
Abstract
Post-traumatic stress disorder (PTSD) is a debilitating psychiatric disorder. While current treatment options are effective for some, many individuals fail to respond to first-line psychotherapies and pharmacotherapy. Transcranial magnetic stimulation (TMS) has emerged over the past several decades as a noninvasive neuromodulatory intervention for psychiatric disorders including depression, with mounting evidence for its safety, tolerability, and efficacy in treating PTSD. While several meta-analyses of TMS for PTSD have been published to date showing large effect sizes on PTSD overall, there is marked variability between studies, making it difficult to draw simple conclusions about how best to treat patients. The following review summarizes over 20 years of the existing literature on TMS as a PTSD treatment, and includes nine randomized controlled trials and many other prospective studies of TMS monotherapy, as well as five randomized controlled trials investigating TMS combined with psychotherapy. While the majority of studies utilize repetitive TMS targeted to the right dorsolateral prefrontal cortex (DLPFC) at low frequency (1 Hz) or high frequency (10 or 20 Hz), others have used alternative frequencies, targeted other regions (most commonly the left DLPFC), or trialed different stimulation protocols utilizing newer TMS modalities such as synchronized TMS and theta-burst TMS (TBS). Although it is encouraging that positive outcomes have been shown, there is a paucity of studies directly comparing available approaches. Biomarkers, such as functional imaging and electroencephalography, were seldomly incorporated yet remain crucial for advancing our knowledge of how to predict and monitor treatment response and for understanding mechanism of action of TMS in this population. Effects on PTSD are often sustained for up to 2–3 months, but more long-term studies are needed in order to understand and predict duration of response. In short, while TMS appears safe and effective for PTSD, important steps are needed to operationalize optimal approaches for patients suffering from this disorder.
Introduction
Post-traumatic stress disorder (PTSD) is a debilitating psychiatric disorder characterized by symptoms from four core clusters after exposure to a traumatic event: re-experiencing symptoms which include flashbacks and nightmares, hyperarousal, avoidance of internal and external stimuli related to trauma, and negative alterations in mood and cognition.1,2 While lifetime prevalence in the United States is estimated around 6% in the general population, 3 the prevalence of PTSD in certain subpopulations including military veterans is significantly higher (e.g. point prevalence was found to be around 12–13% in military personnel soon after their return from combat duty in Iraq). 4 The impact of negative health sequelae on the lives of those with PTSD is hard to overstate. Patients have increased rates of social and occupational dysfunction, comorbid psychiatric illness [over half also meet criteria for major depressive disorder (MDD)], substance use, and suicide.5–7 Equally hard to overstate is the need for new treatment options, with important limitations of both first-line psychotherapeutic and pharmacologic interventions.8–11 For example, while recent meta-analysis data 9 show large effect sizes for both cognitive processing therapy (CPT) and prolonged exposure (d = 0.78–1.10), only 49–70% of patients have a clinically meaningful response and 60–72% do not achieve remission. Well-known to trauma therapists, drop-out rates are very high with trauma-focused therapies, averaging 36% according to another meta-analysis. 10 Compared with the effect sizes of the above psychotherapies, those of first-line medications have been shown to be lower (g = 0.41–0.74), again with many individuals not responding meaningfully. 11
With the emergence over the past several decades of neurostimulation for the treatment of psychiatric disorders, there has been a growing body of literature on the application of these modalities in PTSD. While many of these neurostimulation treatments, including transcranial direct current stimulation (tDCS), vagus nerve stimulation (VNS), and deep brain stimulation (DBS), show promise, the studies remain limited and the evidence for efficacy is preliminary (for a comprehensive review of the neuromodulatory techniques studied for PTSD, see Koek et al. 12 ). The major exception to this is therapeutic transcranial magnetic stimulation (TMS, which is different from single pulse and other forms of related stimulation used for neurophysiological research). As a noninvasive intervention that uses induction of electromagnetic fields to modulate cortical circuitry, TMS has a substantial body of literature demonstrating safety, tolerability, and efficacy in the treatment of pharmacoresistant depression (e.g, George et al. 13 and O’Reardon et al. 14 ; reviewed in Cosmo et al. 15 ), and was cleared by the US Food and Drug Administration for this indication in 2008. 1 While its use in PTSD is less well established, the evidence for its efficacy is accumulating. For example, one of the most recent meta-analyses of TMS for PTSD included 11 randomized controlled trials (RCTs) and demonstrated a significant reduction in core PTSD symptoms with a large and medium effect size (Hedges’s g = –0.975 and –0.680) for high- and low-frequency TMS, respectively, applied to the right dorsolateral prefrontal cortex (DLPFC). 16
In the present article, we review and summarize the existing literature on TMS for PTSD and highlight a number of important issues, including optimal parameters of stimulation, laterality and targets of stimulation, newer TMS protocols such as theta-burst TMS (TBS), and TMS as monotherapy versus combination with psychotherapies.
