
Abstract
Posttraumatic stress disorder (PTSD) is a devastating condition, for which there are few pharmacological agents, often with a delayed onset of action and poor efficacy. Trauma-focused psychotherapies are further limited by few trained providers and low patient engagement. This frequently results in disease chronicity as well as psychiatric and medical comorbidity, with considerable negative impact on quality of life. As such, off-label interventions are commonly used for PTSD, particularly in chronic refractory cases. Ketamine, an N-methyl-D-aspartate (NDMA) receptor antagonist, has recently been indicated for major depression, exhibiting rapid and robust antidepressant effects. It also shows transdiagnostic potential for an array of psychiatric disorders. Here, we synthesize clinical evidence on ketamine in PTSD, spanning case reports, chart reviews, open-label studies, and randomized trials. Overall, there is high heterogeneity in clinical presentation and pharmacological approach, yet encouraging signals of therapeutic safety, efficacy, and durability. Avenues for future research are discussed.
Keywords
Introduction
Posttraumatic stress disorder (PTSD) is a chronic and disabling mental illness, with immeasurable socioeconomic burden. 1 It has a cross-national lifetime prevalence of 3.9% in the general population, and 5.9% among the trauma exposed, varying significantly across countries and income groups. 2 Veterans and active-duty military, 3 as well as first responders, 4 are among those with the highest rates of PTSD. Indigenous People of the Americas, with shared Paleoamerican origins, are likewise disproportionately affected, carrying 1.4 greater odds of lifetime prevalence. 5
While clinical manifestations vary, PTSD is characterized by aberrant adaptations to trauma exposure, involving four symptom clusters: intrusive thoughts, stimuli avoidance, negative affect, and autonomic arousal. 6 These limit one’s ability to maintain employment and social relationships, leading to functional and psychosocial impairment, with considerable negative impact on quality of life. Moreover, several pre- and peri-trauma risk factors are known to contribute to the development and maintenance of PTSD, such as childhood adversity and trauma severity. 7 This is further complicated by psychiatric comorbidity. According to the Adult Psychiatric Morbidity Survey, 78.5% of those with PTSD meet diagnostic criteria for at least one other mental illness, most commonly major depressive disorder (MDD) (⩽53.6%).8,9 Depressive and anxiety disorders, in addition to alcohol and substance abuse, are specifically 2–4 times more prevalent among sufferers, 10 the latter dependencies often used to self-medicate.
The primary care pathway for PTSD is psychotherapy followed by pharmacotherapy, or a combination of both. To date, only two medications are approved by the Food and Drug Administration (FDA) for the treatment of PTSD, sertraline and paroxetine, both of which are selective serotonin reuptake inhibitors (SSRIs). Despite their effectiveness for a minority few, these therapeutics have critical limitations. 11 Even when delivered under optimal conditions, up to 60% of patients do not respond to SSRIs, less than 30% achieve remission, and many experience adverse reactions prior to clinical benefit.12–15 This frequently results in polypharmacy and/or early discontinuation. Furthermore, as slow-acting antidepressants (SAADs), there is a notable latency period associated with SSRIs, comprising up to 12 weeks of therapeutic lag time. 16 Such limitations in efficacy and onset of action shown in SSRI treatment have been termed as ‘PTSD pharmacotherapy crisis’, 17 significantly increasing the risk for suicide and self-harm,18,19 particularly during the first 7–9 days of use.
Given the shortcomings of traditionally available medications, trauma-focused psychotherapies are designated as first-line treatments in PTSD practice guidelines,20,21 including prolonged exposure (PE) and cognitive processing therapy (CPT). These interventions are supported by a large evidence base, targeting fear memory reconsolidation and extinction, as well as cognitive distortions that may contribute to symptom maintenance. However, treatment access and patient engagement remain low, 22 even within the Veterans Healthcare Administration (VHA).23,24 A recent trial evaluating the comparative effectiveness of PE and CPT found attrition rates of 55.8% and 46.6%, respectively, among veterans with PTSD. 25 Likewise, a large proportion (~50%) of patients engaged in treatment fail to respond, 26 one-third of which remain symptomatic 10 years post-trauma exposure. 4 Novel therapeutics offering rapid and robust improvements are therefore desperately needed, especially for chronic refractory cases.
Ketamine, initially FDA-approved as a general anesthetic in 1970, 27 is a non-competitive channel blocker of N-methyl-D-aspartate (NMDA) receptors, an analogue derived from the parent drug, phencyclidine (PCP). It is a racemic mixture of its two optical enantiomers, S(+)- and R(–)-ketamine, 28 inducing dissociative and psychotomimetic effects. Alterations in visual, auditory, and proprioceptive stimuli, however, are largely attributed to the actions of S(+)-ketamine,29,30 a more potent antagonist31,32 with stronger analgesic potency 33 than R(–)- ketamine. Once taken, ketamine is initially metabolized to norketamine, undergoing rapid and extensive biotransformation via CYP2B6- and CYP3A4-mediated N-demethylation, and is further metabolized to hydroxynorketamines (HNKs) and dehydronorketamines (DHNKs). 34
Bioavailability (BA) depends on ketamine’s route of administration. 35 The most common route is intravenous (IV) infusion, providing the most predictable dosing with time to peak concentration (Tmax) acutely observed (IV: BA = 100%; Tmax < 1 min). 36 Other routes include intramuscular (IM: BA = 93%; Tmax = 5–30 min), 37 intranasal (IN: BA = 45%; Tmax = 18–21 min),38,39 and oral (PO: BA = 20%; Tmax = 20–120 min) 40 administration. Notably, the esketamine prescription nasal spray, developed by Janssen Pharmaceuticals 41 and FDA-approved for adults with treatment-resistant depression (TRD) in 2019, 42 uses IN administration only.
Since the discovery of ketamine’s fast-acting antidepressant effects,43,44 a growing body of work has supported its role in mood disorders.45–47 This is further evidenced by esketamine’s TRD indication and FDA approval. 42 In addition, ketamine shows antisuicidal properties in adults with psychiatric disorders, 48 with esketamine indicated for acute suicidal ideation and behavior in major depression. The drug also carries prophylactic and transdiagnostic potential. 49 These findings have prompted a paradigm shift in neuropsychiatric research and drug development, 50 underscoring the rationale of targeting the glutamatergic system, over the monoaminergic system, to modulate aberrant neural circuitry.51–55 These discoveries have also stimulated the development of next-generation psychoplastogens, a class of fast-acting compounds like ketamine, to rapidly promote structural and functional neural plasticity.51–55 With respect to PTSD, ketamine is a promising therapeutic given its high comorbidity with major depression and suicidality;56,57 the link between NMDA receptor activity and increased formation of spontaneous, intrusive memories; 58 and the probable role of synaptic dysconnectivity underlying its clinical presentation, disease course, and response to treatment.54,55,59 Here, we synthesize clinical evidence on ketamine in PTSD, with the aim of characterizing emerging trends and informing future research.
Case studies
Donoghue et al. 60 were the first to report ketamine in a 7-year-old boy with PTSD, accompanied by severe, refractory behavioral dysregulation. On two separate occasions, the patient received procedural ketamine (10 mg), once for a tonsillectomy and again for a magnetic resonance imaging (MRI) scan, returning to a residential care facility thereafter. Post-operatively, his clinicians noted markedly improved aggression and emotion control, his therapist reported a newfound ability to discuss past trauma and abuse, and his adoptive parents described increased affection. This enabled the patient to make significant therapeutic gains, with a mean time-to-relapse of 10.5 days.
