
Abstract
Despite its enduring relevance as the single most effective and important evidence-based treatment for schizophrenia, underutilization of clozapine remains considerable. To a substantial degree, this is attributable to a reluctance of psychiatrists to offer clozapine due to its relatively large side-effect burden and the complexity of its use. This underscores the necessity for continued education regarding both the vital nature and the intricacies of clozapine treatment. This narrative review summarizes all clinically relevant areas of evidence, which support clozapine’s wide-ranging superior efficacy – for treatment-resistant schizophrenia (TRS) and beyond – and make its safe use eminently feasible. Converging evidence indicates that TRS constitutes a distinct albeit heterogeneous subgroup of schizophrenias primarily responsive to clozapine. Most importantly, the predominantly early onset of treatment resistance and the considerable decline in response rates associated with its delayed initiation make clozapine an essential treatment option throughout the course of illness, beginning with the first psychotic episode. To maximize patients’ benefits, systematic early recognition efforts based on stringent use of TRS criteria, a timely offer of clozapine, thorough side-effect screening and management as well as consistent use of therapeutic drug monitoring and established augmentation strategies for suboptimal responders are crucial. To minimize permanent all-cause discontinuation, re-challenges after neutropenia or myocarditis should be considered. Owing to clozapine’s unique efficacy, comorbid conditions including substance use and most somatic disorders should not dissuade but rather encourage clinicians to consider clozapine. Moreover, treatment decisions need to be informed by the late onset of clozapine’s full effects, which for reduced suicidality and mortality rates may not even be readily apparent. Overall, the singular extent of its efficacy combined with the high level of patient satisfaction continues to distinguish clozapine from all other available antipsychotics.
Introduction
With a life-time prevalence of 4.8–7.2 per 1000,1,2 schizophrenia is one of the most common mental disorders with a high number of disability-adjusted life years. 3 Roughly two-thirds of all patients suffer from a recurrent or chronic course of illness, 4 and about 30% of all patients develop resistance against standard antipsychotic treatment.5–7
More than 65 years after its discovery and more than 30 years after the seminal study by Kane and colleagues, 8 clozapine remains the only effective antipsychotic drug for patients with treatment-resistant schizophrenia (TRS).9–12 Moreover, the superior efficacy of clozapine for crucial clinical aspects of schizophrenia beyond narrowly defined treatment resistance is very well established.13–15 Although these findings are reflected in all major national and international treatment guidelines,16–20 converging evidence from developed countries clearly indicates that clozapine remains substantially underused. 21 It has been suggested that one major reason for this situation is a lack of sufficient training and experience regarding clozapine treatment in a considerable number of psychiatrists.22,23 While specific prescriber-related obstacles remain rather poorly understood, 22 they may include a delayed detection of TRS, incomplete knowledge of clozapine’s broad beneficial effects, and an unfounded hesitance to use or maintain clozapine in accordance with guideline recommendations out of respect for its potential side-effects. 24
Here, we review the current literature on all clinically relevant aspects of clozapine treatment with a particular emphasis on those we deem most pertinent to help rectify these issues. This includes guidance for optimal side-effect monitoring and management geared toward maximizing the number of patients, who can be treated safely with clozapine, while minimizing the overall number of treatment discontinuations. Moreover, by highlighting the current evidence for the full range of its clinical effects, we want to encourage increased use of clozapine not only in TRS but also in other patient groups, for which this unique medication can provide unmatched benefits.
Literature selection
We based our review on a MEDLINE and Google Scholar search for all relevant topics, selecting both relevant individual clinical studies as well as meta-analyses and reviews. We included all articles that were published until November 2022. We searched for publications containing the following MeSH terms: treatment-resistant schizophrenia [AND] criteria, treatment-resistant schizophrenia [AND] treatment, treatment-resistant schizophrenia [AND] neurobiology, clozapine [AND] xx, with xx reflecting the topic we aimed to focus at that timepoint (e.g. side-effects, neutropenia, agranulocytosis, hypersalivation, pneumonia, myocarditis, re-challenge, re-challenge [AND] myocarditis, re-challenge [AND] neutropenia, withdrawal, discontinuation, pregnancy, breastfeeding elderly, metabolic syndrome, gastrointestinal side effects, sedation, mortality, pharmacokinetics, pharmacodynamics, valproate, clinical effects, clozapine-resistant schizophrenia). In addition, we manually screened reference lists of topical review articles. In cases in which we did not have any access to the full article, we contacted the study authors. Literature selection was also informed by our own clinical experience in the use of clozapine.
Treatment-resistant schizophrenia
The international guidelines by the Treatment Response and Resistance in Psychosis (TRRIP) Working Group provide a clear consensus definition of TRS. 25 A central criterion is the presence of persistent symptoms of at least moderate severity despite adequate standard antipsychotic treatment. 25 Importantly, persistent symptoms do not need to cause subjective distress in patients but must have some degree of objectifiable detrimental functional impact. Moreover, pseudo-resistance due to continued use of hallucinogenic drugs or insufficient antipsychotic plasma levels needs to be excluded.25,26 Pseudo-resistance can also result from side-effects or comorbid medical conditions masking the clinical effects of antipsychotic treatment.13,25 In this context, the importance of therapeutic drug monitoring is underscored by evidence from a naturalistic clinical setting indicating that approximately 30% of patients with suspected treatment resistance should in fact be classified as ‘pseudo-resistant’ because of subtherapeutic antipsychotic plasma levels.27–29 Finally, a comprehensive diagnostic workup is essential to rule out other underlying disorders.
The minimal criteria for TRS encompass the following points:
Persistent symptoms (positive, negative, and cognitive symptoms) over at least three months of at least moderate severity causing at least moderate functional impairments. Symptoms classification and thresholds require the use of standardized, validated clinical rating scales.
Insufficient response to treatment with at least two different antipsychotic drugs with a minimum duration of treatment of twelve weeks (six weeks for each drug). This corresponds to a minimum chlorpromazine dose equivalent of 600 mg per day.
Ascertainment of sufficient treatment adherence defined as patients having taken at least 80% of the prescribed doses. To this end, at least two of the following methods need to be employed: counting pills, patient and caregiver report, and chart and record reviews. In addition, blood plasma drug levels should be monitored at least once for each antipsychotic.
In addition to these minimal TRS criteria (Figure 1), which are most relevant for clinical practice, optimal criteria have been proposed, which are geared more toward use in clinical trials. 25

Treatment-resistant schizophrenia.
