
Abstract
We report on the case of a 46-year-old woman with generalized anxiety disorder, paranoid personality disorder, and mild reduction in glomerular filtration rate (GFR). She was treated with pregabalin, trazodone, hydroxyzine, and clonazepam before hospital admission. Pharmacotherapy for the patient was changed during her first week in the hospital. Dosing of hydroxyzine and clonazepam was gradually decreased, and then these two drugs were withdrawn. Treatment with amisulpride was started on the fourth day after admission, and amisulpride serum levels were then measured three times as a part of therapeutic drug monitoring (TDM). The serum concentration of amisulpride detected during concurrent use of trazodone and pregabalin was approximately twice the therapeutic range for amisulpride. When the dose of pregabalin was reduced by half, the serum concentration of amisulpride decreased to therapeutic serum levels. We hypothesize that an interaction between amisulpride and pregabalin was responsible for the increased amisulpride concentration since both drugs are almost exclusively excreted from the body by the renal route. Pregabalin–amisulpride interaction might also be influenced by concomitant therapy with trazodone or a mild reduction in GFR. However, we only have clinical evidence for an interaction between amisulpride and pregabalin because after we halved the dose of pregabalin, the amisulpride concentration decreased, and the C/D ratio normalized. This could be helpful information for psychiatrists in order to avoid drug–drug interactions between amisulpride and pregabalin. We recommend TDM of amisulpride in patients treated concomitantly with other drugs eliminated mainly by the kidneys.
Introduction
Patients with generalized anxiety disorder are often treated for extended periods, that is, months or years. Medication is generally not used to treat patients with paranoid personality disorder (PPD); however, if there are psychotic symptoms, treatment with antipsychotics can be considered. Even though there are many second-generation antipsychotic agents to choose from, it can be challenging to find the right one for patients who have psychosis. Amisulpride is an antipsychotic agent used at high doses 400–800 mg to treat schizophrenia and at low doses 50–200 mg to treat minor depression/dysthymia and primary negative syndrome in schizophrenia. Amisulpride may be preferred in some patients because it has a low risk of metabolic side effects and does not lead to increased body weight. With respect to drug–drug interactions, amisulpride has the advantage of not being metabolized by cytochrome P450 enzymes in the liver and has a low potential for pharmacokinetic interactions. Nevertheless, it does not mean that there is no potential for pharmacokinetic interactions in the kidneys. The interaction between lithium and amisulpride, which are both eliminated from the body by the kidneys, has been described. 1 We did not find any other examples of drug–amisulpride interactions in the kidneys; however, in our clinical practice, we recently found one that may be of interest to clinicians. The therapeutic range of serum levels for amisulpride is 100–320 ng/ml, and the alert level is 640 ng/ml. 2 Pregabalin is an antiepileptic drug with anxiolytic properties that is approved for long-term pharmacotherapy of generalized anxiety disorder (GAD). Trazodone is an established antidepressant suitable for treating unipolar depression associated with anxiety and insomnia.
Case description
A 46-year-old female patient was admitted to the hospital with GAD and PPD. She presented fluctuating anxiety and paranoid thinking, and at its most intense verging on delusional. She mainly complained about several injustices that had occurred in the past. She also had vegetative symptoms of anxiety, such as chest tightness, shortness of breath, and tingling in the limbs. At admission, she was being treated with daily doses of trazodone 150 mg, pregabalin 300 mg, hydroxyzine 100 mg, and clonazepam 4 mg; she had been taking this combination of medicines for several months before admission. The patient had individual consultations with a clinical psychologist and a social worker as adjuncts to her pharmacotherapy during hospitalization. Complete blood biochemistry was done at the beginning and the end of the patient’s stay in the hospital.
Laboratory findings during admission found normal liver function, creatinine (80 μmol/l), urea (4.3 mmol/l), and uric acid (245 μmol/l). Thyroid gland function as well as body mass index (BMI = 24.57) were also normal. The CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) Creatinine Equation showed a mild reduction in glomerular filtration rate (eGFR) 76.8 ml/min at the beginning of hospitalization; eGFR was also mildly reduced in the fourth week and sixth week, see Table 1. This finding was confirmed with a 24-h urine collection and measurement of Creatinine Clearance (GFR = 86 ml/min) at the end of hospitalization.3,4
Summary of pharmacotherapy during hospitalization in 2018 (January 15–February 20).

