiopathic hypersomnia, 5 and Kleine-Levin syndrome. 6 Although modafinil has been investigated for its potential benefits on negative symptoms in patients with schizophrenia,7–10 exacerbation of psychotic symptoms has been documented in patients with schizophrenia who were administered modafinil.11–13
In this manuscript, we refer to psychosis that developed or worsened following modafinil use as “modafinil-associated psychosis.” We refrained from using the term “modafinil-induced,” which implies a definite causal relationship between modafinil use and psychosis. Because the available evidence consists largely of case reports and case series and therefore cannot reliably establish causality, we use association-based terminology. Modafinil-associated psychosis presents with heterogeneous backgrounds, and understanding its clinical characteristics is important in sleep medicine and psychiatric practice. However, previous reviews on substance-induced psychosis (SIP) have not extended to modafinil,14,15 and no comprehensive systematic review of modafinil-associated psychosis has yet been conducted. Consequently, its clinical features remain unclear, and no standardized management strategies have been established.
Given the rarity and heterogeneous nature of modafinil-associated psychosis, available evidence has been limited to individual case reports. In this context, systematically reviewing these cases represents a valuable step toward identifying clinical patterns and guiding future research. Therefore, we conducted a systematic review of modafinil-associated psychosis to better characterize its clinical manifestations and explore implications for management and prevention.
Methods
Study design
We conducted a systematic review of published case reports and case series describing psychotic symptoms occurring in association with modafinil or armodafinil use. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. 16
Registration and protocol
This review was not registered, and no protocol was prepared.
Eligibility criteria
The inclusion criteria for this review were as follows: (1) case reports or case series describing psychotic episodes associated with the use of modafinil or armodafinil, and (2) articles written in English. The exclusion criteria were as follows: (1) studies that did not involve human participants, (2) studies unrelated to psychosis, (3) studies unrelated to modafinil or armodafinil, (4) review articles, (5) records that were not in English, (6) records published only as a poster, and (7) records for which the full text was unavailable. For records for which the full text was unavailable, we did not contact corresponding authors prior to exclusion; records were excluded when full texts could not be obtained through available institutional channels.
Search strategy and information sources
This systematic review was conducted and reported in accordance with the PRISMA 2020 statement, 16 and the completed PRISMA checklist is provided in Supplemental File S1. A comprehensive literature search was performed in PubMed and Web of Science on November 7, 2024, using the following search terms: modafinil AND (psychosis OR psychotic OR schizophrenia). For Web of Science, a custom publication date range (1900-01-01–2024-11-07) was applied. The full search strategies are provided in Supplemental File S2. Additional relevant articles were identified through manual screening of reference lists. All identified articles were imported into EndNote, and duplicate articles were removed. Screening was conducted in two steps. First, one reviewer (Y.S.) screened titles and abstracts to exclude clearly irrelevant studies. Second, two reviewers (Y.S. and A.S.) independently assessed the potentially eligible full-text articles, discussed discrepancies, and reached consensus on the final selection of studies for inclusion.
Data extraction
The following information was extracted from each included article: first author, publication year, patient age, sex, diagnoses/comorbidities, modafinil dose, psychotic symptoms, treatment, and clinical outcomes. Diagnoses/comorbidities included sleep, psychiatric, developmental, and neurological disorders, as well as relevant medical conditions when reported. Clinical outcomes were categorized as follows: “no improvement”: psychotic symptoms persisted without alleviation, “partial improvement”: psychotic symptoms were alleviated but persisted or recurred, and “marked improvement”: psychotic symptoms were alleviated and did not recur. For descriptive synthesis, treatment outcomes were categorized as follows: “Antipsychotics only” (antipsychotic treatment without discontinuation of modafinil/armodafinil), “Discontinuation of modafinil only” (discontinuation of modafinil/armodafinil without antipsychotic treatment), or “Antipsychotics and discontinuation of modafinil” (both antipsychotic treatment and discontinuation of modafinil/armodafinil). Two reviewers (Y.S. and A.S.) independently verified that the data extraction was performed accurately and consistently. When information was not provided in the original report, it was recorded as “Not reported” and treated as missing. For continuous variables (e.g., total daily dose), summary statistics were calculated using available-case data (i.e., including only cases with reported numeric values). For categorical summaries (e.g., diagnoses/comorbidities, treatment, and outcomes), proportions were calculated using the total number of included cases as the denominator unless otherwise specified.