The neurobiology of treatment resistance
Importantly, in 70–80% of cases, treatment resistance emerges already during the first psychotic episode, highlighting the need for an early detection of this condition.5,6,30,31 Several risk factors for the development of TRS have been identified. These include male sex, living in a less urban area, younger age, family history of psychosis, a high load of schizophrenia risk genes, longer duration of untreated psychosis, substance abuse, and a higher number of relapses due to non-adherence.4,32–34 Obstetric complications, lower premorbid social adjustment, a history of suicide attempts, extended hospitalization, impaired illness insight, and comorbid personality disorders have also been associated with an increased risk for TRS.32,34–36
The exact neurobiological underpinnings of TRS remain elusive. Some authors distinguish between primary and secondary TRS.7,37–40 While primary TRS is present at illness onset, secondary TRS manifests during later stages of the disorder after an initially sufficient response to antipsychotic treatment.7,39,40 Dopaminergic supersensitivity has been discussed as one likely cause of secondary TRS.7,41 Upregulation of striatal postsynaptic dopamine D2 receptors in response to antipsychotic treatment can lead to psychotic exacerbation despite continuous treatment. Consecutive dose increases of antipsychotics can induce further receptor upregulation inducing dopaminergic supersensitivity. In general, serotonin dysregulation and inflammation as well oxidative stress have been proposed to be involved in the pathophysiology of TRS. 7 There is also converging evidence that abnormalities in glutamatergic neurotransmission might contribute to the emergence of treatment resistance, 41 which would also be compatible with the existence of a normodopaminergic subtype of schizophrenia.7,37,38 A higher genetic load for schizophrenia also appears to increase the risk for TRS.7,33,42,43
Clinical effects of clozapine
Unequivocal evidence supports the superior efficacy of clozapine for the reduction of positive symptoms and global psychopathology in TRS compared with other antipsychotics.8,12,44–46 Patients treated with clozapine also show improved treatment adherence 11 and reduced rehospitalization rates.47–52 It is crucial to emphasize that there is no evidence for a comparable efficacy of antipsychotic polypharmacy, that is, the combination of two non-clozapine antipsychotics. 16 Therefore, offering clozapine should always take precedence when treating patients with TRS.
Importantly, the beneficial effects of clozapine go far beyond positive symptoms. Clozapine is among the most effective antipsychotics for improving negative symptoms.14,46,53 It also shows a similar level of efficacy against depressive symptoms, 14 which constitute a common, independent risk factor for suicidality in schizophrenia. 54 Accordingly, clozapine leads to a stronger reduction of both suicidal behavior55–57 and suicide mortality compared with other antipsychotics. 15 Some guidelines therefore explicitly recommend clozapine for persistent suicidality independent of treatment resistance.16–20 Compared with other antipsychotics, clozapine also shows superior efficacy in reducing aggressive and violent behavior.58–62 Furthermore, clozapine lowers the risk of developing a substance use disorder (SUD), 52 and also reduces relapse rates in patients with a comorbid SUD.52,63
Response rates to antipsychotic treatment in drug-naïve patients are estimated at 75%.64,65 Conversely, response rates to a second trial with a standard antipsychotics are considerably lower, ranging between 20% and 45%.64,65 Estimates for overall response rates range between 40% and 60%.66,67 Clinical efficacy of clozapine depends crucially on early treatment initiation.66,68–70 Response rates for treatment initiation within the first 2–3 years after establishing treatment resistance can reach up to 80%.64,66,71 For later treatment initiation, response rates can be as low as 30%. 66 Combined with the clear evidence for a predominantly early onset of treatment resistance, these findings underscore the vital importance of offering and starting clozapine early.
Pharmacodynamics
Clozapine is an antagonist at all dopamine-receptor subtypes (D1–D5). 72 Among them, the antipsychotic effects of clozapine appear to be primarily mediated via D2 receptor antagonism. 73 In this regard, clozapine mirrors other antipsychotics, but its superior efficacy for positive symptoms appears to be the result of additional pharmacological properties. Even after decades of clinical use, the neurobiological mechanisms underlying the broad superior clinical efficacy of clozapine remain elusive. Currently, effects in the glutamatergic74–77 as well as the GABAergic system are discussed as likely explanations.78–80 The pleiotropic effects of clozapine, however, also encompass neurobiological systems not directly related to neurotransmission,37,75,81–83 but their relevance remains unclear.
By comparison, the properties underlying clozapine’s side-effect profile are relatively well established. The nearly complete absence of extrapyramidal symptoms is most likely attributable to rapid dissociation of clozapine from striatal D2-receptors. 84 Antagonism at serotonergic 5HT2C- and 5HT2A-receptors85,86 and at histaminergic H1-receptors is implicated in clozapine-associated weight gain. 85 Antagonism at H1-histaminergic receptors87,88 as well as agonism at gamma-aminobutyric acid (GABA) B receptors have been implicated in sedation. 80 Serotonergic antagonism appears to be involved in clozapine-associated obsessive compulsive symptoms.89,90 Clozapine’s unique muscarinic profile is responsible for several highly relevant side effects. Agonistic effects at M4-receptors are the primary cause of hypersalivation. Conversely, antagonism at M2-receptors is implicated in clozapine-induced gastrointestinal hypomotility (CIGH). Anticholinergic mechanisms might also worsen symptoms associated with cognitive decline, cause delirium, and urinary retention. 91 In addition, clozapine’s antagonistic properties at adrenergic receptors have been linked to nocturnal enuresis, hypotension, and hypersalivation.92,93
Pharmacokinetics and interactions
Clozapine’s half-life is approximately 14 h.94,95 Its metabolism is influenced by several factors including hormones like estrogens, concurrent medication, smoking, 96 sex, with higher blood plasma levels in females,97,98 and age.96,99–102 Ethnicity can also have an effect, with people of Asian descent generally reaching sufficient clozapine plasma levels at lower doses than Caucasians. 100
The following cytochrome P450 (CYP)-enzymes are mainly involved in clozapine metabolism: CYP1A2 (30%), CYP2C19 (24%), CYP3A4 (22%), CYP2C9 (12%), and CYP2D6 (6%). 103 Among them, CYP1A2 induction or inhibition can lead to clinically relevant changes in plasma clozapine levels.94,95 Inhibitors include caffeine, 104 and C-reactive protein (CRP),105–107 which can be triggered by infections. This is underscored by recent reports of toxic plasma clozapine levels during SARS-CoV-2 infections.108,109 Oral contraceptives containing estrogens also inhibit CYP1A2 and CYP2C19 enzyme activity leading to clinically relevant plasma level increases.110,111 Polycyclic aromatic hydrocarbons (PAHs) contained in cigarette smoke are the most relevant CYP1A2 inducers.112,113 Importantly, after abrupt smoking cessation, enzyme activity typically normalizes within three days, 112 which can lead to toxic plasma clozapine levels.113–121 Notably, nicotine patches and e-cigarettes are not associated with a comparable interaction risk.28,122–125
Optimal plasma clozapine levels for the treatment of TRS fall in the range of 350–600 µg/L.126,127 Plasma clozapine levels above 600 µg/L increase the risk for side-effects considerably. 128 Plasma clozapine levels above 1000 µg/L are considered toxic, are associated with an at least two-fold increase in mortality risk, 129 and require immediate dose reduction and intensified pharmacovigilance. Plasma clozapine levels above 2000 µg/L are acutely life-threatening.130,131 Notably, clozapine intoxication is associated with a delayed plasma peak due to clozapine’s extensive enterohepatic circulation and its induction of gastrointestinal hypomotility. 132 In general, international guidelines strongly recommend regular monitoring of plasma clozapine levels to increase both patient safety and response rates.28,29
In rare cases, rapid metabolism of clozapine due to yet unknown causes may preclude reaching sufficient plasma clozapine levels.133–135 Here, augmentation with low doses of fluvoxamine, a strong CYP1A2 inhibitor, should be considered.136–138 A total of 25–50 mg of fluvoxamine can raise plasma clozapine levels five- to ten-fold within 2–4 weeks139–141 and also triple clozapine’s half-life. 142 Consequently, frequent screening for side effects and therapeutic drug monitoring are crucial during augmentation with fluvoxamine.28,29
In summary, there are several relevant pharmacokinetic and pharmacodynamic interactions clinicians need to be aware of (Tables 1 and 2). When addressing such interactions, switching to safer alternatives for interacting drugs wherever possible should be the primary strategy. Discontinuation of clozapine should only be considered as a last resort.