The therapeutic range of amisulpride plasma levels: 100–320 ng/ml. Amisulpride serum levels decreased after dose reduction from 400 to 300 mg, and after pregabalin was reduced by one-half. CKD-EPI, estimation of creatinine clearance; ClCr, clearance of creatinine; NA, not applicable.
The clinical suspicion of a PPD was confirmed by psychological examination. Regarding pharmacotherapy, the case psychiatrist decided to gradually decrease the dose of hydroxyzine and clonazepam and then withdraw these two drugs. On the fourth day of hospitalization, the patient was started on amisulpride due to paranoid delusion. The amisulpride was titrated up to 400 mg daily. The serum concentration of amisulpride was measured three times during the in-hospital pharmacotherapy. Liquid chromatography-tandem mass spectrometry was used and validated according to international standards for the determination of amisulpride levels in the blood. The first measurement detected an increased amisulpride serum concentration of 756 ng/ml. This concentration was well over the laboratory alert level, which is 640 ng/ml. The attending psychiatrist was surprised by such a high serum concentration of amisulpride, considering that the dose given was in the middle of the dosage range, that is, 400 mg; range 100–800 mg. During treatment, the patient did not experience side effects such as akathisia, muscle rigidity, or tremor, nor did the attending psychiatrist observe extrapyramidal symptoms that might be acute consequences of a high amisulpride serum concentration. The psychiatrist decreased the amisulpride dose to 300 mg q.d. in response. A second measurement was conducted after a week of amisulpride 300 mg q.d.; the serum concentration of amisulpride was 544 ng/ml. When the dose of pregabalin was reduced from 300 mg to 150 mg q.d., the concentration of amisulpride declined to 254 ng/ml with the patient taking amisulpride 300 mg q.d. During hospitalization, the patient’s antipsychotic medication mitigated the urgency and influence of the past alleged injustices on her behavior. In accordance with the main diagnosis, the primary paranoid processing of external events failed to be affected by medication. Her anxiety decreased to the point that she did not feel any vegetative symptoms, but the anxiety did not disappear completely. After 37 days of hospitalization, the patient was released to outpatient care, and she was recommended to find a psychologist skilled in systematic psychotherapy. The course of pharmacotherapy, amisulpride serum concentrations, and measurement of renal functions during hospitalization are set out in Table 1 and Figure 1.

TDM of amisulpride (AMI) during hospitalization.
Discussion
Factors influencing the concentration of amisulpride in the blood
Gender and age aspects
The therapeutic serum levels of amisulpride are 100–320 ng/ml. 2 A recent combined meta-analysis of the concentration of oral amisulpride in patients showed that there is significant inter-individual variability in plasma levels of amisulpride and suggested that being female contributes to higher amisulpride concentrations. 1 Analysis of therapeutic drug monitoring (TDM) data found sex differences in amisulpride serum concentrations, but the differences did not reach statistical significance. 5 In previously published clinical studies, dose-corrected amisulpride concentrations in the blood were also higher in women than in men. However, the authors concluded that gender-specific aspects were not relevant for clinical practice except at higher doses.6,7 A review of studies conducted on healthy volunteers revealed that the Cmax was the parameter with the greatest variability. 8 A small study on older people showed that physicians should consider adjusting amisulpride dosing in older patients, especially in those over 85 years. 9 Age-related changes in the pharmacokinetics of amisulpride should also be considered in patients older than 65 years because of normal declines in renal function. 1 The patient in our case report was 46 years old; therefore, the age of the patient did not impact her amisulpride serum concentrations.
Amisulpride renal excretion
Amisulpride is eliminated from the systemic circulation primarily (74%) by renal excretion as an unchanged drug. 10 Czech marketing authorization holder of Solian (Sanofi-Aventis) recommends a reduction of amisulpride dosing by 50% for GFRs in the range of 30–60 ml/min. The Maudsley Prescribing Guidelines in Psychiatry also recommend dose reduction of amisulpride by half in the case of a decline in renal function. 11 In contrast, the Food and Drug Administration (FDA)-approved summary of product characteristics for Barhemsys® states that no dosage adjustment of amisulpride is necessary for patients with mild-to-moderate renal impairment, that is, an eGFR of 30 ml/min/1.73m2 and above. We assessed eGFR three times during hospitalization, and in none of the measurements was the GFR less than 60 ml/min (Table 1).
