
Abstract
Research has generated good quality evidence about the treatment and management of bipolar disorder in acute and, to some degree, sub-acute/continuation phases. This has informed various guidelines about the treatment and management of bipolar disorder (BD). However, for the long-term or maintenance phase of illness, most guidelines peter out and, in the absence of sufficiently high-quality research evidence, remain vague. This is particularly evident for the important clinical question of discontinuing mood stabilizing pharmacological agents after a period of remission has been achieved. The aim of this review is to put together current existing evidence about discontinuing mood stabilizers after a period of remission in order to come up with a structured and coherent strategy for managing such discontinuation and to make recommendations for future research. To this end, we reviewed the main relevant treatment guidelines and subsequent evidence following the publication of these guidelines. The current recommended long-term treatment of BD is usually considered within the same principles applicable to any chronic health condition (e.g. hypertension or diabetes) where the focus is on continuing treatment at minimum effective medication dose often life-long, switching to alternative choice of medication due to side-effects and very few, if any, indications for complete cessation. However, in the absence of strong evidence on long-term treatment and the high rate of non-concordance in BD, medication discontinuation is a very important aspect of the treatment that should be given due consideration at every aspect of the treatment.
Keywords
Introduction
Discontinuing a medication that has shown benefit in an illness as multifarious as bipolar disorder (BD) is perhaps one of the most difficult questions in current psychiatric clinical practice. It invokes a clinician’s fear of their patient relapsing fairly quickly and returning to the proverbial square one of treatment – that is, acute manic or depressive phases.
In BD, the question of treatment is a complex one and is usually divided into acute (Ac), continuation (Co) and maintenance (Mn) phases: the first geared towards symptom resolution, the second towards sustaining remission and the last towards relapse prevention.1–7
For most other disorders, this model would be a straightforward one, for it would involve either presence of the disease or its absence. But for this polar affective illness, the idea of remission from one affective state is a concern – for always in a clinician’s mind as their patient’s mood state improves is the worry of transition into the other. This is illustrated in Figure 1.

Different phases of treatment in BD. Here depicted in the depressive pole. Modified from Frank et al. (1991) by Grunze et al. (2013) (Grunze, Vieta and Goodwin, 2013).
Pharmacotherapy for BD performs really well in clinical trials across the board in terms of symptom remission, maintenance of remission and a higher rate of relapse and subsequent treatment resistance on discontinuation. However, if this success is subjected to further scrutiny, it transpires that:
In terms of individual pharmacological agent, lithium has the strongest evidence for long-term relapse prevention; with the evidence for anticonvulsants such as valproate and lamotrigine, evidence is less robust and uncertainty of any longer-term benefits of antipsychotics exists 9 ;
In terms of mood polarity, the evidence is strongest for the efficacy of pharmacological management for management of acute mania and mania prophylaxis but equivocal for bipolar depression, rapid cycling and subsyndromal states.1,10 This is of particular importance considering that depressive symptoms consume the majority of the lives of patients with BD, with one study reporting patients with BD having residual depressive symptoms for about a third of the weeks of their lives11,12;
In terms of treatment phase, the current evidence stands the strongest for acute phase of the illness. However, trials like STEP-BD show a rate of recurrence of mood episodes within 2 years as high as 49% despite acute response to treatment. 13 Others quote a relapse rate of 37% at 1 year and 60% in 2 years and a 5-year risk of 73% of either polarity despite continuation of treatment. 14
In terms of patient response factors, since genome-wide association studies (GWAS), 15 it is becoming more apparent that not every patient will respond to same combination of pharmacological agents – in particular the universally acclaimed lithium. 16 In fact, a very niche cohort of patients will show the ideal treatment response (see Figure 2) hailed for lithium in BD: those with fewer hospitalisations preceding treatment; an episodic course characterised by an illness pattern of mania, followed by depression and then euthymia; and a later age at onset of BD.17,18