In adults, Womble 61 first introduced ketamine for PTSD, targeting concomitant TRD among a 26-year-old male combat veteran. Through IV administration, the patient received propofol (anesthetic drug; 30 mg) and ketamine (0.5 mg/kg), both infused over 20 min, pre-treated with midazolam (benzodiazepine sedative; 0.04 mg/kg). No adverse events or side effects were observed. He reported complete remission in depressive symptomatology, as well as in debilitating PTSD-related nightmares, along with uncharacteristic affability and increased life satisfaction. Yet, the effects were transitory, lasting 14 days post-infusion, prior to him returning to a dysphoric state. The use of propofol in this study should be noted, as it may impair emotional episodic memory reconsolidation in humans, and may trigger rapid antidepressant effects. 62
Another case 63 described transient symptom resolution. A 23-year-old male presented to a European Army Medical Center with survivor’s guilt and extreme night terrors, following a 15-month deployment. During this time, he was subject to more than 300 firefights and multiple confirmed kills. The patient was diagnosed with severe, chronic PTSD; however, he remained unresponsive to first- and second-line therapies, including military-specific trauma recovery programs. This led to an elevated risk for suicide. As such, he was given a single dose of ketamine (35 mg) infused over 20 min. His initial response was rapid and robust, taking effect within 2 h, resulting in sizable reductions in PTSD (Mpre = 66.0 vs Mpost = 29.0) as well as in sleep disturbance, anxiety, and functional impairment. Still, the effects were not durable, as the patient regressed to baseline 15 days later.
Artin et al. 64 examined esketamine in veterans with PTSD and TRD. Treated at the VA San Diego Neuromodulation Clinic, patients (N = 35, Mage = 45.4, female = 29%) received IN esketamine scheduled twice weekly for 4 weeks. The first dose started at 56 mg, with subsequent doses titrated up or down based on tolerance and response. Of these patients, a sub-group (n = 19) continued past the eighth dosing, transitioning to a weekly or bi-weekly maintenance schedule. Repeated-measures analyses of variance (ANOVAs) showed significant improvement in PTSD (F [7, 238] = 15.50, p < 0.001) and TRD (F [7, 238] = 8.30, p < 0.001) overtime, with 46% and 14% of patients classified as responders, respectively. Moreover, individuals in the sub-group who completed ⩾16 doses of esketamine, displayed sustained improvement in PTSD (F [7, 126] = 2.70, p = 0.03); yet, this did not extend to TRD (F [7, 126] = 0.70, p = 0.60).
To augment response, ketamine was paired with psychotherapy (KAP) in a case 65 of treatment-resistant, complex PTSD related to racial discrimination. A Black 58-year-old female, engaged in an intensive outpatient program, received four sessions of sublingual ketamine (150 mg) over 13 days. Each session involved preparation, dosing, and integration. Mindfulness-based cognitive therapy (MBCT) and functional analytic psychotherapy (FAP) were specifically used. These interventions were aimed at negative self-talk, catastrophic thinking, and feelings of helplessness. Treatment led to significant reductions in PTSD cognition as well as in comorbid depression and anxiety, lasting 4 months post-treatment. The patient also reported increased psychosocial functioning.
Keizer et al. 66 likewise described KAP in PTSD, though from both civilian and military trauma, with co-occurring neuropathic pain. As part of standard care, patients (N = 11, Mage = 39.7, female = 27%) received continuous ketamine (11–15 μg/kg/min) infused over 96 h, in addition to daily bedside psychotherapy. A paired sample t-test showed significant improvement in PTSD severity (Mpre = 55.3 vs Mpost = 27.1, p = 0.003), with 64% of patients achieving a clinically meaningful response. However, this significance was not observed in neuropathic pain (Mpre = 5.8 vs Mpost = 4.6, p = 0.087). Only 55% of these patients met response criteria.
Most recently, a cohort-based study 67 investigated KAP in a community of healthcare providers impacted by the coronavirus disease (COVID-19) pandemic, a subset of whom screened positive for PTSD (n = 37). At weeks 4, 5, and 7 of a 12-week program (reviewed in Dames et al. 67 ), patients received IM ketamine (1–1.5 mg/kg) over 90 min, supplemented by preparatory and integrative psychotherapy. Results demonstrated significant reduction in PTSD (Mpre = 46.0 vs Mpost = 20.0) symptoms, with 86% of patients screening negative post-treatment.
See Table 1 for a summary of the case studies presented here, including single case reports and cross-sectional, cohort-based, and longitudinal case series.
Summary of case studies.

BDI-II, Beck depression inventory-II; cPTSD, civilian posttraumatic stress disorder; FAP, functional analytic psychotherapy; IN, intranasal; IV, intravenous; MBCT, mindfulness-based cognitive therapy; mPTSD, military posttraumatic stress disorder; NPRS, numeric pain rating scale; PCL-5, PTSD checklist for DSM-5; PCL-M, PTSD checklist for military; PHQ-9, patient health questionnaire-9; PTCI, posttraumatic cognitions inventory; PTSD, posttraumatic stress disorder; R, route of administration; SL, sublingual; TRD, treatment-resistant depression; xPTSD, mixed civilian and military posttraumatic stress disorder.
Sample size of patients with PTSD receiving ketamine.
Chart reviews
Schönenberg et al. 68 examined peri-traumatic ketamine on PTSD in moderately injured accident victims. During emergency transportation, patients received a single dose of ketamine (n = 17, Mage = 36.7, female = 12%) or esketamine (n = 12, Mage = 37.5, female = 25%) combined with midazolam. One-way ANOVAs identified robust effects of medication on peri-traumatic dissociation (F [2, 53] = 11.26, p < 0.001), with the esketamine group displaying markedly increased levels (p < 0.001). Acute stress was additionally significant across three cardinal features of PTSD: dissociation (F [2, 53] = 6.71, p = 0.003), re-experiencing (F [2, 53] = 3.89, p = 0.027), and avoidance (F [2, 53] = 5.27, p = 0.008); although, this did not extend to hyperarousal (F [2, 53] = 1.64, p = 0.205). Regarding sustained PTSD, esketamine patients showed elevated symptoms, relative to ketamine, in re-experiencing (p = 0.034) and avoidance (p = 0.005).
Another chart review 69 analyzed peri-traumatic ketamine in combat soldiers, spanning 3 years of the French military operation in Afghanistan. From their initial sample (N = 274, female < 1%), 54 patients were given ketamine due to injury related to firearms, explosives, or vehicle accidents, of whom met diagnostic criteria for PTSD 3 months post-trauma. In contrast to Schönenberg et al., 68 a multivariate, logistic regression model revealed that ketamine did not predict the development of PTSD, though acute stress [odds ratio (OR) = 16.50 (95% CI: 6.5–41.8); p < 0.001] and surgery frequency [OR = 1.40 (95% CI: 1.2–1.6); p < 0.001] did.
Highland et al. 70 further investigated the relationship between ketamine exposure and PTSD symptoms. In a matched cohort study, using medical record data from Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF), service members were stratified into ketamine (n = 107, Mdnage = 24.0, female = 0%) and non-ketamine (n = 1051, Mdnage = 25.0, female = 2%) groups. Logistic regressions, comparing the risk of developing PTSD, found no significant differences in those treated with or without ketamine (OR = 1.28 [95% CI: 0.48–3.47]; p = 0.62). Linear regressions also showed PTSD severity to be comparable between the groups (Mdiff = 1.98 [95% CI: −0.99 to −4.96]; p = 0.19). These findings underscore prior literature on burned service members and peri-operative ketamine. One study, 58 additionally using OIF-OEF chart data, reported a lower incidence of PTSD in patients given low-dose ketamine than those who were not (27% vs 46%, p = 0.044), despite larger burn sizes, higher injury severity, more operations, and greater time in intensive care. Likewise, a much larger retrospective analysis 71 – led by the same investigators – found that ketamine did not increase PTSD onset in burned soldiers (27% vs 24%, p = 0.582), regardless of significantly greater injuries (p < 0.01). Propensity matching on burn surface area and injury severity neither found remarkable differences in PTSD prevalence between ketamine and non-ketamine groups (26% vs 28%, p = 0.843).