Pharmacokinetic interactions.

CYP, cytochrome P450; PAH, polycyclic aromatic hydrocarbon.
Pharmacodynamic interactions.

ACE, angiotensin-converting enzyme.
Clozapine metabolites
Clozapine is mainly demethylated to n-desmethylclozapine (norclozapine) and oxidized to clozapine-n-oxide. 95 In contrast to clozapine-n-oxide, norclozapine is pharmacologically active. Compared with clozapine, norclozapine shows diverging effects on dopaminergic and muscarinic receptors98,160 and also affects serotonergic receptors among others.161–164 While it has no antipsychotic properties, norclozapine appears to contribute to the overall side-effect burden including sedation, hypersalivation, constipation, metabolic complications, and seizures. 163
Recently, the clozapine:norclozapine ratio has received growing attention.98,136,165 Based on clinical observations, the optimal clozapine: norclozapine ratio is deemed to be around two. Higher values are indicative of a non-trough blood sample, a recently missed dose, or decreased CYP1A2 enzyme activity. Lower values appear to be indicative of increased CYP1A2 enzyme activity.136,165,166 Other authors, however, recommend using the total clozapine C/D ratio, with C representing the sum of the clozapine and norclozapine trough steady-state plasma concentration and D representing the daily dose of clozapine. 98
Side effects of clozapine
Owing to the relatively high side-effect burden associated with clozapine (Figure 2 and Table 3), extensive pharmacovigilance as well as early and consistent management of side-effects are of particular importance. 167 Frequent consultation of both patients and their families is an important element of this strategy. 101 In addition to clozapine’s broad antagonistic and agonistic effects on key neurotransmitter systems outlined above, immunomodulatory effects, which might partly explain clozapine’s unique efficacy, have also been implicated in adverse drug reactions (ADRs) including eosinophilia, myocarditis, pancreatitis, and nephritis. 167 Side-effect risk decreases with slower initial dose titration regimes. 101 This is particularly important in light of evidence for an association between rapid initial dose escalation and risk for both myocarditis and neutropenia. 92 Owing to the clear dose dependency of some side effects (Table 3), dose reductions should be attempted first whenever feasible before considering other options. 101

Clozapine-associated side effects.
Management of clozapine-associated side effects.
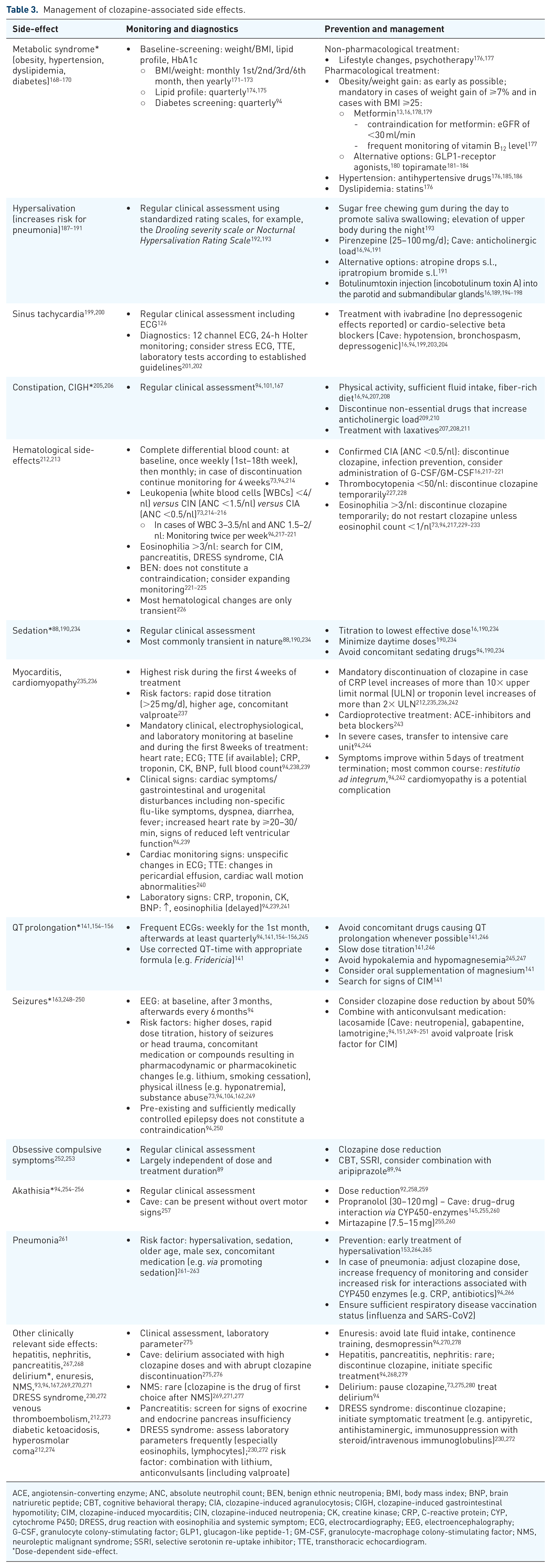
ACE, angiotensin-converting enzyme; ANC, absolute neutrophil count; BEN, benign ethnic neutropenia; BMI, body mass index; BNP, brain natriuretic peptide; CBT, cognitive behavioral therapy; CIA, clozapine-induced agranulocytosis; CIGH, clozapine-induced gastrointestinal hypomotility; CIM, clozapine-induced myocarditis; CIN, clozapine-induced neutropenia; CK, creatine kinase; CRP, C-reactive protein; CYP, cytochrome P450; DRESS, drug reaction with eosinophilia and systemic symptom; ECG, electrocardiography; EEG, electroencephalography; G-CSF, granulocyte colony-stimulating factor; GLP1, glucagon-like peptide-1; GM-CSF, granulocyte-macrophage colony-stimulating factor; NMS, neuroleptic malignant syndrome; SSRI, selective serotonin re-uptake inhibitor; TTE, transthoracic echocardiogram.