Principles and practice of TMS
TMS is a noninvasive neuromodulatory intervention that makes use of Faraday’s law of electromagnetism by running an alternating current through a conductive coil that is placed on a patient’s scalp. This generates a focal and fluctuating magnetic field, which induces an electrical field and depolarizes neurons in a targeted brain region. Some of the earliest studies in the development of TMS targeted the primary motor cortex in order to evoke reliable muscle activity, for example, stimulation of the hand knob of M1 with corresponding contraction of the contralateral hand. 17 This basic application to the motor system is, in fact, still utilized clinically in the determination of a ‘motor threshold’ (MT), that is, the least amount of energy required to elicit a motor response, upon which stimulation intensity is based (e.g. stimulating at 120% of the patient’s MT). Each magnetic ‘pulse’ reaches a peak magnetic field strength of around 1.5 Tesla and stimulates predominantly cortical gray matter of the target region, most commonly the DLPFC in its clinical application to psychiatric disorders. 18
When these magnetic pulses are run in quick succession to form ‘trains’, the technique is referred to as repetitive TMS. Depending on the frequency of the pulses, cortical excitability can be effectively increased, as with high-frequency protocols (typically 10–20 Hz), or decreased, as with low-frequency protocols at 1 Hz or less.19,20 Each TMS session is thus comprised of several trains with protocol pulse frequency, train duration, intertrain intervals, and session total of pulses. For example, in the original FDA-cleared use of TMS for pharmacoresistant MDD, patients receive high-frequency (10 Hz) stimulation at 120% of their MT targeting the left DLPFC with a train duration of 4 s and intertrain interval of 26 s for a session total of 3000 pulses. Each session lasts 37.5 min and patients have five sessions per week for 4–6 weeks, making the total dose of 60,000–90,000 pulses.
More recently, TMS protocols such as TBS have been gaining traction. Mimicking endogenous theta rhythms of hippocampal pyramidal neurons, TBS delivers triplet bursts (i.e. three 50 Hz pulses) at 5 Hz which similarly increase or decrease cortical excitability but do so in far less time, with sessions lasting 10 min or less.21,22 Given the significant improvements in patient burden and cost-effectiveness, with compelling evidence for noninferiority in MDD, 23 TBS marks an important advancement and may have used in the treatment of other psychiatric disorders, including PTSD. As described below, the protocols used in the literature thus far for PTSD, which have included both 10 Hz TMS as well as TBS, have varied significantly, and determining the importance of TMS parameters remains critical.
Early formative studies
With the rapid advancement of functional imaging in the 1990s came the conceptualization of PTSD as a disease of aberrant neural circuitry involving trauma-recall associated hypermetabolism of right-sided limbic, para-limbic, and frontal cortical regions. 24 Around this time, TMS had not only been shown to be capable of altering cerebral metabolism but had also been successfully applied to treatment-resistant depression. 25 Recognizing the potential of TMS to alleviate PTSD symptoms based on this novel type of neurobiological targeting, two formative studies were published in 1998 examining its safety, tolerability, and clinical effects. McCann et al. 26 reported two cases treated with multiple 20-min sessions of 1 Hz TMS to the right DLPFC that showed reductions in PTSD symptom scores at variable time points with return to baseline by 1-month follow-up. Positron emission tomography scans revealed decreases in cerebral metabolism more prominently in the right hemisphere posttreatment. In an unblinded prospective study of 0.3 Hz TMS to the left and right motor cortices applied successively in one session, Grisaru et al. 27 demonstrated improvement in several core PTSD symptom domains that was transient and suggested repeating stimulation sessions. This approach was taken in the next prospective study published 4 years later in which 12 comorbid PTSD/MDD patients received 10 sessions of either 1 or 5 Hz TMS to the left DLPFC. 28 While the primary outcome was depressive symptoms, for which participants showed a 75% response rate post-TMS, core combat-related PTSD symptoms, anxiety, and anger also showed statistically significant decreases, though these were notably smaller effects (e.g. 6% decrease in core PTSD measures). Although the study was limited by a small sample size and unblinded design, the authors highlighted the greater effect of left-sided stimulation on mood symptoms over PTSD symptoms, as well as the lack of difference between the 1 and 5 Hz groups on all measures.
The first RCT of TMS for PTSD was conducted by Cohen et al. 29 in 2004 and included 29 participants receiving 10 sessions of 10 Hz, 1 Hz, or sham TMS to the right DLPFC. Compared with both sham and low-frequency TMS, 10 Hz TMS was superior in improving core PTSD as well as anxiety symptoms. At 2-week follow-up, both re-experiencing and avoidance symptoms as measured by the Clinician Administered PTSD Scale (CAPS) 30 remained significantly reduced compared with baseline (approximately 32%). Depressive symptoms were not impacted in any group. Of note, total doses differed between active groups with 1000 pulses administered in the 1 Hz group versus 4000 in the 10 Hz, meaning higher total dose rather than frequency may have explained the superior outcomes in the 10 Hz group.
These foundational studies demonstrated safety and tolerability of TMS in the PTSD population and provided crucial preliminary evidence for efficacy in reducing core PTSD and anxiety symptoms, with some indication toward favoring right-sided stimulation. Notably, stimulation parameters varied significantly and the total doses administered were relatively low (e.g. 1000–4000 total pulses in Cohen et al. 29 and 6000 total pulses in Rosenberg et al. 28 ) compared with the > 90,000 pulses in a treatment course using currently cleared protocols.
TMS monotherapy
To date there have been nine RCTs investigating the efficacy of TMS monotherapy for PTSD (Table 1), five of which were published between 2018 and 2020. Two of these investigated newer TMS modalities, namely synchronized TMS (sTMS, described below) and TBS. A number of open-label prospective studies and case series have also been published (Tables 2 and 3) and are also highlighted.
RCTs of TMS monotherapy for PTSD..

BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BNCE, Brief Neurobehavioral Cognitive Examination; CAPS, Clinician Administered PTSD Scale; DLPFC, dorsolateral prefrontal cortex; DMN, default-mode network; GAD-7, Generalized Anxiety Disorder Assessment; HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale; IAF, individualized alpha frequency; IPF, Inventory of Psychosocial Functioning; MADRS, Montgomery–Asberg Depression Rating Scale; MDD, major depressive disorder; MT, motor threshold; NA, not available; NSI, Neurobehavioral Symptom Inventory; PCL, PTSD Checklist; PCL-M, PTSD Checklist Military; PTSD, post-traumatic stress disorder; QIDS-SR, Quick Inventory of Depressive Symptomatology–Self Report; QLESQ, Quality of Life Enjoyment and Satisfaction Questionnaire; RCTs, randomized controlled trials; rTMS, repetitive transcranial magnetic stimulation; SOFAS, Social and Occupational Functioning Assessment Scale; STAI, State Trait Anxiety Inventory; sTMS, synchronized transcranial magnetic stimulation; TBS, Theta-burst transcranial magnetic stimulation.
Unblinded prospective studies of TMS monotherapy for PTSD..

CGI, Clinical Global Impression; HAM-D, Hamilton Depression Rating Scale; IES, Impact of Event Scale; MDD, major depressive disorder; MISS, Mississippi Scale of Combat Severity; MT, motor threshold; PTSD, post-traumatic stress disorder; rTMS, repetitive transcranial magnetic stimulation; SCL-90, The Symptom Checklist–90.
Case reports and case series of TMS monotherapy for PTSD..
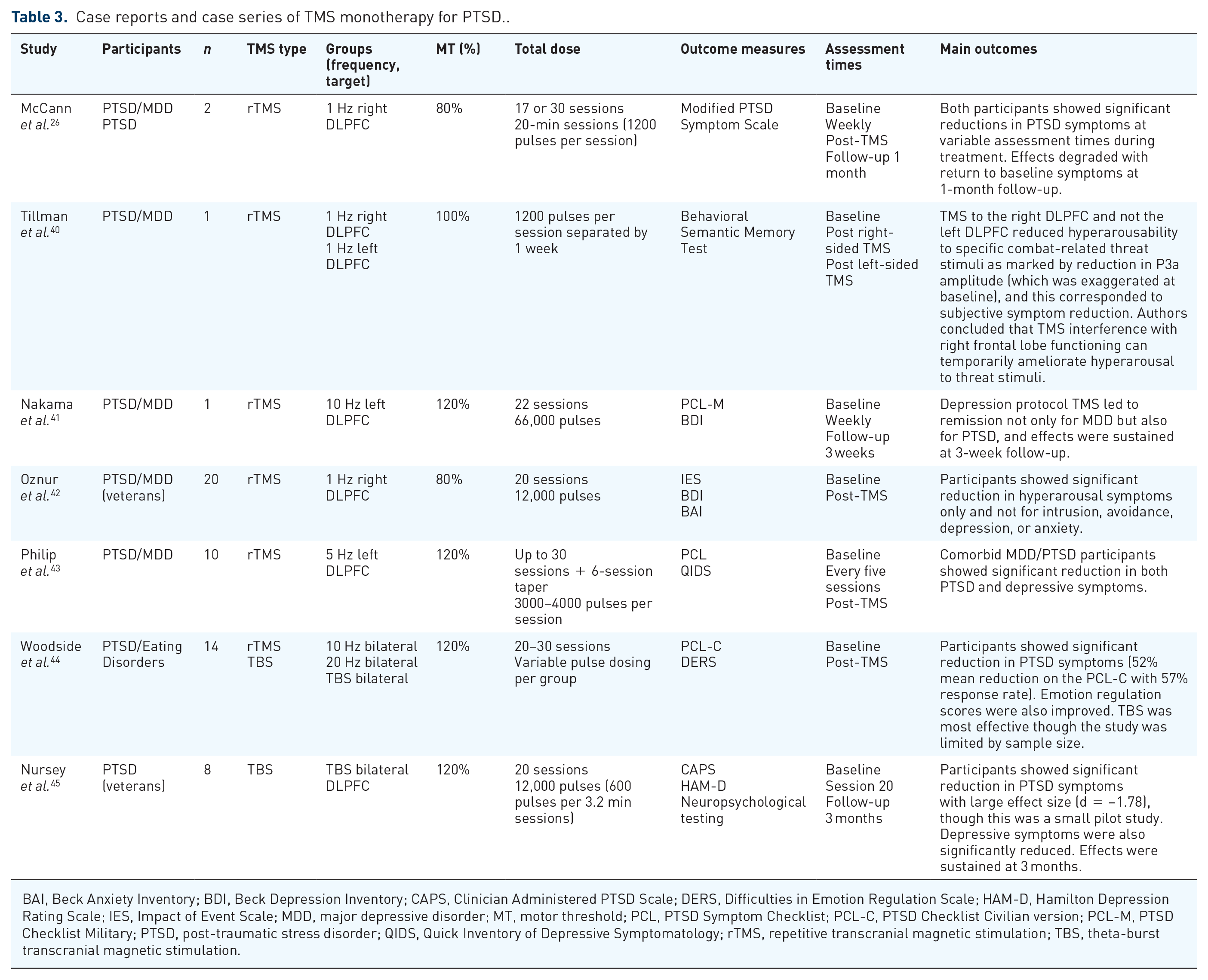
BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; CAPS, Clinician Administered PTSD Scale; DERS, Difficulties in Emotion Regulation Scale; HAM-D, Hamilton Depression Rating Scale; IES, Impact of Event Scale; MDD, major depressive disorder; MT, motor threshold; PCL, PTSD Symptom Checklist; PCL-C, PTSD Checklist Civilian version; PCL-M, PTSD Checklist Military; PTSD, post-traumatic stress disorder; QIDS, Quick Inventory of Depressive Symptomatology; rTMS, repetitive transcranial magnetic stimulation; TBS, theta-burst transcranial magnetic stimulation.