Along the same accord, Melcer et al. 72 examined correlates of pre-hospital ketamine and PTSD prognosis. They randomly sampled military personnel (N = 398, Mage = 25.1, female = 2%) from the Expeditionary Medical Encounter Database, who sustained serious combat injury in Iraq or Afghanistan. Patients were categorized by administration of ketamine, with or without opioids (n = 56) or opioids alone (n = 146), including morphine, fentanyl, and others. Multivariable logistic regressions showed a significant interaction between ketamine versus opioids and traumatic brain injury (TBI) on first-year PTSD [OR = 14.72 (95% CI: 1.37–158.73); p = 0.027]. For patients who did not sustain TBI, ketamine was associated with significantly lower odds of PTSD during the first year [OR = 0.08 (95% CI: 0.01–0.71); p = 0.023]. However, this was not significant for those who did [OR = 1.20 (95% CI: 0.38–3.78); p = 0.756]. Results were additionally non-significant for 2-year PTSD outcomes, with respect to TBI interaction, TBI non-presence, and TBI presence. Nonetheless, patients treated with ketamine had numerically lower 2-year PTSD incidence compared to those receiving opioids (29% vs 38%, p = 0.23).
Given that ketamine may be advantageous over esketamine, 73 one study 74 evaluated both medications in a retrospective switch-over analysis. Veterans with comorbid PTSD and TRD (N = 15, Mage = 49.1, female = 47%) were given ⩾six doses of IN esketamine (56–84 mg) prior to switching to IV ketamine (0.5–1.0 mg/kg), scheduled twice weekly. All patients demonstrated significant improvement in PTSD (F [13, 39] = 5.90, p = 0.006) and TRD (F [14, 42] = 12.60, p < 0.001) post-treatment, as indicated by repeated-measures ANOVAs. Notably, reduction in PTSD severity after switching to ketamine was considerably greater than esketamine alone (t [13] = 3.20, p = 0.007). Improvements were also observed in three of four PTSD symptom clusters: re-experiencing (t [13] = 2.40, p = 0.03), negative mood and cognition (t [13] = 2.50, p = 0.026), and arousal and reactivity (t [13] = 3.10, p = 0.009). Yet, this was not significant for avoidance (t [13] = 1.50, p = 0.15).
Hartberg et al. 75 were among the few to assess sublingual ketamine in PTSD comorbid to TRD (N = 37, Mdnage = 46.0, female = 76%). Patients received a single dose of ketamine (0.5–7.0 mg/kg), held for 2–3 min under tongue, with subsequent doses titrated up by 20% to 50% twice daily (3 h apart), scheduled twice per week. From baseline to post-treatment, the number of inpatient hospital days (p < 0.001) and number of admissions for psychiatric episodes (p < 0.001) were significantly reduced by 70% and 65%, respectively. No tolerance building, acute adverse events, or long-term negative effects were observed.
Taking a step further, Davis et al. 76 examined KAP in trauma-exposed individuals, leveraging sublingual administration and body-centered techniques. As part of standard care, patients (N = 18, Mage = 45.2, female = 56%) underwent six sessions of ketamine (100–200 mg) combined with somatic-based interactional psychotherapy, each 120 min. This approach targeted autonomic nervous system reactivity, aimed at promoting adaptive regulation of challenging internal experiences, without inducing fear or dissociation. Paired sample t-tests showed clinically meaningful improvement in PTSD (Mdiff = 1.9, t = 2.03, p = 0.058, d = −0.48) and functional disability (Mdiff = 1.8, t = 2.12, p = 0.05, d = −0.52); and a significant reduction in depression (Mdiff = 1.2, t = 2.58, p = 0.019, d = −0.61). However, anxiety symptoms remained unchanged following treatment (Mdiff = 0.6, t = 1.19, p = 0.249, d = −0.28).
See Table 2 for a summary of the chart reviews presented here, including cohort-based, crossover, and longitudinal studies using retrospective data.
Summary of chart reviews.

AIS, associated injury score; ASDS, acute stress disorder scale; cPTSD, civilian posttraumatic stress disorder; FAP, functional analytic psychotherapy; GAD-2, generalized anxiety disorder-2; ICD-9 CM, International Classification of Diseases Clinical Modification, 9th revision for posttraumatic stress disorder; IES-R, impact of event scale-revised; IN, intranasal; ISS, injury severity score; IV, intravenous; LEC-5, life event checklist5; MBCT, mindfulness-based cognitive therapy; mPTSD, military posttraumatic stress disorder; PCL-5, PTSD checklist for DSM-5; PCL-C, PTSD checklist for civilian; PCL-M, PTSD checklist for military; PCL-S, PTSD checklist for specific; PC-PTSD-5, primary-care posttraumatic stress disorder-5; PDEQ, peri-traumatic dissociative experiences scale; PHQ-2, patient health questionnaire-2; PHQ-9, patient health questionnaire-9; PTSD, posttraumatic stress disorder; R, route of administration; SDS, Sheehan disability scale; SL, sublingual; TBSA, total body surface area; TLEQ, traumatic life events questionnaire.
Sample size of patients with PTSD receiving ketamine.
Sample size of patients with PTSD, during the first-year post-injury, receiving ketamine.