Dose-dependent side-effect.
Hematological side effects
Not least for historic reasons, 281 clozapine is closely associated with agranulocytosis and other, less serious forms of neutropenia. An absolute neutrophil count (ANC) of 1–1.5/nl is referred to as mild neutropenia while ANCs of 0.5–1.0/nl are referred to as moderate neutropenia. ANCs of <0.5/nl constitute severe neutropenia. 282 ANCs below 0.5/nl are also typically referred to as agranulocytosis.215,283,284 However, strictly speaking agranulocytosis requires near absence of neutrophils, that is, ANCs below 0.1/nl.283,285 The clinical syndrome of agranulocytosis is commonly associated with a triad of symptoms encompassing fever, mouth ulcers, and sore throat. 215 Pragmatically equivalating severe neutropenia and agranulocytosis is motivated by the substantial risk for opportunistic infections associated with ANCs below 0.5/nl, 215 which triggers several clinical actions discussed in detail below. For pragmatic purposes, we will therefore likewise refer to ANCs of 1.5–0.5/nl as clozapine-induced neutropenia (CIN) and to ANCs of <0.5/nl as clozapine-induced agranulocytosis (CIA).
Owing to an increased risk for CIN and CIA, frequent blood cell counts are mandatory throughout treatment.212,281,286 This procedure has reduced risk of death from CIA to less than 1 in 10,000 patients. 238 Risk for CIN and CIA is estimated to be 3% and 0.4–0.7%, respectively.217,287 Although CIN or CIA can occur at any time during treatment,288,289 the highest incidence rates have been observed during the first 6–18 weeks of treatment (49% cases of neutropenia, 82% cases of agranulocytosis) with a clear subsequent risk decrease after six months.73,213,217,287,290 This should be considered when a comorbid somatic disorder necessitates treatment with a drug also linked to blood dyscrasia. Whenever possible, treatment with such drugs should be initiated after the critical first six months. 213
Currently, safety thresholds for neutrophil counts during clozapine treatment vary slightly across health systems. Importantly, discontinuation should require clear evidence for a downward dynamic of the neutrophil count,219,220,291 as cases of transient neutropenia under clozapine treatment have also been observed. 292 Moreover, an immediate thorough search for other causes of blood dyscrasia is essential, as this would have important implications for a potential re-challenge of clozapine.217,218,287 Important causes include concomitant medication – including antibiotics273,293 and psychotropic compounds like carbamazepine and valproate294,295 – or viral infections. 296
Confirmed CIN and CIA stipulate immediate discontinuation of clozapine. In addition, CIA requires the administration of granulocyte colony-stimulating factor (G-CSF). Moreover, further actions to prevent and treat infections, for example, administration of antibiotics and protective isolation, might be necessary.297–299
In cases of mild neutropenia even before treatment onset, benign ethnic neutropenia (BEN) is an important differential diagnosis, which does not constitute a contraindication.221–225 Safety thresholds for patients with a confirmed diagnosis of BEN are lower (Figure 3(a) and Table 3). 300 Pseudo-neutropenia resulting from physiologically reduced neutrophil counts due to higher cortisol levels in the morning should also be considered. 217
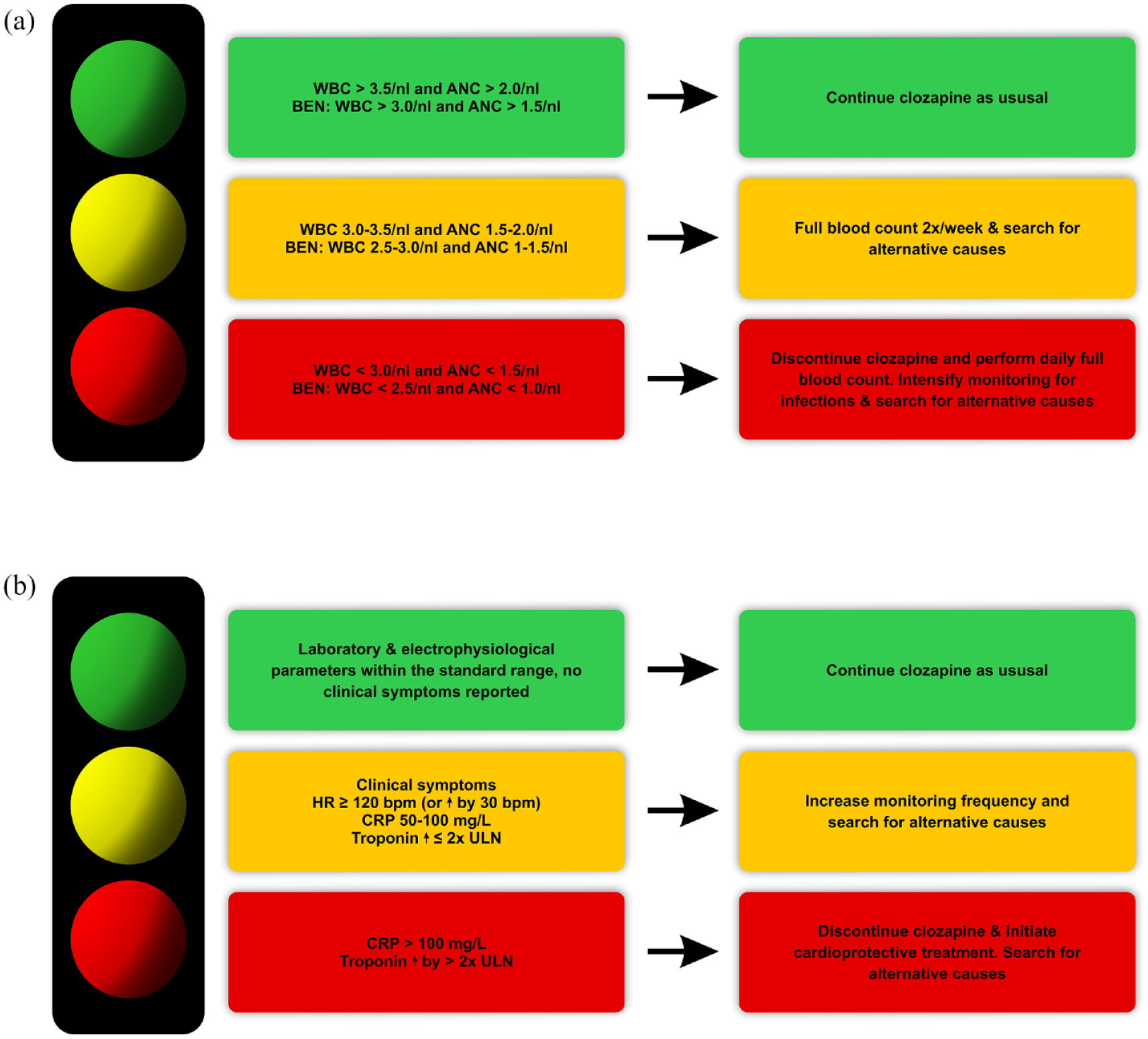
Screening and management of clozapine-induced neutropenia (CIN) and clozapine-induced myocarditis (CIM). (a) Color code categorization of CIN screening parameters and required action. Absolute neutrophil counts within the green range do not require any action except regular monitoring. ANCs within the yellow range require intensified full blood monitoring and searching for an alternative cause. ANCs within the red range necessitate immediate discontinuation of clozapine, daily monitoring of full blood count, and searching for an alternative cause. (b) Color code to categorization of CIM screening parameters and required action. Results within the green range do not require any action except regular monitoring. Results within the yellow range require intensified monitoring and searching for an alternative cause. Results within the red range necessitate immediate discontinuation of clozapine, daily monitoring, initiation of cardioprotective treatment, and searching for an alternative cause.
The pathophysiology of CIN and CIA remains poorly understood, but an autoimmune mechanism appears most likely. Eosinophilia is another important but rare hematological side effect. Importantly, eosinophilia does not warrant permanent discontinuation of clozapine.212,301 Treatment can be restarted at eosinophil counts below 1/nl. Eosinophilia, however, should prompt a search for other clozapine-induced ADRs including CIA, clozapine-induced myocarditis (CIM), pancreatitis, and drug reaction with eosinophilia and systemic symptom (DRESS) syndrome.227,302