1 versus 10 Hz right-sided TMS for PTSD
Several of the RCTs utilized low-frequency 1 Hz right-sided protocols and tested it against high-frequency 10 Hz TMS, sham, or both (in keeping with the first RCT discussed above). Watts et al. 32 administered 1 Hz TMS to the right DLPFC versus sham and demonstrated significantly improved self-report PTSD symptoms (25% improvement) as well as depression, but not anxiety, with some attenuation of effect at 2-month follow-up. Notably, the total dose of 4000 pulses over 10 sessions was significantly higher compared with the 1000 pulses in Cohen et al. 29 which did not clearly outperform sham. A small RCT also compared right-sided 1 Hz TMS with sham but did so in a civilian population with a considerably higher total dose of 18,000 pulses over 15 sessions. 33 The outcome measure in the study was the CAPS and its subscales, and low-frequency TMS again showed improvement of PTSD symptoms, specifically in re-experiencing symptoms. Avoidance scores trended toward improvement and there was no difference in hyperarousal scores. Curiously, a case series published soon after also showed improvements with 1 Hz right-sided TMS but only for hyperarousal scores, with no difference for other symptom domains. 42 The study was limited by its unblinded design, however, and differed in both its psychometric (Impact of Event Scale 46 ) and sample (veterans with combat-related trauma). Overall, these studies provided evidence for low-frequency 1 Hz TMS targeting the right DLPFC in PTSD, especially with higher total doses than those used in Cohen et al. 29
More recently, a larger veteran study (n = 35) compared right-sided 1 with 10 Hz directly without a sham condition with the goal of better understanding the importance of the frequency parameter given these divergent findings. 35 Unlike the older studies discussed above, the protocol more closely resembled modern clinical practice in comorbid MDD populations with more sessions and higher total dose, in this case 86,400 pulses over 36 sessions, which was consistent between groups. Both groups showed similar improvements in PTSD and depressive symptoms at endpoint: 1 Hz response rates on the CAPS, PTSD Symptom Checklist–5 (PCL-5 47 ), Montgomery–Asberg Depression Rating Scale (MADRS 48 ), and Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR 49 ) were 29%, 43%, 36%, and 29%, respectively, versus 10 Hz response rates of 31%, 31%, 25%, and 46%. The only significant difference was superior psychosocial functioning scores in the 10 Hz group, though no difference was found on self-reported functioning scores. Ultimately, the study found no statistical advantage of one frequency parameter over the other. Notably, the authors measured outcomes up to a 3-month follow-up and the effects were sustained.
The most recent RCT, published last year by Leong et al., 38 randomized 31 civilians with PTSD into right-sided 1 Hz, 10 Hz, or sham conditions. They found 1 Hz to be superior to both 10 Hz and sham for PTSD symptoms as measured by the CAPS at endpoint, with no difference in anxiety scores. A nonsignificant statistical trend for depression was noted in favor of 10 Hz. A disproportionately high attrition rate in the sham group precluded a 3-month follow-up data analysis. Total doses (22,500 pulses in the 1 Hz group and 30,000 pulses in the 10 Hz group) were higher relative to most of the older RCTs and low-frequency 1 Hz stimulation was superior even with a lower total dose than the 10 Hz group.
Taken together, the above studies demonstrated that both 1 and 10 Hz TMS targeting the right DLPFC can be effective for PTSD, with modest evidence favoring right-sided low-frequency stimulation. Results were variable in terms of which symptoms showed improvements (i.e. core PTSD, anxiety, depression). Ultimately, they raise several important questions. Which parameters are most important in optimizing treatment: TMS total dose or frequency? Is there a therapeutic range of pulses below which there will be no treatment response, as perhaps evidenced by Cohen et al.? 29 Is there a dose-dependent effect on the duration of treatment response, with lower doses leading to degradation of effect noted months after completion of treatment, as in Watts et al.? 32 And why can both high-frequency and low-frequency stimulation (which have differential effects on motor cortex physiology) to an identical target lead to improvements in the same symptoms?
Left-sided versus right-sided TMS for PTSD
Two RCTs examined right versus left or bilateral TMS, both implementing a higher frequency protocol of 20 Hz. Boggio et al. 31 randomized 30 civilian individuals with PTSD to right, left, or sham TMS at 20 Hz for a total of 16,000 pulses over 10 sessions and found that both active groups were superior to sham for core PTSD symptoms. Right-sided high-frequency stimulation had the greatest effect (36.9% versus 23.1% reduction in total PCL scores), and subscale analysis showed better outcomes specifically for hyperarousal and avoidance symptom domains. Interestingly, right-sided TMS improved anxiety scores, whereas left-sided TMS improved depression scores, and effects were sustained at 3 months. Another RCT of TMS for PTSD included 65 veterans and compared right 20 Hz, bilateral 20 Hz, and sham TMS. 34 Bilateral stimulation consisted of 1200 pulses to the left DLPFC followed by 1200 pulses to the right DLPFC. All groups received a total dose of 24,000 pulses over 10 sessions. Both active groups showed superiority over sham with no significant difference between right and bilateral 20 Hz TMS at endpoint (response rates on the PCL were 41.2% and 62.5%, respectively). The authors highlighted quicker response in the bilateral stimulation group, with significant improvement in PCL over the right-sided group at midway point.