Synthesis method
Descriptive statistical analyses were performed using IBM SPSS Statistics version 25 (BM Corp., Armonk, NY, USA). The clinical characteristics of patients were summarized as percentages, means, standard deviations, and medians, as appropriate. Findings were summarized descriptively. Study- and case-level characteristics were tabulated, and the study selection process was summarized using a PRISMA flow diagram. We conducted a sensitivity analysis excluding an extreme overdose case to examine the robustness of dose summary statistics.
Quality assessment
The methodological quality of the included studies was assessed using a standardized tool proposed by Murad et al. 17 (Supplemental Table S1). Each study was rated as having low (0–2 points), moderate (3–5 points), or high (6–8 points) methodological quality using author-defined cut-offs for descriptive summarization, based on the total score (0–8 points).
Results
Study selection
Our systematic literature search initially identified 367 articles. After screening titles and abstracts, 186 articles were excluded. Following a full-text review, 17 articles met the eligibility criteria, and four additional articles were identified through manual reference search. In total, 21 articles describing 24 cases were included in this review (Figure 1). A list of full-text articles excluded after eligibility assessment, with reasons, is provided in Supplemental Table S3. Detailed case-level characteristics are provided in Supplemental Table S4.2–6,11–13,18–30

PRISMA flow diagram of study screening and selection.
Clinical characteristics of the cases
The clinical characteristics of the reviewed cases are summarized in Table 1. The mean patient age was 37.4 (range: 13–79) years. Because this estimate was driven by a single intentional overdose case (12,000 mg/day), 5 we also calculated the mean excluding this outlier as a sensitivity analysis; the mean daily dose was 363 mg/day when the overdose case was excluded. The male: female patient ratio was 13:11. The average modafinil dose was 945 mg/day (range: 100–12,000 mg/day). The median modafinil dose was 250 mg/day. The most common diagnoses were narcolepsy (33.3%), schizophrenia (20.8%), and depression (20.8%). Ten cases (41.7%) involved sleep disorders such as narcolepsy, idiopathic hypersomnia, Kleine-Levin syndrome, and sleep apnea. Among these, one case reported by Canellas et al. 27 involved both narcolepsy and sleep apnea. Among cases with schizophrenia, modafinil was used for narcolepsy in only one case reported by Canellas et al. 27 Modafinil was used to treat sedation caused by clozapine in the case reported by Narendran et al. 11 In the cases reported by Aggarwal et al., 12 modafinil was used for excessive sleep and negative symptoms. The two cases reported by Neto et al., 13 were used modafinil for negative symptoms. The most frequently reported psychotic symptoms were hallucinations (66.7%) and delusions (58.3%). Among hallucinations, auditory (45.8%), visual (33.3%), and multimodal (20.8%) types were described. In the case reported by Mariani and Hart, 18 neither hallucinations nor delusions were present, but disorganization was observed. One of the cases reported by Dauvillier et al. 19 lacked detailed descriptions of psychotic symptoms. Psychosis was treated with antipsychotics in 75.0% of patients, and modafinil (or armodafinil) was discontinued in 66.7% of cases. Treatment outcomes were summarized in Table 2.
Clinical characteristics of the cases.

Two cases were excluded because information on age at modafinil initiation was unavailable.
Three cases were excluded because information on the modafinil dose was not available, and one case was excluded because armodafinil was used.
The intentional overdose case (12,000 mg/day) was excluded in the sensitivity analysis.
Diagnoses were not mutually exclusive; some patients had multiple diagnoses.
Antipsychotic frequencies were not mutually exclusive; some cases received more than one agent.
The case in which armodafinil was used was also included.
Treatment and improvement of psychosis.