Open-label studies
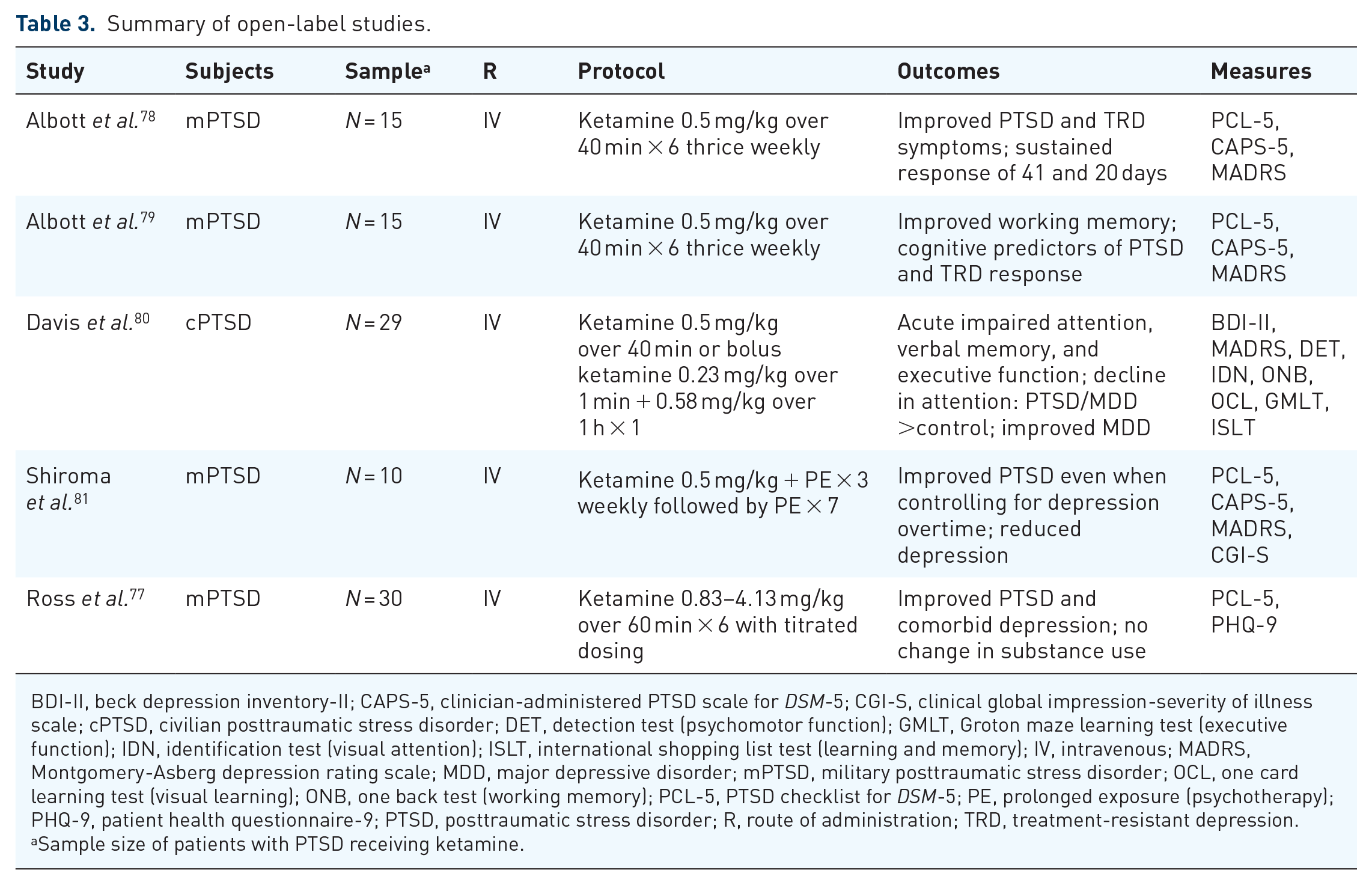
To characterize transpersonal dissociative experiences, Ross et al. 77 explored the use of ketamine in veterans with PTSD, stemming from combat trauma (N = 30, Mage = 46.5). Patients were also screened for TRD and alcohol and substance abuse. Treatment involved six, 1-h ketamine infusions over 2–3 weeks, starting at 1.0 mg/kg that increased according to response thereafter. Settings were additionally tailored at the individual level, with a subset of patients watching nature videos and/or listening to ambient music. From baseline to post-treatment, PTSD (F = 55.60, p < 0.001, d = 1.42) and TRD (F = 90.00, p < 0.001, d = 1.38) significantly improved by 44% (Mpre = 56.2 vs Mpost = 31.3) and 50% (Mpre = 18.9 vs Mpost = 9.5), respectively. Alcohol and substance abuse, however, remained unaffected despite positive anecdotal reports.
Albott et al. 78 further examined the safety, efficacy, and durability of repeat ketamine in veterans with PTSD and concomitant TRD (N = 15, Mage = 52.1, female = 33%). Patients received six doses of ketamine (0.5 mg/kg) infused over 40 min, scheduled thrice weekly, with data collected 24 h post-infusion as well as 8 weeks following treatment. Results showed continuous reductions in PTSD [Mdiff = 33.3 (95% CI: 23.0–43.5); p < 0.001] and TRD [Mdiff = 26.6 (95% CI: 23.0–30.2); p < 0.001] symptoms, both associated with large effect sizes (d‘² = 2.17 and d‘² = 4.64, respectively). Transient increases in dissociation were also noted. In regard to durability, 80% of patients achieved PTSD remission, carrying a median time-to-relapse of 41 days; whereas 93% of patients responded to TRD, with a median time-to-relapse of 20 days.
A secondary analysis 79 of the Abbott et al. 78 study investigated changes in neurocognitive performance and its role in predicting ketamine response. Patients completed a battery of cognitive tests at baseline and following all six ketamine infusions. Tasks were administered online and in a fixed sequence, measuring attention, working memory, visual and verbal learning, processing speed, and set shifting. Paired sample t-tests revealed significant improvements in working memory (Mdiff = 14.4, t [14] = 2.56, p = 0.023) post-treatment, with a medium effect size (d = 0.72); yet, this was not identified in other domains. In addition, large reductions in PTSD and TRD were associated with lower working memory (rPTSD = −0.55, p = 0.036; rTRD = −0.56, p = 0.029), slower processing speed (rPTSD = 0.59, p = 0.028; rTRD = −0.59, p = 0.02), and faster set shifting (rPTSD = −0.55, p = 0.036; rTRD = −0.57, p = 0.028) at baseline. Lower verbal learning (rTRD = −0.528, p = 0.043) also predicted improved TRD.
Likewise, Davis et al. 80 examined the effect of ketamine on cognitive function, specifically among patients with PTSD and/or MDD (n = 29, Mage = 36.1, female = 62%) relative to healthy controls (n = 29, Mage = 33.3, female = 55%). In each group, approximately half received 0.5 mg/kg of ketamine infused over 40 min, while the remaining received 0.58 mg/kg infused over 1 h, pre-treated with a bolus of 0.23 mg/kg over 1 min. Across study groups, ketamine impaired attention, verbal memory, and executive function 2 h post-administration, resolving completely within 1 day. No change was observed in working memory. Notably, the magnitude was greater in patients with PTSD and/or MMD in attention only (F = 6.99, p = 0.012, d = 0.56). Repeated measures ANOVAs further showed a significant interaction of psychiatric status and depression across timepoints (F = 11.39, p < 0.001, d = 0.86), with symptom severity decreasing from moderate to mild. Change in baseline cognitive function, however, was not associated with ketamine’s antidepressant response.
Another study 81 investigated the feasibility of repeat ketamine adjunct to PE in trauma-exposed veterans. In a 10-week pilot, patients (N = 10, Mage = 45.1, female = 30%) received IV ketamine (0.5 mg/kg) 24 h prior to weekly PE over 3 weeks, followed by ⩽seven PE sessions. Linear mixed models, with intent-to-treat analysis, demonstrated markedly improved clinician-reported (t [11] = 4.21, p = 0.001, d = 1.21) and self-reported (t [11] = 6.35, p < 0.001, d = 1.83) PTSD, as well as improved depression (t [11] = 4.68, p = 0.001, d = 1.35). In addition, change in global PTSD (F [1, 10] = 5.69, p = 0.038, h2 = 0.36) and avoidance (F [1, 10] = 6.31, p = 0.031, h2 = 0.36) remained significant when controlling for depression over time; although, intrusion (F [1, 10] = 4.48, p = 0.06, h2 = 0.31), negative mood and cognition (F[1, 10] = 3.83, p = 0.079, 0 2 = 0.28), and hyperarousal (F[1, 10] = 1.25, p = 0.29, h2 = 0.11) did not.
See Table 3 for a summary of the open-label studies presented here, including cross-sectional, cohort-based, and comparative studies.
Summary of open-label studies.
BDI-II, beck depression inventory-II; CAPS-5, clinician-administered PTSD scale for DSM-5; CGI-S, clinical global impression-severity of illness scale; cPTSD, civilian posttraumatic stress disorder; DET, detection test (psychomotor function); GMLT, Groton maze learning test (executive function); IDN, identification test (visual attention); ISLT, international shopping list test (learning and memory); IV, intravenous; MADRS, Montgomery-Asberg depression rating scale; MDD, major depressive disorder; mPTSD, military posttraumatic stress disorder; OCL, one card learning test (visual learning); ONB, one back test (working memory); PCL-5, PTSD checklist for DSM-5; PE, prolonged exposure (psychotherapy); PHQ-9, patient health questionnaire-9; PTSD, posttraumatic stress disorder; R, route of administration; TRD, treatment-resistant depression.