With evidence for the lateralization of threat processing to the right hemisphere as well as for right-sided TMS ameliorating PTSD symptoms, Tillman et al. 40 described a case report focusing on electrophysiological hyperarousability using electroencephalogram (EEG)-measured P3a amplitude in response to combat-related threat stimuli before and after left versus right 1 Hz TMS. This report demonstrated that a single session of right, but not left, TMS reduced P3a amplitude (which was exaggerated at baseline in this patient with PTSD), which in turn correlated with subjective symptom improvement. Correlating a biomarker of a core PTSD symptom, the authors argued that TMS effectively interferes with right frontal lobe functioning leading to improvement, though findings from this case report have yet to be replicated.
Several unblinded studies have examined left-sided high-frequency TMS for patients with both MDD and PTSD considering the very high rate of comorbidity, and have consistently found improvements not only in depressive but also in PTSD symptoms. In one case report, 41 a standard 10 Hz depression protocol was applied to an individual with comorbid PTSD and MDD, and this led to remission on both the Beck Depression Inventory (BDI 50 ) and the PCL. Building on prior work that showed efficacy of an intermediate stimulation frequency of 5 Hz for both depression and anxiety symptoms, two studies found significant improvement in both depression and PTSD with left-sided 5 Hz TMS.39,43 Carpenter et al. administered up to 40 sessions plus a 5-session taper to 35 comorbid participants and at endpoint showed a mean PCL reduction of 35.5% (with a Cohen’s d effect size of 1.04) and a response rate of 48.6%, with similar reductions in depression scores. Although limited by modest samples and unblinded design, these studies provide evidence for the use of left-sided TMS for both symptom domains in a comorbid population. In the latter studies, neuroimaging approaches [fMRI (functional magnetic resonance imaging) and EEG] were able to identify predictors of improvement as well as brain regions implicated in symptom change (Philip et al. 51 and Zandvakili et al. 52 for fMRI and EEG, respectively).
The above studies show that stimulation to either the left or right DLPFC at variable frequencies can be effective for PTSD symptoms; though when left versus right was tested directly at high frequency, right-sided stimulation appeared superior. Nevertheless, considering the high rates of comorbid depression in this population, left-sided high-frequency protocols traditionally used in pharmacoresistant MDD are an important option for comorbid patients, as there are significant direct improvements in PTSD symptoms even if they may be less robust compared with right-sided stimulation. Several questions are again raised. How important is laterality in TMS targeting for PTSD, and are there lateralized biological correlates to improvement in specific symptoms (e.g. P3a amplitude with hyperarousal) that can help predict response and elicit mechanism of action? If bilateral stimulation leads to quicker symptom response, might other parameters impact this also? Is achieving an early response a predictor for other measures like patient retention or duration of effect?
sTMS and TBS
Two RCTs have investigated second-generation TMS modalities in PTSD. The first was a pilot study 36 of sTMS, a unique system which uses three rotating magnets to deliver relatively low energy stimulation that is synchronized to a participant’s unique intrinsic alpha frequency. 53 Twenty-two veterans with comorbid PTSD/MDD were randomized to sTMS or sham for 20 sessions over 4 weeks with the option of an additional unblinded 20 sessions of active sTMS. Compared with sham, active sTMS showed significantly greater reduction in threshold PTSD symptoms and trended toward superiority on total PCL and QIDS-SR reductions. Greater separation between groups was noted for greater number of active treatment sessions (i.e. higher total dose).
The second study investigated right-sided TBS, another newer TMS approach which delivers triplet bursts of pulses at 5 Hz with shorter session times. 37 Fifty veterans with PTSD were randomized to active or sham stimulation for 10 blinded sessions which were followed by 10 unblinded active sessions. At the end of the 2-week blinded phase, the active stimulation group was superior in social/occupational functioning only, with no difference from sham in PTSD symptom improvement and a trend toward depression improvement. At 1 month, the active TBS group (which received at total of 20 active sessions) was superior in all three of these domains, including significant reductions in PCL and CAPS scores for PTSD symptoms. A secondary analysis showed significant reductions in anger. 54 Resting-state fMRI was performed at baseline for a convenience subset of the sample (n = 26) and ultimately demonstrated two major predictors for PTSD symptom response on the PCL: (1) increased positive connectivity within the default-mode network (DMN), and (2) increased negative connectivity (anticorrelation) between the DMN and externally oriented networks, that is, executive control network (ECN). A naturalistic clinical outcomes study over the following year showed a dose-dependent effect on duration of response, that is, sham participants (who had less cumulative TBS exposure compared with active) were 3.5 times more likely to relapse within 1 year and did so sooner (mean 182 days versus 296 days). 55 Resting-state fMRI analysis again showed that increased within-network connectivity of the DMN was predictive of better outcomes.
Another subset of this study sample had EEG performed before and after the blinded phase of stimulation in order to explore mechanism of action through electrophysiologic functional connectivity. 56 Using a machine learning classifier (Support Vector Machine), the active stimulation group was successfully identified against sham posttreatment with 75.0% accuracy based on EEG changes in functional connectivity, namely coherence in the delta band (1–4 Hz) that was decreased around the stimulation site (between right frontal and central electrodes) as well as increased around midline (between central and occipital electrodes). Aside from contributing to a growing body of literature on TMS mechanism of action, the study also raises the possibility for an inexpensive bedside technique for therapeutic monitoring.