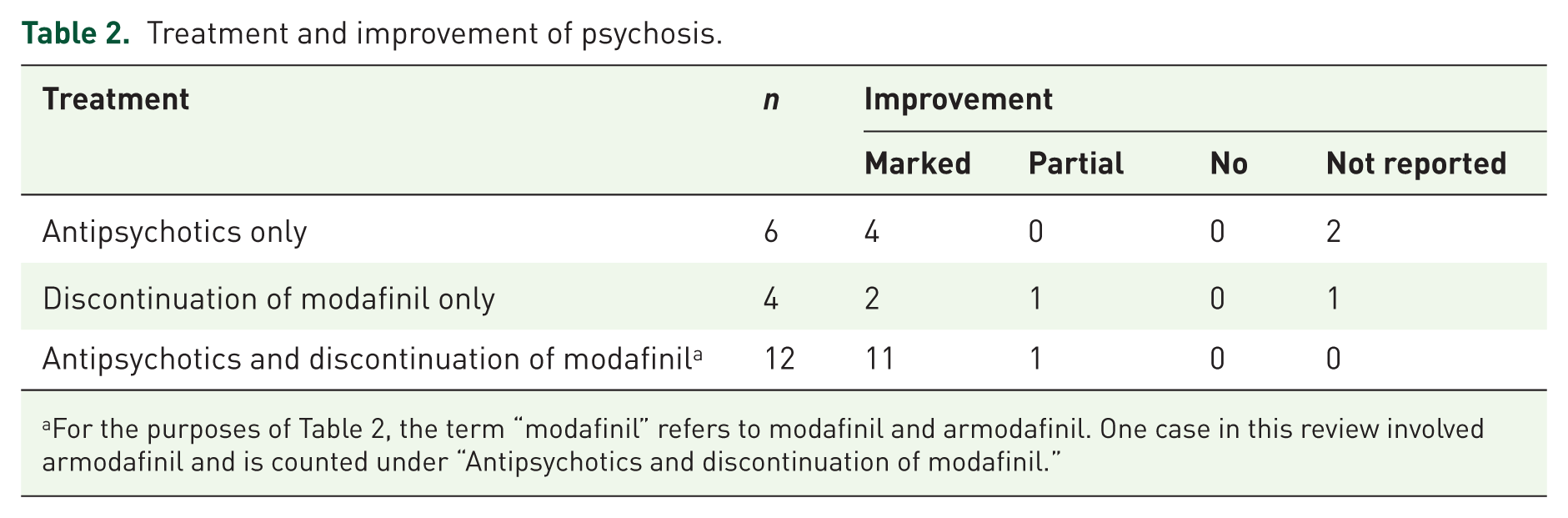
For the purposes of Table 2, the term “modafinil” refers to modafinil and armodafinil. One case in this review involved armodafinil and is counted under “Antipsychotics and discontinuation of modafinil.”
Quality assessment
The methodological quality of the included studies was assessed using a standardized tool. 17 Eight cases were rated as high quality, 15 as moderate quality, and one as low quality. The detailed quality assessment of each case is presented in Supplemental Table S2.
Discussion
To our knowledge, this is the first systematic review of reported cases of modafinil-associated psychosis. The strengths of this work include a literature search performed using systematic methods and the detailed examination of clinical characteristics through the review of case reports and case series.
Modafinil-associated psychosis has been observed across a wide age range. The youngest patient was a 13-year-old with Kleine-Levin syndrome, 6 and the oldest was a 79-year-old with dementia with Lewy bodies. 25 These findings indicated that modafinil-associated psychosis should be considered in any patient using modafinil, regardless of age.
Considering that modafinil is recommended for narcolepsy, 1 it is not surprising that narcolepsy was the most common diagnosis among the reviewed cases. Hanin et al. 31 reviewed narcolepsy cases with psychotic-like symptoms or comorbid psychotic disorders and proposed a clinical algorithm. However, their analysis primarily focused on the overall clinical spectrum of psychotic phenomena in narcolepsy and only minimally addressed the specific influence of modafinil. Among the studies they reviewed, only a limited number of cases, such as those reported by Vorspan et al., 2 Dauvilliers et al., 19 and Canellas et al., 27 described psychotic episodes in narcolepsy patients treated with modafinil. In addition, the case presented by Crosby et al., 32 involved mania in a narcolepsy patient taking modafinil and venlafaxine, without documented psychotic symptoms. Therefore, the direct evidence linking modafinil to psychosis in their review was limited. In contrast, the present review focuses on psychotic episodes occurring in association with modafinil use, regardless of the underlying diagnosis. In the algorithm proposed by Hanin et al., 31 patients with narcolepsy and psychotic symptoms were classified into three groups: (1) typical narcolepsy hallucinations, (2) narcolepsy with psychotic-like symptoms, and (3) narcolepsy with psychotic disorders. They suggested that patients in any group may experience SIP, especially those receiving high doses of psychostimulants or with a history of psychotic symptoms, and recommended modafinil as a wakefulness drug with the lowest risk of psychosis. For patients with comorbid narcolepsy and psychotic disorders (Group 3), fewer sedating antipsychotics, such as aripiprazole and risperidone, were recommended. This algorithm may help guide the management of modafinil-associated psychosis in patients with narcolepsy.