Sample size of patients with PTSD receiving ketamine.
Randomized trials
Feder et al. 82 were the first to compare the efficacy of ketamine (n = 22, Mage = 36.4, female = 59%) to midazolam (n = 19, Mage = 35.7, female = 32%), as a treatment for chronic PTSD, in a proof-of-concept, double-blind, active placebo-controlled, crossover randomized controlled trial (RCT). Following psychiatric medication washout, patients received a single dose of ketamine (0.5 mg/kg) or midazolam (0.045 mg/kg) infused over 40 min, to which the order was randomly assigned and scheduled 2 weeks apart. A mixed-model crossover analysis revealed significant reduction in PTSD severity, 24 h post-infusion, between ketamine and midazolam [Mdiff = 12.7 (95% CI: 2.5–22.8); p = 0.02]. Ketamine was additionally well-tolerated with transient dissociation that resolved completely. No serious psychotic or manic symptoms were observed.
These findings informed a double-blind, active placebo-controlled, parallel-arm RCT, 83 evaluating the safety, efficacy, and durability of repeat ketamine infusions. Their sample similarly comprised individuals with chronic PTSD, though from both civilian and military trauma. Employing randomly permuted blocks, patients underwent six ketamine (n = 15, Mage = 39.3, female = 87%) or midazolam (n = 15, Mage = 38.5, female = 67%) infusions, following the previously described dosing regimen, scheduled thrice weekly over 2 weeks. Improvement in PTSD over the course of study visits differed significantly between the two medications (F [2, 55] = 5.97, p = 0.005), with lower severity reported in the ketamine versus midazolam group (Mdiff = 11.88, SE = 3.96, p = 0.004) at the 2-week primary endpoint. Mixed modeling also showed significant group-by-time interactions for three of four PTSD symptom clusters: intrusion (F [2, 55] = 3.77, p = 0.03), avoidance (F [2, 55] = 12.29, p < 0.001), and negative mood and cognition (F [2, 55] = 4.42, p = 0.02). This did not extend to arousal and reactivity (F [2, 55] = 2.47, p = 0.09). Regarding duration of effect, there was a median time-to-relapse of 27.5 days among ketamine responders (67%) post-treatment.
An ad hoc, observational analysis 84 of this trial further explored neuroimaging correlates and predictors of ketamine response. Using elastic-net regression, Norbury et al. 84 analyzed functional imaging data collected from a subset of patients undergoing repeat ketamine (n = 11, Mage = 42.5, female = 91%) or midazolam (n = 10, Mage = 42.3, female = 80%) infusions. This comprised data from two emotion-processing tasks and one task-free scan. Across all patients, the most reliable predictor of PTSD improvement was increased functional connectivity between the ventromedial prefrontal cortex (vmPFC) and amygdala (βs = 2.90), specifically when viewing emotional face stimuli. This effect was notably stronger in the ketamine group (β = 0.86), targeting cardinal PTSD symptoms over and beyond concomitant reductions in depression. Moreover, findings from an effective connectivity analysis, via dynamic causal modeling, showed that lower baseline vmPFC inhibition of the amygdala, during emotional face viewing, was associated with greater overall ketamine response.
The promise of low-dose ketamine for chronic pain (CP) and PTSD, as separate diagnoses, motivated Dadabayev1 et al. 85 to examine its effect on their comorbidity. In a double-blind, active placebo-controlled, four-arm RCT, veterans were randomized to one of the following groups: CP + PTSD with ketamine (n = 11, Mage = 45.3, female = 36%), CP + PTSD with ketorolac (nonsteroidal anti-inflammatory drug; n = 10, Mage = 40.1, female = 40%), CP with ketamine (n = 10, Mage = 43.5, female = 10%), or CP with ketorolac (n = 10, Mage = 52.9, female = 10%). A single dose of ketamine (0.5 mg/kg) or ketorolac (15 mg reconstituted in 500 cc of saline) was infused over 40 min, pre-treated with 4 mg of ondansetron (anti-nausea medication). Two-way repeated measures ANOVAs showed a main effect of time on PTSD in the CP + PTSD groups (F [1, 52] = 9.35, p < 0.01), with symptoms markedly decreasing from baseline to 7 days post-infusion. However, there was no significant effect of medication (ketamine vs ketorolac) on PTSD (p > 0.05) nor group-by-time interactions (p > 0.05), suggesting comparable improvement in symptomatology.
Given that benzodiazepines have potential to worsen PTSD outcomes, 86 Abdallah et al. 87 compared an inactive placebo to active comparators in a double-blind, three-arm RCT. Here, investigators tested the efficacy of repeat ketamine in veterans and active-duty military with refractory PTSD. Patients were randomized to three parallel arms, receiving low-dose ketamine (0.2 mg/kg; n = 53, Mage = 45.2, female = 19%), standard ketamine (0.5 mg/kg; n = 51, Mage = 43.2, female = 26%), or saline placebo (n = 54, Mage = 42.0, female = 26%). Study drugs were administered intravenously over 40 min and scheduled twice weekly for 4 weeks. Mixed-model analyses failed to identify dose-related effects of ketamine on PTSD symptoms (F [2, 148] = 1.80, p = 0.17), with no significant group-by-time interactions (F [18, 137] = 1.10, p = 0.38). Nonetheless, standard ketamine was advantageous over placebo in reducing comorbid depression 24 h post-first infusion (Mdiff = 4.6, p = 0.02, adj. p = 0.05) and at the end of treatment (Mdiff = 6.4, p = 0.004, adj. p = 0.01). Notably, this improvement was not sustained during the 4-week follow-up period.
In an effort to prolong its therapeutic effect, Pradhan et al. 88 evaluated ketamine with Trauma Interventions using Mindfulness Based Extinction and Reconsolidation (TIMBER) psychotherapy. In a double-blind, placebo-controlled, crossover RCT, patients with chronic refractory PTSD received a single dose of ketamine (n = 5, Mage = 37.2, female = 100%) or placebo (n = 5, Mage = 48.8, female = 40%) infused over 40 min combined with 12 sessions of TIMBER, 45 min each. These groups were referred to as TIMBER-K and TIMBER-P, respectively. Of the TIMBER sessions, three occurred during the first week of infusion, including 10 min before and after dosing, followed by nine sessions weekly. From baseline to 24 h post-infusion, 90% of patients displayed improvement in clinician reported (Mpre = 87.6 vs Mpost = 20.0, p < 0.001) and self-reported (Mpre = 75.1 vs Mpost = 25.9, p < 0.001) PTSD, as well as in concomitant depression (Mpre = 26.1 vs Mpost = 4.3, p < 0.001) and anxiety (Mpre = 48.9 vs Mpost = 8.6, p < 0.001). The TIMBER-K group also showed increased durability (Mdays = 33.0 vs 25.0, p = 0.545); however, this difference was only marginally significant.
To further examine clinical response, as well as correlates of d-serine (DSR; a potent co-agonist at the NMDA glutamate receptor), Pradhan et al. 89 conducted a follow-up, double-blind, placebo-controlled, parallel-arm RCT. Here, patients were randomized to either TIMBER-K (n = 10) or TIMBER-P (n = 10), undergoing the same intervention protocols as previously described. Plasma samples were additionally collected pre- and post-infusion. Akin to the former trial, results indicated greater sustained response with TIMBER-K compared to TIMBER-P (Mdays = 34.4 vs 16.5, p = 0.022). DSR plasma levels were also positively correlated with baseline PTSD severity (r = 0.42, p = 0.07) and negatively correlated with treatment durability (r = −0.02, p = 0.93). Yet, neither effect was significant.