Notably, a recent longitudinal study revealed an increased risk for hematological malignancies in patients receiving clozapine. 303 This risk, however, is smaller than the reduction of all-cause mortality associated with clozapine. Moreover, mortality rates in clozapine users diagnosed with a hematological malignancy were lower compared with patients treated with nonclozapine antipsychotics.303–305 Therefore, while these findings necessitate increased vigilance regarding signs of hematological malignancy in clozapine users, they do not undermine the general case for clozapine.304,305
Cardiac side effects
CIM is among the most important and yet underdiagnosed side effects. CIM risk is the highest during the first 4 weeks after treatment initiation,306,157 but also during re-exposure following a first successful trial. 94 Moreover, rare cases of CIM after long-term treatment of more than a decade have also been observed.73,307,308 Compared with CIN and CIA, the incidence of CIM is noticeably higher.157,309 The timely detection of CIM might be impeded by its often unspecific clinical presentation, which can include flu-like symptoms like fever, dyspnea, myalgia, and vague complaints of fatigue and malaise.242,309,310 Patients might also experience symptoms reflecting cardiac involvement such as chest pain, hypotension, palpitation, tachycardia, and peripheral edema.242,309,310 These more specific symptoms, however, are by no means mandatory. By contrast, there have been reports of cases solely presenting with gastrointestinal and urogenital disturbances like diarrhea, dysuria, and vomiting.241,242,310,311 Hence, frequent screening for clinical, electrophysiological, and laboratory signs of CIM is mandatory.94,147,167,241 Electrocardiographic (ECG) findings in CIM are characterized by non-specific alterations such as T-wave inversion and ST elevation or depression.242,312 Transthoracic echocardiogram (TTE) might reveal left ventricular impairments and pericardial effusion, while cardiac magnetic resonance imaging (MRI) can provide more direct evidence for myocardial inflammation.240,313 In addition, endomyocardial biopsy can be performed to rule out viral myocarditis. 314 Mandatory laboratory screening at baseline and during the first 8 weeks of treatment encompasses troponin, CRP, creatine kinase (CK), and brain natriuretic peptide (BNP)13,242,310,312,315 are highly sensitive markers for CIM.
Importantly, while monitoring of clinical symptoms is important to inform CIM diagnosis, confirmation of a suspected CIM should rely primarily on objective parameters, that is, laboratory parameters exceeding pre-specified thresholds (Figure 3(b) and Table 3), to prevent premature and unnecessary discontinuation but also to ensure patient safety in cases of unspecific clinical symptoms. 310 Clearly established CIM necessitates immediate termination of clozapine,246,310 strict avoidance of major physical activity, 244 and initiation of a cardioprotective pharmacotherapy with a beta-blocker and an angiotensin-converting enzyme (ACE) inhibitor.73,241,242,246,316 Serious cases of CIM might require treatment in an intensive care unit.4,244,317 Severe outcomes of CIM – typically as a consequence of delayed or missed diagnosis and treatment 318 – include ventricular arrhythmia, persistent heart failure, and sudden death.158,244,246,312 Importantly, early intervention increases the chance for a restitutio ad integrum, 242 underscoring the relevance of CIM screening during the initial titration of clozapine. 318
Based on its early onset and titration speed dependency, a hypersensitivity reaction is discussed as a likely pathophysiological mechanism of CIM,235,244,246,319–323 but current evidence remains inconclusive. 157 Thus far, no reliable predictors for an individual’s CIM risk have been established. Several risk factors for CIM, however, have been identified, 157 chiefly among them concurrent treatment with valproate.157,237,324 Consequently, valproate should not be prescribed concurrently with clozapine, neither for treatment of any residual psychopathology nor for seizures. There is also preclinical and clinical evidence that rapid titration increases the risk of CIM.237,319,325 This suggests that people with slow clozapine metabolism might be at a higher risk for CIM. Higher age and higher clozapine doses also appear to constitute risk factors.157,326
Cardiomyopathy constitutes another potential cardiac side effect with reported incidence rates ranging between 0.02% and 1%.215,222 Importantly, undetected and self-limiting myocarditis has been implicated as a likely cause.198,215,222 Hence, prevention and adequate management of CIM might also reduce the risk of clozapine-associated cardiomyopathy.