Balancing the treatment of narcolepsy with modafinil against the risk of psychosis can be challenging. In the case reported by Yasui-Furukori et al., 4 modafinil was resumed for treating recurrent narcoleptic symptoms, and the patient was able to manage occasional auditory hallucinations through psychoeducation. Psychoeducation may thus play an important role in the management of modafinil-associated psychosis.
It should be noted that the majority of patients in the reviewed cases used modafinil, despite having no diagnosis of sleep disorders. Modafinil has been prescribed to alleviate fatigue, loss of energy, and excessive daytime sleepiness in patients with depression.23,24 A network meta-analysis showed that modafinil was superior to placebo for treatment-resistant depression. 33 The 2023 Canadian Network for Mood and Anxiety Treatments guidelines continue to recommend adjunctive modafinil treatment as second-line option for difficult-to-treat depression. 34 While this recommendation may encourage clinicians to prescribe modafinil for treating depression, especially with excessive daytime sleepiness, the cases reported by Oulis et al. 24 and Kanal et al. 23 underscore the need for careful monitoring during its use.
Modafinil treatment in patients with schizophrenia also warrants attention. In a case of schizophrenia reported by Narendran et al., 11 modafinil was added to treat severe daytime sedation associated with clozapine. Aggarwal et al., 12 prescribed modafinil to address excessive sleep and negative symptoms, and Neto et al., 13 used modafinil for negative symptoms. A meta-analysis by Ortiz-Orendain et al. 8 found that adding modafinil to antipsychotic treatment had little or no effect on the overall mental state of patients with schizophrenia, specifically regarding the risk of worsening psychosis. They noted that there was no difference in effectiveness and safety between add-on modafinil and placebo, and that these findings were based on low- or very low-quality evidence and were therefore inconclusive. A meta-analysis by Sabe et al. 9 found no significant effect of modafinil/armodafinil on negative symptoms in the overall sample of patients with schizophrenia, but reported a significant improvement in a subset of studies that required a minimum threshold for the severity of negative symptoms. A more recent meta-analysis by Osugo et al. 10 supported these findings, suggesting a benefit for modafinil/armodafinil in patients with predominant negative symptoms. Osugo et al. emphasized the need to determine whether this effect is specific to modafinil/armodafinil. Nevertheless, the safety of modafinil use in patients with schizophrenia remains insufficiently supported by robust evidence. As shown in the present review, several cases have reported the development of psychotic episodes following modafinil administration in individuals with schizophrenia. Therefore, further high-quality clinical research is warranted, and clinicians should exercise caution and carefully consider the risk–benefit balance when prescribing modafinil in this population.
The mechanisms underlying modafinil-associated psychosis remain poorly understood. Modafinil affects multiple neurotransmitter systems, including dopamine, norepinephrine, serotonin, glutamate, gamma-aminobutyric acid (GABA), orexin, and histamine in the brain. 35 It blocks dopamine transporters and increases dopamine levels in the human brain. 36 The enhancement of dopamine signaling by modafinil may precipitate or exacerbate psychosis. Its effect on the GABAergic system is also noteworthy as a hypothesized mechanism of modafinil-associated psychosis. Narendran et al. 11 speculated that modafinil may aggravate the already impaired GABAergic inhibition observed in schizophrenia by reducing GABA release, leading to psychosis exacerbation. Modafinil may serve as a useful probe in translational research and in developing animal models of schizophrenia.