See Table 4 for a summary of the randomized trials presented here, including placebo- or active placebo-controlled trials. Table 5 provides an additional summary of outcome measures and therapeutic responses in open-label and randomized studies.
Summary of randomized trials.

CP, chronic pain; cPTSD, civilian posttraumatic stress disorder; DSR, d-serine; IV, intravenous; mPTSD, military posttraumatic stress disorder; PTSD, posttraumatic stress disorder; R, route of administration; RCT, randomized controlled trial; TIMBER, trauma interventions using mindfulness based extinction and reconsolidation (psychotherapy); vmPFC, ventromedial prefrontal cortex; xPTSD, mixed civilian and military posttraumatic stress disorder.
Summary of outcome measures and therapeutic responses.

AUDIT, alcohol use disorders identification test; BAI, Beck anxiety inventory; BDI-II, Beck depression inventory, 2nd edition; BFI-I, brief pain inventory-interference; BFI-P, brief pain inventory-pain; CADSS, clinician-administered dissociative states scale; CAPS-5, clinician-administered PTSD scale for DSM-5; CAPS-4, clinician-administered PTSD scale for DSM-IV; DAST-10, drug abuse screen test; DSR, d-serine; GCI-I, clinical global impression-improvement; CGI-S, clinical global impression-severity; HAM-D-17, 17-item Hamilton rating scale for depression; IES-R, impact of event scale-revised; MADRS, Montgomery-Asberg depression rating scale; OLS, open-label study; PCL, PTSD checklist; PCL-5, PTSD checklist for DSM-5; PHQ-9, patient health questionnaire-9; QIDS-SR, quick inventory of depressive symptomatology, self-report; RCT, randomized controlled trial; VAS, visual analogue scale.
Discussion
Herein, utilizing a narrative review approach, we identified 26 studies that retrospectively or prospectively examined ketamine in PTSD, excluding two ad hoc analyses. A systematic review, risk of bias assessment, and pooled statistics – such as meta-regressions – were not performed due to high variance in study design, methods, and measured outcomes. Overall, ketamine does not appear to increase the risk of developing PTSD, addressing early concerns over its psychosomatic effects; and provides encouraging signals of therapeutic safety, efficacy, and durability. This is supported by a rapidly growing evidence base (see Figure 1). Importantly, treatment regimens were highly tolerated, with no serious adverse events reported. Ketamine-induced dissociative and psychotomimetic symptoms were transient, resolving completely within 1–2 h on average. However, findings regarding efficacy are still mixed, with the largest RCT 87 failing to identify significant dose-related effects of ketamine on PTSD. While this was specific to veterans and military personnel, more robust data are patently needed.
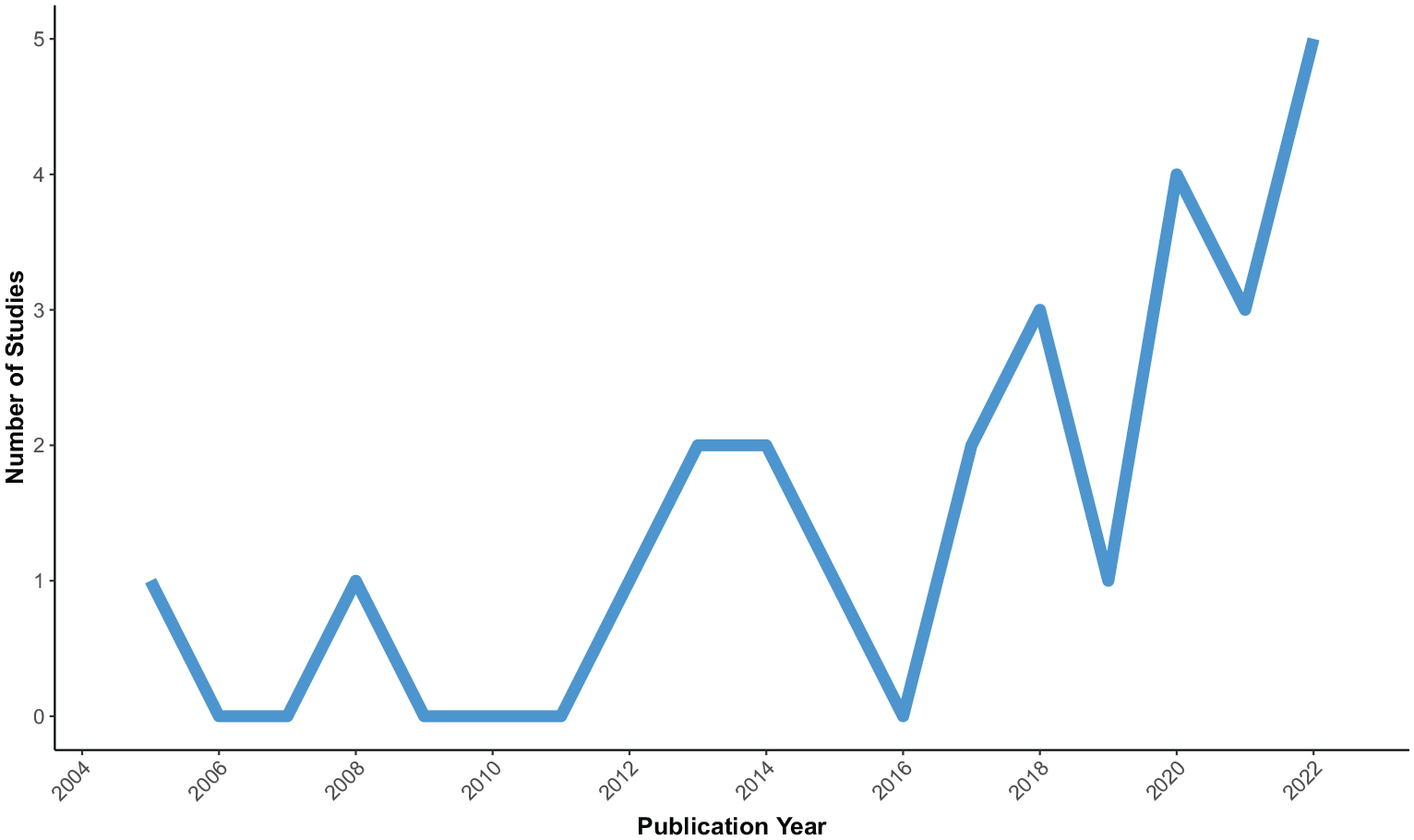
Distribution of studies investigating ketamine in posttraumatic stress disorder (PTSD) over time by publication year.
Two factors largely attributing to study heterogeneity were clinical presentation and pharmacological approach. The majority of studies involved veterans and active-duty military with combat-related trauma (mPTSD, 54%), followed by civilian trauma (cPTSD, 31%), or a combination of both (xPTSD, 15%). See Figure 2 for a breakdown of studies investigating ketamine for PTSD by trauma type. Akin to recent events, one case series explored ketamine in a community of healthcare providers with lived experience of PTSD and treatment failure, who were further impacted by COVID-19. 67 Yet, no studies included first responders 4 nor Indigenous People, 5 both of whom have significantly elevated rates of PTSD alongside service members. 3 If these groups were included, they were not identified as such. Looking ahead to the research pipeline, an observational study recently investigated ketamine as a treatment for PTSD among paramedics working in emergency medical services for at least 5 years (NCT03947099). Their sample comprised seven patients, each undergoing six 1-h infusions of ketamine scheduled over 3 weeks. The results are forthcoming.

Number of studies investigating ketamine in posttraumatic stress disorder (PTSD) by study design and trauma type.