Building on the evidence base for TBS in PTSD, a recent pilot study of eight Australian PTSD veterans receiving bilateral TBS over 2 weeks demonstrated significant reductions in both PTSD and depressive symptoms with sustained effect at 3 months. 45 Effect sizes were large (d = –1.78 on the CAPS) but should be considered preliminary given the small sample size and unblinded case series design. Of note, the TBS protocol and targeting differed from that of Philip et al., 37 consisting of twenty 3.2-min sessions for a total dose of 12,000 pulses delivered to the bilateral DLPFC (compared with twenty 9.5-min sessions for a total dose of 36,000 pulses in the active group delivered unilaterally to the right DLPFC). A recent retrospective study reported on clinical outcomes in a small number (n = 20) of patients comparing TBS (120% MT, left DLPFC, 600 pulses) versus 5 Hz TMS (120% MT, left DLPFC, 3000 pulses). 57 They found that PTSD outcomes were generally inferior in the TBS group (p < 0.011), whereas depression outcomes did not differ. However, effect sizes were generally smaller in the TBS group regardless of the outcome measure (i.e. 5 Hz TMS demonstrated superior PTSD and MDD symptom improvement, ds = 1.81 and 1.51, respectively, versus TBS, ds = 0.63 and 0.88, respectively). Effect sizes in the 5 Hz group approximated those observed in the prior study of TBS (80% of MT, right DLPFC, 1800 pulses).
Both sTMS and TBS are promising newer TMS modalities for PTSD with RCT evidence demonstrating that they are safe and effective in reducing PTSD symptoms, with the additional benefits of cost-effectiveness and decreased patient burden. Neurophysiologic measurements (fMRI and EEG) embedded in the TBS studies not only allow exploration of mechanism of action but also reveal predictors of clinical response (e.g. increased within-network connectivity of the DMN) which may help guide and individualize treatment. Follow-up studies investigating long-term outcomes, as the above 1-year TBS study, further highlight clinically relevant questions about treatment effect. For those who benefit from TMS, how long does that benefit typically last? Is the total dose the most important factor or are there other parameters that impact duration of response? How can we practically make predictions about who will benefit and sustain it?
Combination of TMS and psychotherapy
Psychotherapies including PE (prolonged exposure) and CPT remain first-line treatments for PTSD, and several studies including five RCTs have explored their combination with TMS (Table 4).
RCTs of combination of TMS and psychotherapy for PTSD.

ACC, anterior cingulate cortex; BDI, Beck Depression Inventory; CAPS, Clinician Administered PTSD Scale; CPT: cognitive processing therapy; dTMS, deep transcranial magnetic stimulation; HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale; IES, Impact of Event Scale; IPF, Inventory of Psychosocial Functioning; MPFC, medial prefrontal cortex; MPSS, Modified PTSD Symptom self-report Scale; M-PTSD, Mississippi Scale for Combat-Related PTSD; MT, motor threshold; PCL, PTSD Symptom Checklist; PE: prolonged exposure; PSS-SR, PTSD Symptom Scale–Self-Report; PTSD, post-traumatic stress disorder; QIDS, Quick Inventory of Depressive Symptomatology–Self Report version; RCTs, randomized controlled trials; rTMS, repetitive transcranial magnetic stimulation.
The first of these randomized nine individuals with PTSD to active versus sham 1 Hz right-sided TMS delivered during an imaginal exposure exercise in which the participant would speak aloud about a personalized graduated list of traumatic events or cues in a self-guided manner. 58 The theoretical basis for this protocol was the dampening of right frontal cortex hyperactivation associated with trauma re-experiencing in PTSD by using low-frequency stimulation with the goal of enhancing fear extinction. While no statistically significant difference was found between groups, the active TMS group demonstrated moderate reductions in hyperarousal symptoms on the CAPS whereas there was no improvement in the sham group. Of note, urinary and serum hormone measures were assessed; although not statistically significant, the active TMS group had increased 24-h urinary norepinephrine and serum T4 levels, and decreased serum prolactin levels at endpoint.
Another TMS technique called deep TMS (dTMS) utilizes an H-coil in order to stimulate cortical regions 3–4 cm deep (as opposed to the ~2 cm depth achieved with the standard figure-8 coil). By targeting the medial prefrontal cortex (MPFC) with this deeper reaching coil (specifically, the H1-coil), Isserles et al. 59 investigated the effects of high-frequency TMS delivered after an ultra-brief exposure procedure, theoretically enhancing fear extinction by increasing cortical excitability in the MPFC, a brain region with evidence of functional hypoactivity and anticorrelation to the amygdala in PTSD participants undergoing exposure. 63 Thirty participants were randomized into three groups to receive active or sham 20 Hz dTMS to the bilateral MPFC: (1) active dTMS after trauma exposure, (2) active dTMS after nontrauma exposure, and (3) sham dTMS after trauma exposure. A brief exposure procedure involving a 30-s audio script of a personal nontraumatic versus traumatic life event plus a silent imaginal period was done immediately before each of the 12 dTMS sessions. Compared with both control groups, the active dTMS after trauma exposure group showed a statistically significant improvement in intrusive symptoms on the CAPS (response rates of 44% versus 12.5% and 0%) with a correlated reduction in heart rate response to traumatic scripts. Significant within-group reductions in total CAPS, avoidance, and hyperarousal measures were shown in the active group only. Effects were sustained at 2 months. The study’s small sample size and lack of a fourth control group (i.e. sham dTMS after nontrauma exposure) likely limited the detection of statistically significant differences across multiple outcomes. A follow-up evaluation using a different coil (H7), designed to have greater targeting over the dorsomedial PFC, was recently published. 62 Similar to the prior report, all participants received brief exposure, and results indicated that active stimulation was inferior to sham at 5 and 9 weeks. This finding, which was in the opposite direction than expected, raised important questions about the efficacy of the ultra-brief exposure intervention as well as whether active dTMS with the H7-coil may interfere with trauma memory-mediated extinction, possibly due to differential relative stimulation of target regions.