The mean dose of modafinil was 945 mg/day, higher than the recommended dose for narcolepsy. 37 In contrast, the median dose was 250 mg/day, a typical therapeutic range. This discrepancy reflects the inclusion of a case involving intentional overdose. 5 In this case, a 17-year-old girl diagnosed with idiopathic hypersomnia attempted suicide by ingesting 12,000 mg of modafinil, leading to toxic encephalopathy followed by psychosis. Şahan and Bölükbaşı 5 suggested that such “modafinil intoxication” represents an organic mental disorder requiring intensive care. This extreme presentation could be viewed as a distinct subtype of modafinil-associated psychosis.
The non-medical use of modafinil for cognitive enhancement also warrants concern. This issue is directly relevant to the present review because such use often occurs outside clinical supervision and may involve dose escalation, increasing exposure among individuals with unrecognized vulnerability to psychosis and potentially leading to more cases of modafinil-associated psychosis in practice. In the United Kingdom, the use of psychostimulants as “cognitive enhancers” has increased among students, and lifetime use of modafinil exceeds that of methylphenidate or dexamphetamine. 38 In a case report by Rudhran et al., 26 a 21-year-old man used high doses (1600 mg) of modafinil to improve concentration during preparation for entrance examinations. Similarly, Aytaş and Dilek Yalvaç 29 reported the case of an 18-year-old woman who developed psychosis after being prescribed 100 mg/day of modafinil to increase attention and enhance academic performance. Clinicians should remain alert to modafinil use among youth, especially in students seeking cognitive enhancement, even at therapeutic doses. In addition, it is important to focus on the concerns of young people seeking cognitive enhancement. In the case reported by şahan and Bölükbaşı, 5 a 17-year-old girl preparing for university entrance examinations attempted suicide by overdosing with 12,000 mg of modafinil due to various stressors and exam anxiety. There may be a need for early intervention services for students struggling academically owing to attention and concentration difficulties. Recent reports of modafinil-associated psychosis in patients with comorbid attention deficit hyperactivity disorder also suggest the growing importance of the management of these difficulties.21,28,30 Rudhran et al., 26 considered the possibility of the prodrome of schizophrenia in their case. In individuals at clinical high risk for psychosis (CHR-P), cognitive dysfunction in domains including attention/vigilance has been observed.39,40 A potential pathway to psychosis may involve compensatory modafinil use among individuals with CHR-P to manage such cognitive dysfunction. A recent case report described an individual at CHR-P treated with a maximum dose of 300 mg/day of modafinil for comorbid idiopathic hypersomnia without adverse effects or transition to psychosis. 41 Although this single case report does not provide sufficient evidence to establish the safety of modafinil in individuals at CHR-P, it highlights the need for further clinical observation and research.
In this review, the main symptoms of modafinil-associated psychosis, hallucinations and delusions, resembled the symptom profile commonly observed in SIP, such as that associated with methamphetamine use. 42 While modafinil-associated psychosis can be considered a type of SIP, we deliberately avoided using the term “modafinil-induced psychosis,” which implies a causal relationship between modafinil and psychosis. Recently, the validity of the concept of SIP has been discussed. 43 Bramness et al. 43 argued that substance use is not a sufficient cause of SIP and that several other risk factors are overlooked. They proposed that SIP should be regarded as a psychotic disorder rather than merely a subtype of substance use disorder, and that treatment and follow-up should mirror those for first-episode psychosis (FEP). Their argument was supported by recent studies, including a meta-analysis reporting that 25% of SIP cases later transitioned to schizophrenia. 14 Most patients included in our review had favorable outcomes after appropriate clinical intervention, suggesting that modafinil-associated psychosis may be non-chronic and responsive to treatment, particularly when recognized early and managed appropriately. However, the long-term prognosis remains uncertain, and the possibility of recurrent psychotic episodes or a later transition to psychotic disorders cannot be ruled out. If clinicians consider modafinil-associated psychosis solely as a form of substance use disorder, appropriate treatment and follow-up may be neglected. Therefore, it would be desirable to develop clinical guidelines for modafinil-associated psychosis that recommend treatment and longitudinal monitoring similar to those for FEP, as Bramness et al. 43 proposed for SIP. Given the paucity of evidence, it is important to provide psychoeducation, engage in shared decision-making, and ensure careful clinical follow-ups. Future studies should investigate the long-term course of modafinil-associated psychosis and identify its predictive and biological risk factors.