Gastrointestinal side effects
The most common gastrointestinal side-effect is constipation, which occurs in up to 60% of patients.327–329 Furthermore, at least 50% of patients show unambiguous evidence of CIGH in colonic transit studies. 327 Potentially severe consequences of CIGH include dysphagia, ileus, intestinal obstruction, bowel ischemia, and megacolon,328,329 which are associated with a considerable mortality rate. 330 Importantly, the prevalence of CIGH is markedly higher than the prevalence of CIM and CIA.329,331 CIGH arises primarily due to the anticholinergic and antiserotonergic effects of clozapine 176 and shows a clear dose dependence.167,327 Polypharmacy, which adds to clozapine’s inherent anticholinergic load or otherwise affects gastrointestinal motility, constitutes a risk factor for CIGH.209,210 As a first step, prevention and management of CIGH requires lifestyle and dietary modifications, that is, physical exercise, sufficient fluid intake, and fiber supplementation. As a second-line approach, current guidelines recommend specific pharmacological treatment including laxatives (first line: osmotic laxatives, second line: stimulant laxatives), prosecretory agents, and serotonergic agonists.207,208,211
Metabolic side effects
Irrespective of medication, patients with schizophrenia have an increased risk for developing a metabolic syndrome, encompassing hypertension, dyslipidemia, obesity, and diabetes.168–170 For clozapine, the prevalence of metabolic syndrome is estimated to be approximately 50%.332,333 Weight gain represents a crucial risk factor for developing metabolic syndrome 334 and an important psychological stressor.177,335–337 Moreover, it reduces quality of life, 335 treatment adherence,337,338 and contributes to cognitive dysfunction.339–341 Importantly, weight gain typically occurs during the early stages of antipsychotic treatment.342,343 More than two-thirds of patients show a gain of more than 7% of their baseline weight during the first year of treatment.177,344,345 This underscores the necessity of frequent monitoring of body weight and metabolic parameters and of early weight-stabilizing interventions (Table 4).333,346 Regular physical exercise, a Mediterranean diet, and smoking cessation to decrease cardiovascular risk are the primary recommendations to counteract weight gain.226,347 Among pharmacological interventions, adjunctive metformin shows a good safety profile and the best efficacy for stabilizing weight gain.177,178,348,349 Consequently, the first guideline for metformin use during antipsychotic treatment advocates a routine early initiation in addition to behavioral interventions to most effectively minimize weight gain and cardiometabolic risk. 177 On average, treatment with metformin leads to a weight loss of about 3.2 kg. As the feasibility of reversing weight gain remains limited, weight stabilization should be the primary goal. The recommended daily dose of metformin is 2000 mg when tolerable. Gastrointestinal issues such as nausea, diarrhea and vomiting as well as lactic acidosis are the most relevant side effects. Before and during treatment with metformin, renal function and vitamin B12 level should be monitored routinely.
Management of clozapine-resistant schizophrenia.

CBT, cognitive behavioral therapy; ECT, electroconvulsive therapy; SSRI, selective serotonin re-uptake inhibitor.
More recent findings indicate that glucagon-like peptide-1 (GLP1) receptor agonists could also be effective for mitigating clozapine-associated metabolic comorbidity. 180 Topiramate can also be considered as its efficacy appears to be comparable with metformin.181–184,352 Recently, samidorphan – an opioid receptor antagonist – was introduced as an adjunctive treatment for olanzapine-associated weight gain.353,354 This might be also a promising approach for clozapine.
Treatment of manifest diabetes in patients treated with clozapine should closely follow current guidelines including the use of insulin when indicated.355,356 Adequate antidiabetic treatment substantially reduces cardiovascular risk and the risk for ketoacidosis or hyperosmolar coma. 274 Importantly, pre-existing diabetes mellitus in patients with TRS does not constitute a contraindication for clozapine treatment, 357 but rather requires intensified antidiabetic treatment. This is underscored by converging findings indicating that, for clozapine, the risk for diabetes is not excessive compared with second-generation antipsychotics as a whole, but rather falls in the higher range within this class of drugs.343,358 In conclusion, it needs to be emphasized that strict management of metabolic side effects can notably improve the associated cardiovascular risk factors 359 and that overall clozapine treatment is actually associated with a relevant reduction of cardiovascular mortality.15,46
Hypersalivation and pneumonia
Clozapine-induced hypersalivation (CIH) constitutes a frequent side-effect with incidence rates ranging between 30% and 92%, which typically occurs early during treatment and shows no clear dose dependence.187,360 Agonism at muscarinic M4 receptors and antagonism at α2-adrenergic receptors have primarily been implicated in its etiology.188,361,362 Predominantly, patients report nightly hypersalivation. 187 CIH can cause psychological distress due to embarrassment and social stigma, as well as lead to somatic adverse events like skin irritation, parotitis, and aspiration pneumonia.73,194 Management of CIH commonly requires early pharmacological intervention, usually with anticholinergic, that is, antimuscarinic, drugs. Evidence for their efficacy remains limited, however. Moreover, systemically acting drugs such as pirenzepine increase the overall anticholinergic load, raising the risk for CIGH.209,210,363 Sublingual administration of atropine eye drops73,364,365 and regular botulinum toxin injections into the parotid and submandibular glands can avoid this problem.195,366 Before recommending treatment with sublingual atropine eye drops, prescribers need to ensure that patients can adequately follow instructions regarding the finely dosed topical application to prevent accidental ingestion of relevant amounts of fluid. Importantly, CIH increases the risk of clozapine-associated pneumonia via salivary aspiration. 367 In this context, it is crucial to acknowledge the higher mortality rates of patients with schizophrenia due to pneumonia and increased rates for additional pulmonary diseases including chronic obstructive pulmonary disease. 368 Importantly, pneumonia elevates CRP levels, thus decreasing CYP1A2 enzyme activity and increasing plasma clozapine levels.105,369–372 This underscores the necessity for preventive measures for clozapine-associated pneumonia. Furthermore, health care professionals should ensure a sufficient vaccination status of their patients for respiratory diseases including COVID-19 and influenza in order to reduce mortality rates.368,373
Sedation
