
Abstract

Dear Editor,
Milnacipran is a serotonin–noradrenaline reuptake inhibitor (SNRI) that is effective in treating patients with major depression (MD). 1 Antidepressant treatment in MD has been associated with alterations in peripheral cytokine levels. 2 Monoamine levels in the cerebrospinal fluid are also altered after treatment with antidepressants in MD. 3 Thus, we investigated the plasma levels of 3-methoxy-4-hydroxyphenylglycol (MHPG), a metabolite of noradrenaline or interleukin-6 (IL-6), and the clinical response to milnacipran in MD. We also examined the correlation between plasma MHPG and IL-6 levels before and after milnacipran treatment.
Twenty-four patients who met MD criteria per the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) were enrolled in this study (ages 48.7 ± 13.9 years; male/female 12/12; single/repeated episode 6/18). Improvement in depressive symptoms was evaluated using the 17-item Hamilton Rating Scale for Depression (HAMD). The detection of plasma IL-6 and plasma MHPG was done by sandwich enzyme-linked immunosorbent assay (ELISA) and high-performance liquid chromatography, respectively. The maximum dose of milnacipran at week 4 was 77.0 ± 19.3 mg/day. Changes in plasma MHPG or IL-6, and HAMD scores are shown in Table 1.
Parameter changes.
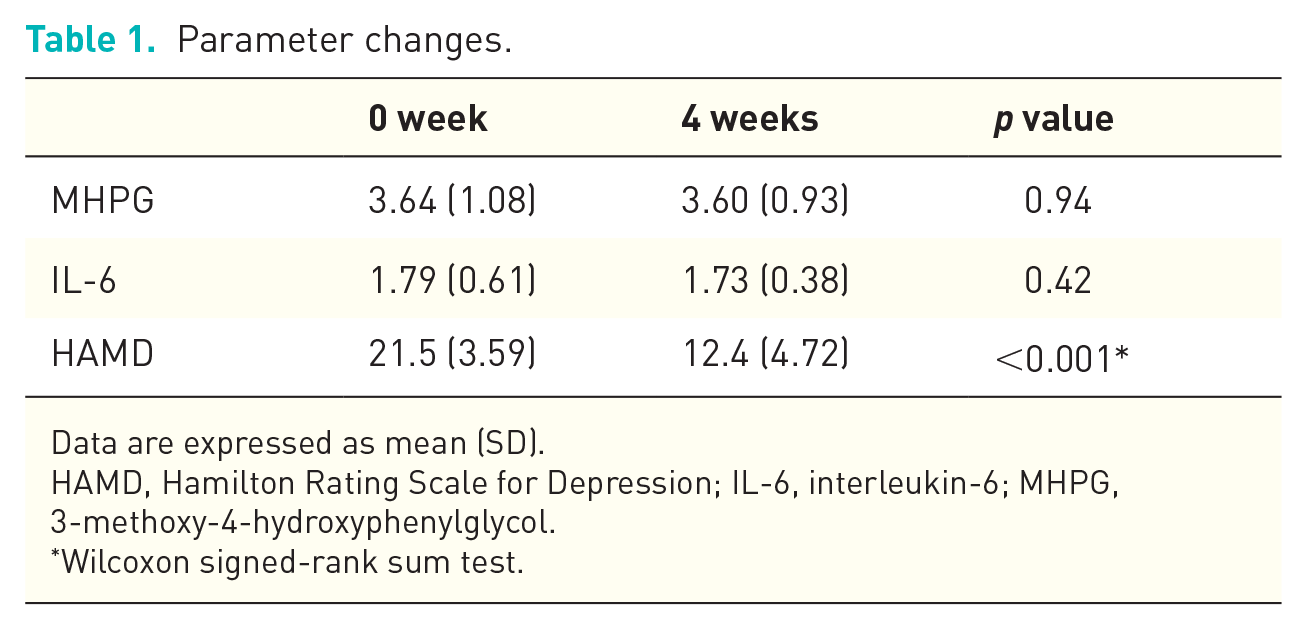
Data are expressed as mean (SD).
HAMD, Hamilton Rating Scale for Depression; IL-6, interleukin-6; MHPG, 3-methoxy-4-hydroxyphenylglycol.
Wilcoxon signed-rank sum test.
The plasma levels of MHPG and IL-6 were not altered before or 4 weeks after milnacipran treatment. HAMD scores significantly decreased after milnacipran treatment. No correlation was found between the changes in plasma MHPG and the changes in HAMD scores before and 4 weeks after milnacipran treatment (r = -0.0030, p = 0.98, Pearson correlation coefficient). No correlation was found between the changes in plasma levels of IL-6 and changes in the HAMD scores (r = 0.00030, p = 0.99, Pearson correlation coefficient). Moreover, there was no correlation between changes in plasma MHPG levels and changes in plasma IL-6 levels (r = 0.021, p = 0.92, Pearson correlation coefficient).
We previously reported a positive correlation between changes in plasma MHPG levels and changes in HAMD scores in first-episode MD patients, 4 which was not confirmed in this study. The discrepancy between our former study and this study may be due to 18 patients of 24 had a history of recurrent, multiple episodes of MD and their average depressive episode was 3.1 in this study. Another report determined that serum levels of IL-6, IL-8, and macrophage inflammatory protein-1β could be used as biomarkers to predict response to milnacipran. 5 In short, the authors suggested that serum levels of IL-6 and IL-8 might be potential blood biomarkers for response to milnacipran in MD patients. Our results show no association between changes in plasma IL-6 levels and response to milnacipran treatment, which was not in accordance with other reports. 5 Our present study only focused on the relationship between plasma levels of IL-6 and response to milnacipran, but not adverse effects. The effect of noradrenaline on induced IL-6 release is primarily mediated by β2-adrenergic receptors, suggesting interaction between noradrenaline and IL-6. 6 Our present study showed no correlation between levels of plasma MHPG and plasma IL-6. 6 Milnacipran improved depressive symptoms at least until week 4. Since we could not detect successfully other cytokines, including IL-1β, IL-8, and tumor necrosis factor (TNF)-α, in this study, we are now undergoing the study measuring these cytokines and response to several antidepressants.
All descriptive statistics and statistical analyses were performed using Python ver. 3.0.