A small pilot RCT was recently published on simultaneous PE with left or right 10 Hz versus sham TMS. 61 Eight participants completed an adapted 8-week PE course plus once weekly TMS, during which time they listened to an audio recording of their PE session. A nonsignificant trend in PTSD symptom improvement on the CAPS favoring active treatment was noted (55% versus 40% reductions), though the study was not powered for clinical outcomes. They did note that adherence was good (67%) and this represents important feasibility data.
A single RCT has combined TMS with CPT, another gold-standard psychotherapy for PTSD in which traumatic memories are elicited and patients are supported through direct confrontation of conflicts and maladaptive beliefs associated with their memories. 60 The authors randomized 103 PTSD veterans to active or sham 1 Hz TMS to the right DLPFC performed immediately prior to 12–15 weekly CPT sessions (standardized using the CPT Veteran Military Version manual). While both groups showed significant reductions in PTSD symptoms on the CAPS and PCL, the active stimulation group was statistically superior with a clinically meaningful difference. Depressive symptoms were reduced in both groups with no advantage of active over sham, which the authors pointed out was unsurprising given a underpowered protocol for depression treatment (i.e. once weekly TMS sessions); 57% of participants completed the 6-month follow-up, and the effects were sustained in this group. Overall, the authors concluded that TMS-augmented CPT produced meaningfully greater treatment of PTSD symptoms. Of note, the treaters were not blinded to groups and the sham coil did not produce somatic experience of active stimulation.
In their totality, these studies demonstrate the feasibility and tolerability of combining psychotherapy with TMS. These data are also mixed (e.g. discordance between the original dTMS and its follow-up study), though the general pattern appears to support combined use with a possible additive effect. Complicating this assessment, however, are the variable abbreviated exposure therapy protocols used in several studies, raising the question of whether standardized psychotherapy, which adds to patient burden and requires therapists with specialized training, is necessary or would result in even greater reductions in PTSD symptoms when combined with TMS. Furthermore, while different mechanisms of action for the enhancing effects of TMS on psychotherapy are proposed (augmenting fear extinction by decreasing right frontal cortex hyperactivity or increasing MPFC hypoactivity with downstream effects), the studies have lacked assessment of corresponding biomarkers.
Discussion: designing future studies for TMS in PTSD
This review of TMS both as monotherapy and combined with psychotherapy for PTSD focused on the evidence for its use while raising pertinent questions meant to guide future directions for researchers and clinicians. TMS in this population was widely demonstrated to be safe and tolerable with significant and clinically meaningful reductions in core PTSD symptoms shown in multiple studies with a highly diverse set of stimulation protocols. To date, six meta-analyses on TMS for PTSD have been published, the more recent of which adopt broad inclusion criteria meaning most of the studies discussed above, including those without control groups, are part of their samples.16,64–68 The most recent meta-analysis included 19 studies (376 participants) and revealed a large positive effect of TMS on PTSD symptoms: d = 1.17, 95% confidence interval (CI) = [0.89–1.45], p < 0.001. 64 There was a wide range of effect sizes across studies with the majority evenly distributed between d = 0.08–1.97, and high heterogeneity indicating unexplained variance in the studies. The authors analyzed a number of moderating factors and found high-frequency TMS to be superior to low-frequency TMS (d = 1.44 versus d = 0.72, p < 0.001) but no difference in effect sizes based on categorical total pulses or brain target/laterality. However, the high degree of variability between included studies (frequency, doses, targets, stimulation type, monotherapy versus combination, psychometrics, length of follow-up, sample size, comorbidities, veteran status, trauma type, etc.) complicates making direct comparisons and drawing simple conclusions in meta-analyses.