Clozapine-induced sedation (CIS) ranks among the most commonly reported side-effects.189,374–376 It shows a clear dose dependence, but is often at least partly transient.88,190,234,377 Importantly, while there are established protocols regarding other important side-effects, data regarding the management of CIS remain limited, despite the relevance of CIS as a key determinant of treatment adherence.80,87,88,189,234 Management of CIS should start with patient education about its potentially transient nature 190 and about healthy habits regarding sleep hygiene. 190 It also includes minimizing daytime clozapine administration, avoiding concomitant sedating drugs and clozapine dose reduction whenever possible.190,234,378 Importantly, recent findings indicate that clozapine administration partly during daytime may not reduce the burden of sedation. 379 Emphasizing nocturnal administration whenever possible while taking into account individual preferences appears to be more promising also given that complex dosing instructions might be too demanding for some patients. 379 Adding aripiprazole constitutes another option.88,378 Augmentation with modafinil has also been discussed, but findings from a placebo-controlled pilot trial were not generally supportive.73,380 Furthermore, there are reports indicating a pharmacokinetic interaction between clozapine and modafinil, which could lead to a considerable increase of clozapine plasma levels. 381
Discontinuation and re-challenge of clozapine
Managing discontinuation
Approximately 30–40% of patients discontinue clozapine over the course of treatment, 382 mainly because of side effects, non-compliance to monitoring protocols or patient preference.234,383 Both immediate and gradual clozapine termination can result in withdrawal symptoms, especially cholinergic and serotonergic discontinuation syndrome.276,384–387
Cholinergic rebound symptoms observed in up to 50% of cases include agitation, delirium, and hallucinations, 386 vomiting, diarrhea, headache, diaphoresis, dystonia, and dyskinesia.384,385,388 Clinical management includes supportive care and treatment with anticholinergic compounds. 386 Serotonergic rebound symptoms comprise agitation, diaphoresis, clonus, and hyperreflexia. In addition to supportive care, termination of concomitant serotonergic medication might be indicated as well as short-term use of cyproheptadine for moderate and severe cases. 385 Current evidence supports olanzapine as well as risperidone and long-acting aripiprazole as the best alternative options,389,390 but without matching the efficacy of a clozapine re-challenge.391–393
Hence, discontinuation of clozapine often leads to a considerable worsening of psychopathology with potentially severe short- and long-term clinical and functional consequences.217,389,390,394–396 While withdrawal symptoms also contribute to this deterioration, supersensitivity mechanisms397–401 and a lack of sufficiently effective alternative antipsychotics are regarded as the main causes. 384 Catatonia and persistent psychotic exacerbation are the most common sequelae.386,397,402 Here, benzodiazepines and electroconvulsive therapy (ECT) constitute crucial treatment options.402–404 There is no evidence for a sufficient medium- and long-term efficacy of ECT without clozapine in most patients with TRS, however.395,405
Based on these findings, current guidelines strongly recommend a hyperbolic discontinuation regime, if discontinuation is inevitable.217,385,406 Immediate termination of clozapine should be limited to potentially life-threatening side effects including agranulocytosis, myocarditis, ileus or subileus, neuroleptic malignant syndrome (NMS), venous thromboembolism, and diabetic ketoacidosis or hyperosmolar coma. 217 Most importantly, because of the complications outlined above and its superior efficacy, permanent discontinuation of clozapine should be avoided whenever possible.217,221
Rather, the singular status of clozapine underscores the importance to seriously consider a re-challenge even after severe side-effects. This notion is supported by a growing body of evidence for a positive risk–benefit ratio and considerable success rates for clozapine re-challenges after neutropenia,217,395 NMS, 407 and to a lesser extent myocarditis.224,408,409 Any re-challenge must only be attempted in an appropriate hospital setting with sufficient support by relevant specialists, that is, cardiologists or hematologists.224,410
Re-challenge after neutropenia
Current evidence clearly argues against a re-challenge after CIA.269,407 After CIN, a re-challenge based on a strict risk–benefit assessment is considered to be a reasonable clinical option. 407 Importantly, time of onset of CIN during a re-challenge is typically shorter. 411 In general, a slower re-titration rate of clozapine might reduce risk of re-occurrence of CIN. 221 Based on published cases, the success rate is estimated at about 66%. 407 Current evidence indicates that concomitant treatment with lithium markedly increases success rates.269,412,413 Plasma lithium levels above 0.4 mmol/L have consistently been associated with increased neutrophil counts, most likely due to bone marrow induction.269,414–416 Lithium treatment should be initiated at least two weeks prior to a clozapine re-challenge and maintained long-term, 217 because its discontinuation increases the risk for a re-occurrence of blood dyscrasia. 412 While it is overall considered to be safe, concomitant treatment with clozapine and lithium can markedly decrease the seizure threshold.151,417,418
Treatment with G-CSF is an alternative approach, which increases re-challenge success rates.287,291,419,420 To this end, G-CSF can be administered on a regular prophylactic basis during a re-challenge irrespective of current absolute neutrophil count (ANC). 421 Alternatively, G-CSF can be administered on an as-required basis in the event of predefined neutrophil counts to maintain clozapine treatment. Current evidence indicates that both approaches are safe and effective. 421 Importantly, currently available evidence indicates that long-term use of G-CSF is not associated with significant morbidity in other patient populations. 422 Therefore, such a strategy has been proposed for patients in which discontinuation of G-CSF results in recurrent neutropenia. 421 Long-term safety and efficacy data are currently lacking, however.419,421,423–426
To summarize, lithium can be suitable for persistent forms of mild neutropenia, while more severe forms of neutropenia require the use of G-CSF.
Re-challenge after myocarditis
At present, there are no established consensus guidelines for re-challenges after CIM, but rather protocols based on case series.243,309,315,407,410,427–431 Importantly, a re-challenge should only be attempted after patients have made a full recovery from CIM. 427 It requires intensive clinical, laboratory and electrophysiological (ECG, TTE) monitoring (e.g. every second to third day) and very slow dose titration (e.g. 12.5–25 mg per week),243,408–410,427,432 which reduces CIM recidivism risk.315,427 Re-challenge success rates after CIM are currently estimated at approximately 60%, 431 but with a high degree of uncertainty. Notably, compared with re-challenges after CIN, the number of published cases is an order of a magnitude lower. 407 Therefore, re-challenges after CIM must not be regarded as a routine procedure and warrant exceptional caution.