Co-prescription of other drugs together with amisulpride
In a study conducted in 2007, increases in amisulpride concentrations were described after the addition of lithium. 12 A recent meta-analysis of female patients on a combination of lithium and amisulpride showed that they had higher amisulpride concentrations and C/D ratios. 1 Lithium and amisulpride are both eliminated from the body by the kidneys; therefore, lithium and amisulpride may interact through competition for renal drug excretion. On the other hand, clozapine coadministration did not affect plasma amisulpride concentrations. 5 Amisulpride is a substrate for the P-glycoprotein efflux pump and for several organic cation transporters OCT1, OCT2, OCT3, OCTN1, and OCTN2.13–16
Pregabalin does not inhibit cytochrome P450 biotransformation enzymes, its renal elimination kinetics is linear, and pregabalin is not a substrate for human P-glycoprotein.17,18 Pregabalin is eliminated from the systemic circulation primarily by renal excretion as an unchanged drug. As pregabalin clearance is directly proportional to creatinine clearance, dose reduction in patients with compromised renal function must be individualized according to creatinine clearance below 60 ml/min. 19
Pregabalin, therefore, has little or no drug–drug interactions. 18 For example, pregabalin drug interaction studies have confirmed that there are no effects on the pharmacokinetics of carbamazepine, lamotrigine, valproate, or tramadol.20,21 However, pregabalin was shown to increase clozapine serum levels in several case reports and the proposed mechanism of interaction was competitive inhibition during renal drug excretion.22–24 In our patient, the dose of pregabalin was titrated slowly because pregabalin concentrations are subject to high inter-subject variability. 25 When we consider that both pregabalin and amisulpride are eliminated almost exclusively by the kidneys, it is possible that the addition of amisulpride to pregabalin resulted in an elevation of amisulpride serum levels. We hypothesize that pregabalin and amisulpride may compete at three levels: (1) influx drug transporters [organic cation transporters 2 (OCT2)], (2) efflux drug transporters [novel organic cation transporters 1 (OCTN1)], and (3) multidrug and toxin extrusion transporters (MATE1). The competion occurs because amisulpride and pregabalin are both substrates of OCT2 and OCTN1.26–28 Moreover, amisulpride is a substrate and inhibitor of MATE1,16,26 and pregabalin inhibits MATE1; 27 this might be the probable underlying mechanism for the pharmacokinetic interaction (see Table 2 and Figure 2). The other possible factor that could have influenced the final amisulpride blood concentrations was concomitant therapy with trazodone. Trazodone can increase the plasma concentrations of digoxin and carbamazepine, and product information recommends monitoring digoxin concentrations if used with trazodone. 29 Trazodone is metabolized by the cytochrome P450 3A4 enzyme. Trazodone is a P-glycoprotein substrate, and trazodone is also a substrate and inhibitor of renal organic cation transporters.30–32 When we consider that amisulpride is a substrate of P-glycoprotein and organic cation transporters, it suggests that therapy with trazodone contributed to the elevation of amisulpride plasma concentrations. Less than 5% of trazodone is excreted unchanged in the urine; approximately 70% of the active metabolites are also excreted by the kidneys. The manufacturer states that adjustment of trazodone dosing is usually not necessary. Nevertheless, trazodone should be prescribed with caution to patients with severe renal impairment. 11 The use of hydroxyzine should not have had a significant effect on the plasma levels of amisulpride since hydroxyzine was withdrawn on day 10 of hospitalization, and the first TDM of amisulpride was conducted 5 days later on day 15; therefore, hydroxyzine had been mostly eliminated from the body before the concentration of amisulpride was analyzed. A major metabolite of hydroxyzine is cetirizine with a half-life of approximately 10 h; as such, cetirizine also could not impact amisulpride concentrations. Interestingly cetirizine is a substrate and an inhibitor of P-glycoprotein, an inhibitor of organic cation transporters OCT2, and cetirizine also inhibits renal MATE1 and MATE2 transporters. 27 Selected pharmacokinetic data that are relevant to the biotransformation and elimination of amisulpride, pregabalin, trazodone, and hydroxyzine are shown in Table 2.