While it is encouraging that TMS appears to be safe and effective despite the many different approaches, the literature shows important areas of opportunity. First, very few studies have had biomarkers which are crucial for better understanding two of the most important questions raised: who responds to treatment, and why is treatment effective for them (i.e. mechanism of action)? Studies have primarily been empirical so it is difficult to interpret negative (or positive) findings. Yet, even simple biomarkers such as EEG have demonstrated the ability to detect and even predict TMS response, and have the potential for a low-cost acquisition to inform observed clinical changes. 56 There has also been significant progress in the neurobiology of PTSD and its treatment, with functional imaging correlates of key pathophysiologic elements, including threat extinction, safety learning, and affective regulation (for a review of the neurobiology of PTSD, see Koek et al. 12 ). Since brain regions implicated in PTSD include deep and subcortical regions (e.g. amygdala), imaging modalities that are well suited to detecting changes in these zones are likely to be needed. To our knowledge, there has only been one imaging study to date showing that PTSD symptom response at the individual and group level could be predicted by baseline functional imaging of the amygdala. 51
It is important to note that the therapeutic targets of TMS for PTSD have largely been justified by empirical evidence and some theoretical consideration, rather than directly utilizing neural network pathology. It is our hope that functional imaging can be used to clarify and validate optimal stimulation targets. As described above, what is now the most studied target for TMS in PTSD, the right DLPFC, is utilized mostly based on successes observed while developing TMS for depression (which have largely but not exclusively focused on the left DLPFC), as well as functional imaging evidence of right-sided hypermetabolism with trauma/fear-processing in PTSD patients. We now better understand the role of the DLPFC as an important region in the ECN that subserves cognitive flexibility and emotion regulation, and stimulation to this target may enhance the top-down regulation of affective circuits, though an exact mechanism remains unclear (reviewed in Koek et al. 12 and Trevizol et al. 68 ). The other major target for PTSD is the MPFC, another region of the ECN more specifically associated with regulation of the fear response. As discussed above, the MPFC has been shown to be functionally anticorrelated with the amygdala, a crucial region that is hyperactive in PTSD participants undergoing trauma exposure, and furthermore ventromedial PFC activation during extinction learning has been shown to be associated with exposure response. 12 For a recent review of defining brain stimulation targets in PTSD via functional imaging, see van Rooij et al. 69 How best to leverage that knowledge remains an important area of inquiry, perhaps demonstrated by the initial success in reducing PTSD symptoms using dTMS stimulation to the ACC (anterior cingulate cortex)/MPFC, 59 yet a similar approach (with admittedly a different TMS coil) yielded countertherapeutic effects when examined with a multisite RCT. 62 Furthermore, important questions about whether there are optimal forms of TMS delivery to reduce PTSD symptoms (once or multiple daily TMS sessions, etc.) remain to be answered using rigorous study design.
Several other empirically based questions remain as well, notably around TMS parameters as well as clinically relevant outcome measures. Relatively few studies have examined protocols head-to-head in RCTs in order to determine the effect of frequency (1 versus 10 Hz studies described above; e.g. Kozel et al. 35 ) and these have excluded other protocols such as 5 and 20 Hz. Total dose has varied considerably between studies and in some cases even between groups of different frequency protocols within studies. Additional studies controlling for this variable are needed in order to determine whether it may impact efficacy or other clinically relevant outcomes such as durability of response (e.g. Petrosino et al. 55 ), or speed of response as shown in a recent study of accelerated TBS for depression which delivered five times the usual dose over 1 week and quickly achieved very high remission rates. 70 Newer TMS modalities like sTMS and TBS are also promising for PTSD but remain to be compared directly with more traditional TMS in prospective trials. Furthermore, whether multiple daily treatments (i.e. accelerated TMS) improve outcomes remains unstudied in this area.
Duration of treatment response to TMS for PTSD is a clinically relevant outcome that deserves additional investigation, as the majority of studies ended at 2- or 3-month follow-up, and only a single study has looked at long-term outcomes over 1 year. 55 Regarding specific outcome measures, many groups have analyzed the effects of TMS on PTSD symptom clusters such as hyperarousability and intrusive symptoms, yet no conclusive patterns have emerged. This likely reflects the limits of our current phenomenological diagnostic schemes and again compels the next generation of studies to utilize neurobiological markers to help guide more accurate disease classification (i.e. biotyping) and more targeted treatment (for a review and implementation of novel methods in this content area within PTSD, see Akiki et al. 71 and Zandvakili et al. 72 ).
Finally, the combination of TMS with psychotherapy has shown promising effects for PTSD in preliminary studies. Still, the methodologies are highly variable with several different TMS parameters and only two of the studies implementing standardized psychotherapy (versus brief exposure procedures). In order to more definitively conclude on the additive and possibly synergistic effect of TMS with psychotherapy, as well as feasibility in the real-world clinical setting, it may be useful to study well-established therapy protocols. No combination studies to date incorporate biomarkers despite a neurobiological basis for the augmentation approach (e.g. stimulating a hypoactive MPFC, the activation of which predicts successful ‘top-down’ modulation of the exaggerated amygdala response in extinction learning). These biomarkers are therefore crucial, not only for the aforementioned reasons in monotherapy TMS but also insofar as they are directly relevant to the psychological modalities. In closing, TMS for PTSD appears to be safe and effective, but important steps remain to be taken to confirm its efficacy and demonstrate meaningful changes to the underlying pathology.
Footnotes
Author contributions
Drs. Philip and Petrosino designed the overall paper and performed the literature search. Drs. Cosmo, Berlow, Zandvakili, and van t’-Wout-Frank assisted with interpretation of the results. All authors materially participated in manuscript preparation and all authors have approved the final submission. This manuscript is not submnitted to another journal and all relevant support and conflicts are provided.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no relevant biomedical conflicts of interest to disclose. In the last 3 years, Dr. Philip has received clinical trial support [through Veterans Affairs (VA) contracts] from Wave Neuro.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the US Department of Veterans Affairs (VA; I01 RX002450, I01 HX002572), the National Institutes of Health (NIH; R01 MH120126, P20 GM130452, and R25 MH101076), and the VA Office of Research Rehabilitation and Development (RR&D) Center for Neurorestoration and Neurotechnology at the VA Providence Healthcare System (I50 RX002864). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the VA or the NIH. The funders had no role in the design of the study, data analysis, or decision to publish.