Pregnancy and breastfeeding
A switch from a non-clozapine antipsychotic to clozapine might increase fertility as a result of alleviated hyperprolactinemia and amenorrhea. 73 Currently, there is no evidence for a reduced safety of clozapine for pregnant women. 433 Several side-effects, however, may be exacerbated including weight gain, constipation, sedation, and orthostatic hypotension. 434 Close monitoring for emerging gestational diabetes is therefore mandatory.435,436 Notably, CYP1A2 enzyme activity decreases by approximately 33% during the first trimester and by approximately 65% during the last trimester. 437 This necessitates monthly monitoring of plasma clozapine levels throughout pregnancy, repeated a week after delivery. 73
To date, there is no conclusive evidence for detrimental neurodevelopmental and cognitive long-term effects resulting from fetal exposure to clozapine.434,438–440 Clozapine is not associated with greater teratogenic effects than other antipsychotics.440–442 Furthermore, there is no evidence for increased rates of prematurity, delivery complications, or changes in birth weight and height compared with other antipsychotics. 434 Given its unique efficacy for TRS, for the majority of pregnant women receiving clozapine, switching to another antipsychotic is not a feasible option.434,436 In most cases, the considerable risk for illness exacerbation associated with such a switch outweighs the risks associated with continued clozapine treatment during pregnancy.436,439 Therefore, a thorough risk–benefit assessment is indispensable before any treatment change. Using the lowest effective dose of clozapine is especially crucial during pregnancy, however.73,433,434,436,438 Furthermore, frequent gynecological consultations and antenatal screenings should be encouraged and supported.73,433,434,436,438
The level of clozapine excretion into breast milk is considerable.436,438 Owing to insufficient short- and long-term safety data, breastfeeding during clozapine treatment should therefore be avoided. 434
Clozapine treatment in the elderly
There are a number of changes in the pharmacokinetics and pharmacodynamics of clozapine in elderly patients, which warrant particular caution including lower maintenance doses.73,443,444 Rates of CIA, CIMs, seizures, and metabolic syndrome increase in older patients.445–447 The anticholinergic properties of clozapine may increase the risk for cognitive decline. 91 Overall, clozapine appears to be both safe and effective in the majority of elderly people when adhering to very low dose titrations and providing increased pharmacovigilance. 443
Management of clozapine-resistant schizophrenia
The markedly delayed onset of its full therapeutic effect is a unique characteristic of clozapine, which appears to be only partly attributable to the necessarily slow initial dose titration.79,448 Consequently, the current TRRIP consensus guidelines strongly recommend deferring treatment evaluation in accordance with the main target symptoms while also ensuring a plasma clozapine level above 350 µg/L (Table 4). 350 For predominant positive and mixed (both negative and positive symptoms) symptoms, treatment evaluation after three months is considered to be adequate. 350 For negative and cognitive symptoms, an evaluation after four months is recommended, while eight weeks are deemed appropriate for aggression and suicidality. 350
About 40% of patients show an insufficient response to clozapine despite clozapine plasma levels within the recommended range.25,67,350 These cases are classified as ultra-treatment-resistant or clozapine-resistant schizophrenia (CRS). 25 A high genetic load for schizophrenia appears to increase the risk for a poor treatment response.33,449 Compared with TRS, CRS is characterized by later clozapine initiation and associated with higher mortality rates.127,350 Importantly, clozapine should not be discontinued in patients with CRS, but rather augmented (Table 3).127,350 For predominant positive symptoms, recommended augmentation strategies include a combination with amisulpride or aripiprazole as well as ECT.350,351 Furthermore, while there is no evidence for clinically meaningful symptom improvements produced by cognitive behavioral therapy (CBT) in CRS, pragmatic individual trials might still be indicated. 450
Impact on mortality
Despite its side-effect burden and its detrimental influence on metabolic parameters in particular, clozapine reduces not only suicide mortality but also all-cause mortality to a greater degree than any other oral antipsychotic. Its positive effects on cardiovascular mortality – while less pronounced – are nonetheless comparable with other antipsychotics.15,46,451 Clozapine’s mortality reducing effects are likely attributable to its superior efficacy regarding positive symptoms and suicidality, to improved treatment adherence and relapse rates, 46 as well as to mitigating the increased mortality risk associated with comorbid SUDs. 452 Consequently, the likelihood of an adequate diagnosis and treatment of somatic comorbidities should also increase. 453 This might also be facilitated partly by the stricter pharmacovigilance regime required for clozapine. In light of the high rates of somatic comorbidities and the considerable overall increased mortality rates in people with schizophrenia,454,455 these findings constitute another crucial argument in favor of a broader use of clozapine while also underscoring its safety. 456
Clinical implications
The singular extent of clozapine’s efficacy outlined above has important clinical implications for the treatment of schizophrenia. First and foremost, existing clinical and neurobiological lines of evidence provide little to no reason to be reluctant regarding clozapine use. Consequently, clozapine must never be regarded as an antipsychotic of ‘last resort’ but rather the drug of choice for patients nonresponsive to first-line treatment and more generally for patients with an emerging unfavorable course of illness. 457 In this regard, stringent use of TRS criteria and close adherence to current recommendations provide excellent guidance for clinical decision-making. The high rates of treatment resistance in first-episode patients underscore the need for early recognition and treatment of TRS.
Slow dose titration is essential to avoid titration-related side effects including sedation, myocarditis, and neutropenia. To this end, dose titration rates of 12.5 mg per day or less during the initial weeks of treatment should be seriously considered. Systematic pharmacovigilance and a timely management of ADRs are very feasible and also among the most important elements of a successful treatment strategy. Furthermore, clozapine might be essential when aiming to address substance abuse and sufficient treatment of somatic comorbidities. Even major pre-existing problems in these areas should not automatically be regarded as obstacles for offering clozapine. 458 After clozapine initiation, clinicians should exhaust every reasonable option to minimize permanent all-cause discontinuation. This includes carefully re-challenging patients even after serious adverse events like myocarditis and neutropenia. Furthermore, treatment algorithms involving clozapine can and should be very simple. Clozapine use is key for reducing antipsychotic polypharmacy and the associated side-effect burden. 459 Accordingly, clozapine should always first be used as an antipsychotic monotherapy in both TRS and non-TRS patients. For persistent positive symptoms despite adequate clozapine use, augmentation with an appropriate second antipsychotic should be the first treatment escalation (Table 4), before offering ECT as a second treatment escalation step. Finally, clozapine use requires a long-term approach acknowledging the late onset of clozapine’s full effects. In this context, clinicians also need to be mindful of the fact that some key benefits like reduced suicidality and mortality rates may be next to invisible.
Conclusion
Underutilization and delayed initiation of clozapine regardless of the continuously mounting evidence and contrary to all recommendations remain a major concern. This underscores the urgent need for intensified research into the real and perceived barriers for clozapine treatment, continued education of psychiatrists, and appropriate structural adjustments of routine clinical care. These efforts are justified not least by the very high patient satisfaction with clozapine despite the considerable complexity of its use and its potential side effects.10,286,460 Most importantly however, they are imperative because – going into the sixth decade of its clinical use – compared with all other available pharmacological treatment options, the broad beneficial impact of clozapine on patients’ life remains second to none.