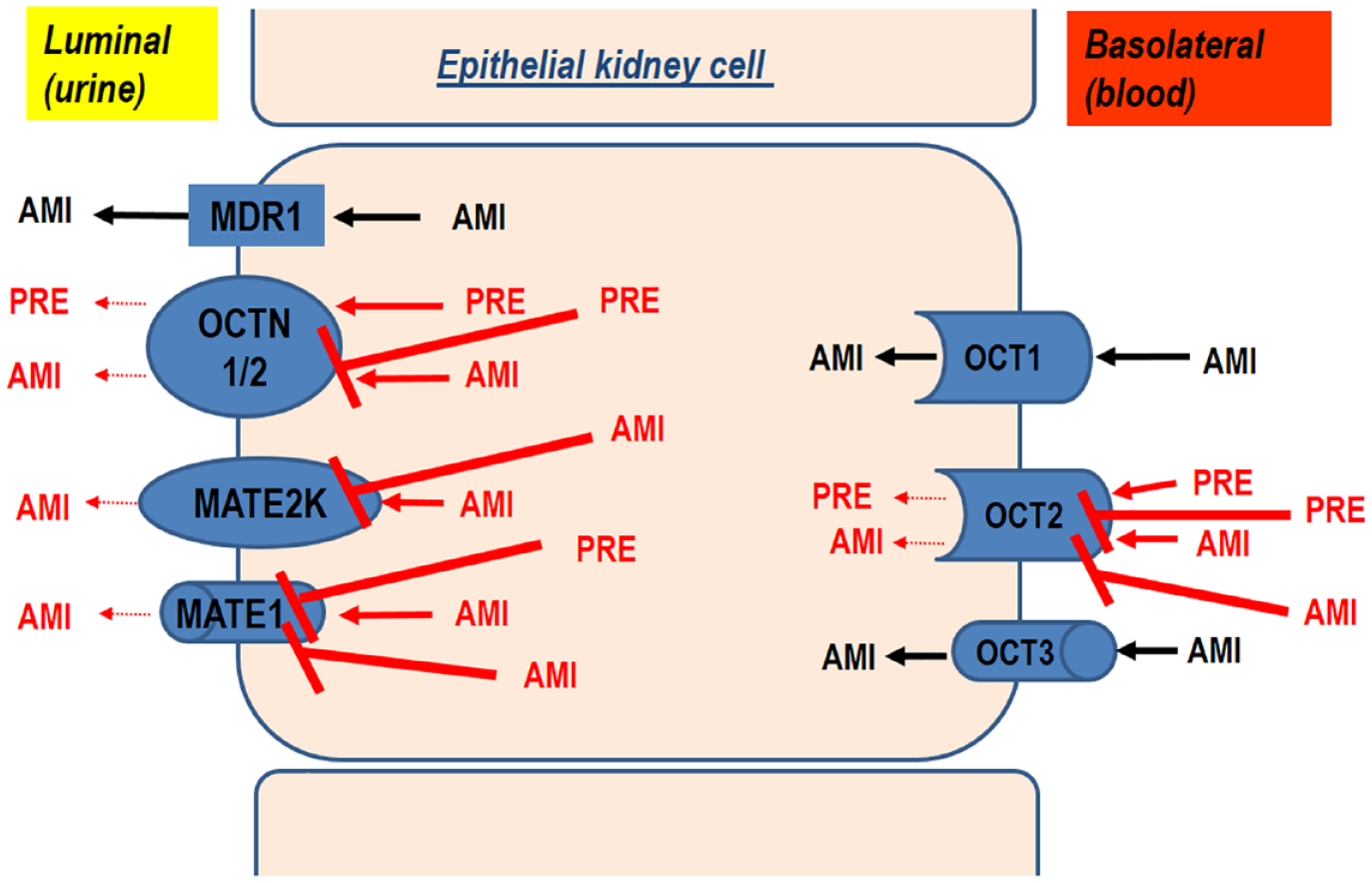
Hypothetical underlying mechanism for the pharmacokinetic interaction between amisulpride and pregabalin in epithelial kidney cells.