Moreover, psychiatric and medical comorbidities of PTSD were frequently described, with concomitant TRD reported most often. This is unsurprising given ketamine’s antidepressant activity and indication for mood disorders,45–47 namely TRD and MDD. Two studies focused on concurrent chronic pain 85 and neuropathic pain, 66 both highly comorbid with PTSD, especially among veterans. However, neither study demonstrated significant improvement in pain following ketamine treatment. These findings are noteworthy, given that ketamine is a well-established analgesic used for procedural sedation in addition to acute and chronic pain management. 90 Its poor efficacy may have resulted from its dose threshold, which is much lower in psychiatric and behavioral medicine. Future research stands to benefit from judiciously investigating ketamine in co-occurring PTSD and pain, particularly when pain develops post-trauma.
Pharmacological approach also varied widely. Most studies used IV infusion (69%), while a subset leveraged sublingual (12%), IM (8%), and IN (4%) methods. See Figure 3 for routes of administration. Two chart reviews72,74 combined approaches (IM-IV, 4%; IN-IV, 4%). Of import, all open-label and randomized trials employed ketamine infusions, delivered at 0.5 mg/kg over 40 min, apart from one study 77 administering high-dose ketamine (0.83–4.13 mg/kg) infused over 1 h. With IV administration used most consistently, there is great prospect for replicability in future work to identify standard approaches that maximize patient benefit. This contrasts to the use of IN esketamine, which few studies investigated despite its FDA-approval for TRD. While esketamine is not currently indicated for PTSD, studies employing IN administration will be critical in characterizing the full potential of ketamine and esketamine for this population. Exploring, understanding, and optimizing ketamine regimens will be equally important in determining efficacy and real-world effectiveness. At present, there is a distinct trend towards repeat dosing over single dosing, as shown in Figure 4. This reflects pipeline trends in the field, with all five trials – actively recruiting or recently completed – testing three-to-six serial treatments of ketamine for PTSD. See Table 6 for a summary of ongoing trials registered with ClinicalTrials.gov. However, the rationale and protocol for these dosing schedules, and how alterations may influence efficacy and durability of effect, warrants further investigation.
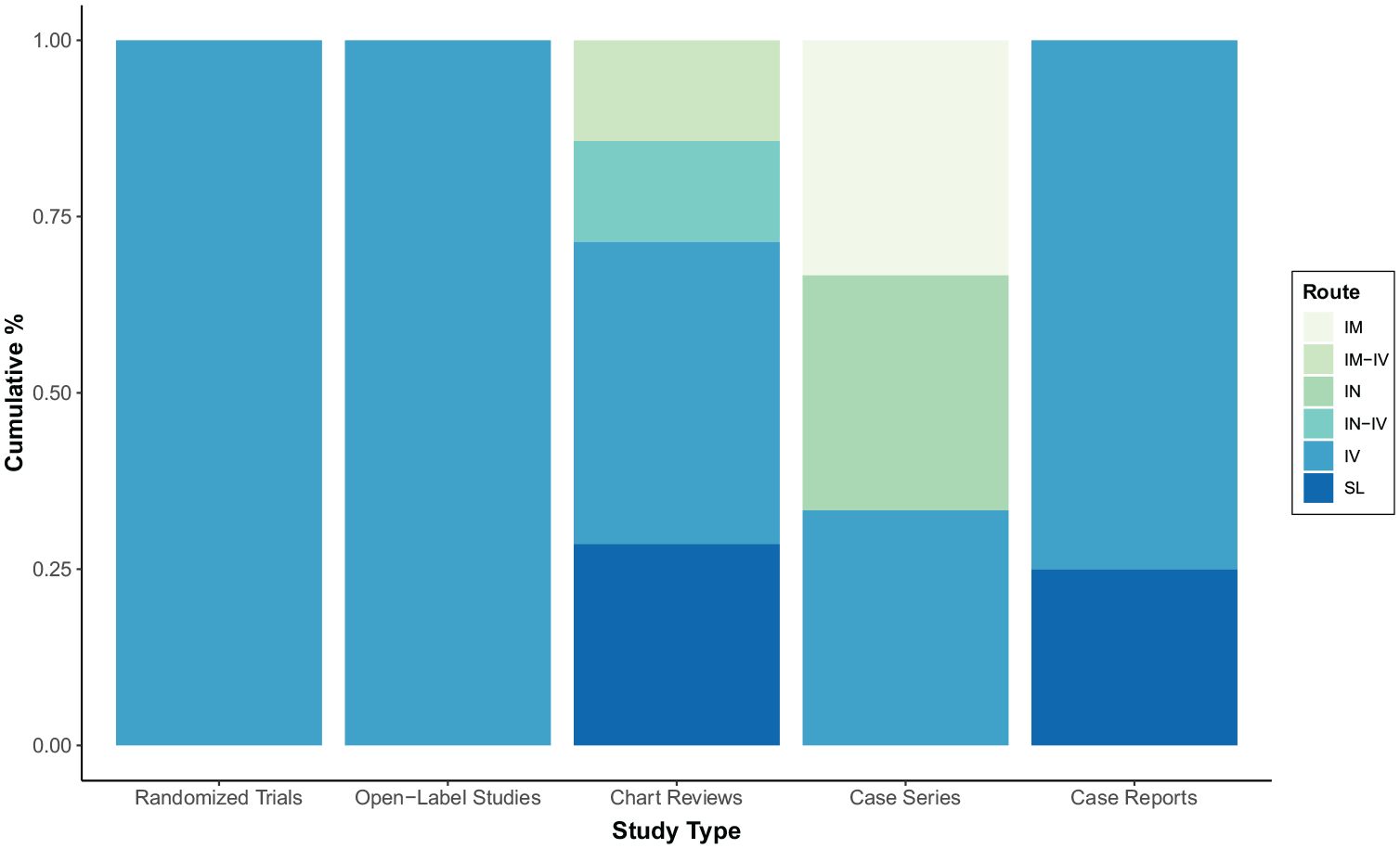
Percentage of studies investigating ketamine in posttraumatic stress disorder (PTSD) by study design and route of administration.