Based on the findings of this study, we propose the following recommendations:
(1) When psychosis emerges during modafinil treatment, clinicians should engage in shared decision-making regarding antipsychotic treatment and the continuation or discontinuation of modafinil, along with providing psychoeducation on psychotic symptoms.
(2) Greater attention should be paid to the non-medical use of modafinil for cognitive enhancement, particularly among young people who may be at CHR-P, because such use may occur without clinical supervision and may involve dose escalation, potentially increasing the risk of modafinil-associated psychosis. Youth mental health services should address attention and concentration problems that impair academic performance.
(3) In both clinical and research contexts, potential risk factors for modafinil-associated psychosis and subsequent transition to schizophrenia should be systematically evaluated and monitored over time to assess long-term outcomes.
(4) Further clinical and pharmacological research is required to elucidate the mechanisms by which modafinil may trigger or exacerbate psychosis and to inform safer therapeutic approaches.
Limitations
This study has several limitations. First, this review was not prospectively registered (e.g., PROSPERO), and no a priori protocol was prepared. Second, our literature search was limited to two electronic databases (PubMed and Web of Science). Although we also performed hand searching/citation screening, relevant reports indexed elsewhere may have been missed. In addition, our search strategy (i.e., search terms and indexing) may not have been fully comprehensive. Some records were excluded because the full text could not be obtained through available institutional channels, and we did not contact authors for these records. Therefore, eligible reports may have been missed. Third, although we summarized methodological quality into low/moderate/high categories for ease of interpretation, this approach may obscure domain-specific weaknesses that are particularly important in a given clinical context. Accordingly, these summary ratings should be interpreted as supportive rather than definitive, and the item-level appraisal (Supplemental Table S2) should be considered alongside the overall category. Fourth, this review was based solely on case reports and case series, which are inherently prone to selection and publication biases. Fifth, this review only included articles published in English, which may have led to the exclusion of relevant data reported in other languages. Sixth, there was considerable heterogeneity among the cases with respect to diagnosis, modafinil dosage, treatment setting, and reporting of clinical details, limiting the generalizability of our findings. Finally, prognostic descriptions in many reports were brief or lacked standardized outcome assessments.
Conclusion
This review provides the first comprehensive synthesis of reports on modafinil-associated psychosis and highlights key clinical patterns and management challenges. Clinicians should remain vigilant regarding the potential non-medical use of modafinil, particularly among students seeking cognitive enhancement, and should closely monitor for emerging psychotic symptoms in individuals taking modafinil, even at therapeutic doses. Further studies are needed to elucidate the pathophysiology of modafinil-associated psychosis, establish standardized management strategies, and clarify its long-term outcomes, including the risk of transition to schizophrenia.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253261446554 – Supplemental material for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies
Supplemental material, sj-docx-1-tpp-10.1177_20451253261446554 for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies by Yutaro Sato, Atsushi Sakuma and Hiroaki Tomita in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253261446554 – Supplemental material for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies
Supplemental material, sj-docx-2-tpp-10.1177_20451253261446554 for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies by Yutaro Sato, Atsushi Sakuma and Hiroaki Tomita in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-3-tpp-10.1177_20451253261446554 – Supplemental material for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies
Supplemental material, sj-docx-3-tpp-10.1177_20451253261446554 for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies by Yutaro Sato, Atsushi Sakuma and Hiroaki Tomita in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-4-tpp-10.1177_20451253261446554 – Supplemental material for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies
Supplemental material, sj-docx-4-tpp-10.1177_20451253261446554 for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies by Yutaro Sato, Atsushi Sakuma and Hiroaki Tomita in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-5-tpp-10.1177_20451253261446554 – Supplemental material for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies
Supplemental material, sj-docx-5-tpp-10.1177_20451253261446554 for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies by Yutaro Sato, Atsushi Sakuma and Hiroaki Tomita in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-6-tpp-10.1177_20451253261446554 – Supplemental material for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies
Supplemental material, sj-docx-6-tpp-10.1177_20451253261446554 for Modafinil-associated psychosis: a systematic review of case characteristics and management strategies by Yutaro Sato, Atsushi Sakuma and Hiroaki Tomita in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.