Biotransformation and elimination of amisulpride, pregabalin, trazodone and hydroxyzine.

AUC, area under the curve; CYP enzymes, biotransformation enzymes belonging to the cytochrome P450 family; MATE1, multidrug and toxin extrusion protein 1; MATE2 K, multidrug and toxin extrusion protein 2 K; OCT1, organic cation transporter 1; OCT2, organic cation transporter 2; OCT3, organic cation transporter 3; OCTN1, novel organic cation transporter 1; OCTN2, novel organic cation transporter 2; P-gp, P-glycoprotein; SPC, a summary of product characteristics.
The concentration of amisulpride in relation to the prescribed dose
In our patient, amisulpride serum levels were = 756 ng/ml after the first, 544 ng/ml after the second, and 254 ng/ml after the third measurement, with the first and second measurements being much higher than the currently recommended concentrations of 100–320 ng/ml. Some authors previously suggested that the optimal range of concentrations for amisulpride should be 200–500 ng/ml. 33 The first and second measurements of amisulpride levels in serum found the concentrations greater than 500 ng/ml. Concentration-to-dose (C/D) ratios were calculated in our patient; the first ratio was 1.89, followed by 1.81, and finally, 0.85 (see Figure 1). C/D ratios are inversely related to total clearance. A high C/D ratio indicates slow and a low C/D ratio rapid drug clearance. According to consensus guidelines for TDM in neuropsychopharmacology, the range of C/D ratios for amisulpride should be 0.47–0.87 ng/ml/mg. 2 In our patient, only the last C/D ratio of 0.85 was within the recommended range of dose-corrected concentrations of amisulpride.
Strengths and limitations of the case report
Our case report has strengths and limitations. The first strength is repeated measurement of the serum amisulpride concentration. Second, between each measurement, there was only one change in drug dosing, and we waited with other measurements for the new steady-state drug concentration. We decreased amisulpride daily doses by 100 mg (1/4 of former doses), and the serum level decreased by 212 ng/ml (approximately by 1/3); however, only a minimal change in the amisulpride C/D ratio was observed. A decrease in the dose of pregabalin by one-half led to a decrease of the amisulpride serum level by more than 50% (from 544 to 254 ng/ml), and the amisulpride C/D ratio changed. The third strength is repeated measurements of renal functions that were above the cut-off (60 ml/min) for moderate renal function reduction. The use of the CKD-EPI creatinine equation was only an estimation of true glomerular filtration; we also used 24-h urine sampling to measure GF more accurately. That measurement confirmed that the GFR was only mildly reduced and that observed amisulpride C/D ratio changes were probably due to a drug–drug interaction than unrecognized kidney disease. The first limitation is that we use only one measurement per new treatment situation. The use of more measurements might have helped estimate the role of amisulpride serum fluctuations. 1 Second, we did not measure pregabalin and trazodone serum concentrations. Third, the pregabalin–amisulpride interaction may have also been influenced by concomitant use of trazodone or by a mild reduction in GFR. We did not change trazodone doses, and therefore we were not able to exclude the influence of trazodone. Fourth, the evidence of the interactions between amisulpride and renal transporters is difficult to assess due to partially conflicting literature,13,16,26 depending on the type of experiment conducted and concentration of substance (therapeutic or supratherapeutic) used.
Conclusion
The probable reason for the drug–drug pharmacokinetic interactions in this case report was a competition between amisulpride and pregabalin during renal elimination or the influence of concomitant therapy with trazodone and a mild reduction in GFR. Both drugs (pregabalin and trazodone) or a mild reduction of glomerular filtration rate could play a theoretical role in the observed interaction with amisulpride. However, we only have clinical proof for pregabalin because after decreasing the dose of pregabalin by one-half, we observed a decrease in the amisulpride concentration and normalization of amisulpride C/D ratio. This could be new information for psychiatrists regarding the addition of amisulpride to a patient taking pregabalin; the addition can result in an increase in serum amisulpride concentrations. TDM can help prevent overdoses in patients taking amisulpride and the development of serious adverse drug reactions.