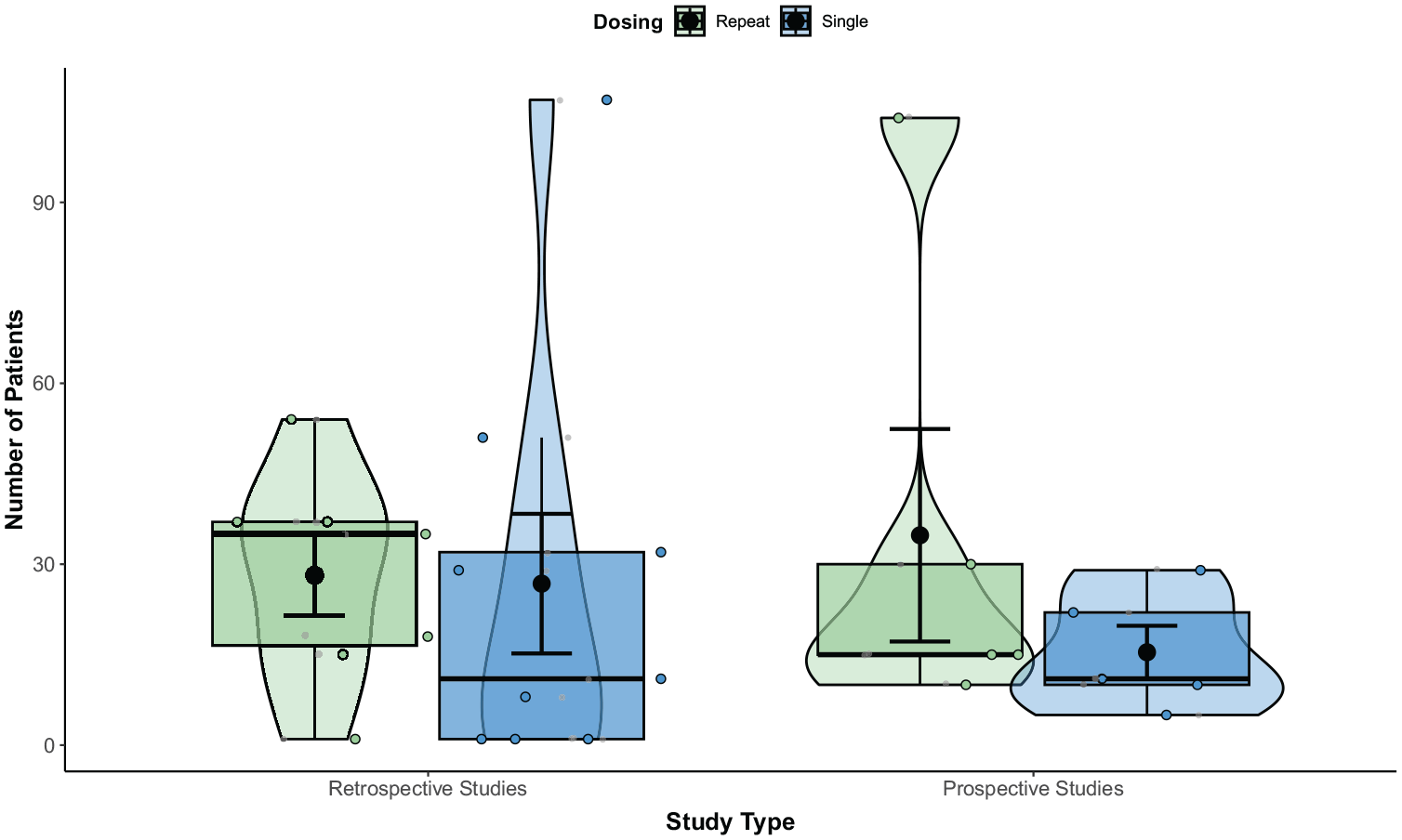
Number of patients with posttraumatic stress disorder (PTSD) treated with ketamine in retrospective versus prospective studies by dosing, using single or repeated schedules.
Summary of registered clinical trials.

cPTSD, civilian posttraumatic stress disorder; co-MDD, comorbid major depressive disorder; IV, intravenous; mPTSD, military posttraumatic stress disorder; NCT, national clinical trial number (identifier); Obs, observational study; PE, prolonged exposure (psychotherapy); R, route of administration; RCT, randomized clinical trial; eTF-CBT, online trauma-focused cognitive behavioral therapy (psychotherapy); xPTSD, mixed civilian and military posttraumatic stress disorder; WET, written exposure therapy (psychotherapy).
Given the time-limited effects of ketamine, a portion of studies investigated adjunctive or combination psychotherapy for PTSD (Figure 5). This generally involved three steps: preparatory psychotherapy, supervised ketamine dosing, and integrative psychotherapy designed to prime, socially support, and process treatment experiences, respectively. Yet, psychotherapeutic approaches were highly variable or unspecified, with some trauma- and/or cognitive behavioral-focused, some lacking preparation and/or integration, and some delivered in clinical versus real-world settings. Pradhan et al. 88 specifically used TIMBER psychotherapy, a type of mindfulness-based graded exposure to target traumatic memories, aimed at prolonging the effects of ketamine for refractory PTSD. Nine of 10 patients demonstrated robust improvement in primary and secondary outcome measures, with a sustained response of approximately 30 days. The authors postulated that ketamine and TIMBER psychotherapy produce a positive synergistic response, potentiating each other, that utilizes a reconsolidation window 6 h posttraumatic memory reactivation.91,92

Cumulative percentage of studies investigating ketamine in posttraumatic stress disorder (PTSD) by study design and pharmacological approach, administering ketamine with or without psychotherapy.
Overall, few studies delivered psychotherapy with ketamine; however, nearly half of trials in the research pipeline do, including prolonged exposure (NCT04560660), written exposure therapy (NCT04889664), and trauma-focused cognitive behavioral therapy (NCT04771767). While ketamine may be an effective stand-alone intervention for PTSD, therapeutic support may foster a sense of safety and security, lower resistance to dissociative and transpersonal experiences, and facilitate engagement in treatment. At a neural level, ketamine in psychotherapy is theorized to increase access to traumatic memory via enhanced synaptic connectivity, decrease central sensitization through transient downregulation of the prefrontal cortex, and augment extinction of previously paired pain-related memories. 66 Serial treatments, as previously mentioned, might also help sustain ketamine’s duration of effect. This was recently observed in a case 93 of extreme and enduring bulimia nervosa, complicated by lifespan polytrauma. The patient underwent 18 sessions of repeated KAP, involving person-centered, humanistic psychotherapy, resulting in complete and sustained remission.
Finally, discussing patients’ goals and expectations for treatment, assessing their current psychological state, and providing an appropriate context for the ketamine experience are key factors to consider in future work. This is particularly central, as ‘set and setting’ has been shown to impact subjective, behavioral, and therapeutic effects of psychedelics, including ketamine.94,95 Examining different psychotherapeutic techniques and styles, such as free-form and manualized therapy, is further recommended.
Regarding trials, one long-standing challenge is the ability to double-blind patients and investigators to treatment allocation.96–98 This plays an important role in reducing detection bias and maintaining intrinsic validity. However, ketamine and other psychoactive drugs are prone to ‘functional unblinding’, otherwise known as code-breaking, due to treatment-emergent adverse events. In the case of ketamine, patients may recognize its acute dissociative effects, enhancing expectations of therapeutic benefit and response. The use of active placebos over saline is commonly employed to address this concern, yet carries limitations. A systematic review and meta-analysis, for instance, showed that midazolam, a putative active comparator in ketamine studies, 99 worsened drug versus control differences in PTSD treatment. 100 In their RCT, Feder et al. 82 also noted that ketamine was associated with higher rates of transient dissociation than midazolam, likely affecting their blind. Moreover, trial personnel who trust in the efficacy of ketamine for PTSD might – knowingly or unknowingly – influence patients’ statuses. This, too, may lead to an overestimation of treatment effects, and subsequently more significant outcomes. Blinding of outcome assessors was additionally absent and/or unreported in trials, which plays a fundamental role in soft endpoints, such as psychosocial functioning and quality of life. To minimize the risk of functional unblinding, investigators may consider remote, telephone-based raters, like those used in esketamine trials for major depression. 101
Conclusion
Ketamine has increasing potential for PTSD, with a rapidly growing evidence base. Psychotherapy holds further merit in prolonging treatment effects, when combined with ketamine, pointing to real, discernable patient benefit. This is evermore salient, given the poor prognosis of PTSD, especially in chronic refractory cases, and the limit in efficacious interventions. Notwithstanding, there is high heterogeneity in clinical presentation and pharmacological strategy. A standard protocol for delivering ketamine based on trauma type, severity, and duration is critically absent. More generally, there is dissensus on the ideal administration route and dosing regimen for this population; and whether to inlcude psychotherapy or supportive care. Finally, increasing diversity in samples will be important for characterizing the potential benefits of ketamine for PTSD, broadly. This can be achieved through diverse study personnel, inclusive recruitment strategies, and equtiable treatment protocols. Data collection in real-world settings is also encouraged. At present, more robust and longitudinal data are needed to explore, establish, and optimize ketamine in PTSD; and to determine the contexts and interventional frameworks it is best suited for.