Phases of index mood episode with complex interplay of treatment duration and discontinuation considerations. (1) Acute side effects, (2) chronic/long term side effects, (3) patient choice (usually on symptom remission), (4) clinician led (e.g. simplification of regimen, TEAS, switch to opposite pole), (5) inadequate response, (6) emergence of new physical health conditions (e.g. renal or cardiac illnesses). For definition of study abbreviations, see main text.
Treatment-emergent affective symptoms (TEAS) and subsyndromal mood fluctuations during remission make it difficult to fully gauge treatment efficacy and response. This is further confounded by the fact that maintenance trials often follow an enriched design where only patients who have remitted under the trial agent during the acute phase are enrolled into the double-blind maintenance phase, which creates biases towards specific treatment and response. 19 Most maintenance trials do not extend beyond a 2-year follow-up period, 20 while their findings are used to recommend potentially life-long treatment in almost all practice guidelines. And while discontinuation trials clearly demonstrate rapid relapse on discontinuation versus staying on the therapeutic agent, up to 87% in a period of 10 months following 5-year stable period of remission, 21 these data need to be interpreted with caution considering the likely confounding of ‘rapid relapse’ following discontinuation with withdrawal effects of the mood stabilizer, in particular lithium as discussed in detail below. 22
Rates of non-concordance to treatment in bipolar settings remain extremely high, 23 in one study being 50%. 24 Psychoeducation and therapeutic alliance may possibly mitigate this but, in reality, throughout the course of any long-term illness many patients decide to come off treatment all together. With our knowledge of increased rate and severity of relapse with abrupt rather than slow discontinuation, 25 it is prudent to consider discontinuation strategies as an equally important part of any management plan rather than insisting on lifelong compliance and being left with a patient who then just decides to abruptly come off everything altogether.
This is then further complicated by the fact that the effects induced by discontinuation – in particular that of lithium – are very poorly understood due to the high overlap between these effects and mood symptoms (as shown in Table 1). This then raises the question of whether these are relapses induced by discontinuation of treatment, or true withdrawal-rebound phenomenon not associated with relapse, or subsyndromal mood fluctuations characteristic of the illness itself? Perhaps one? Or all? Or none? Perhaps these are effects associated with comorbid illnesses that run with the Bipolar cycle like personality disorders or substance misuse? The lack of understanding in this area is perhaps related to our lack of full understanding both of the neurobiology of the illness thereby having no validated pharmacological targets, and the mode of action of the mood-stabilizing medication. This has led to repurposing of neuropsychiatric medications like antiepileptics for the management of mood disorders, leading to Geddes et al.’s proposed suggestion of also perhaps recognizing the role of serendipity somewhere in the management. 9
The curious case of mood stability: the complex overlap of illness symptoms, remission symptoms, pre-morbid and comorbid symptoms, and treatment withdrawal rebound echoes the Parmenidean principle of ‘all is one’ and highlights our current gap in knowledge of how to clinically tell them apart.

ADHD, attention deficit hyperactivity disorder; EUPD, emotionally unstable personality disorder.
The questions of how, when or why to discontinue pharmacological treatment in BD are a major challenge in psychiatric clinical practice, and are best approached based on risk-versus-benefit assessment and an approach tailored to the individual patient in question. 9
This is best expressed in Hamlet’s iconic reply to his friend Horatio in William Shakespeare’s titular play.
‘We defy augury. There is special providence in the fall of a sparrow. If it be now, ‘tis not to come, if it be not to come, it will be now; if it be not now, yet it will come – the readiness is all’. (Hamlet Act 5, scene 2, 217–224)
Hamlet is uneasy about participating in the ultimate sword fight challenge by Leartes, and Horatio advises to sue for postponement. Hamlet, however, brushes this aside, comparing his uneasiness with augury – an omen that he should not go through with this duel. He carefully takes stock of all his options and all possible outcomes of this duel, which is the metaphor for the discontinuation question we have at hand, and decides that fighting now and hoping for a clear victory due to superior swordsmanship is his best course of action given the circumstances. He says he would rather dismiss this uneasiness that he is experiencing and face the duel with all readiness.
And we discover that, based on the facts he possessed, he made the right call and did win that duel.
However, as Shakespearean tragedy would have it, factors unknown to him then impel this to a pyrrhic victory for our hero.
And here we are like Hamlet – taking stock of all that is known about if, how, when and why to discontinue mood stabilizers to provide clinicians with some guidance to defy their own uneasiness and make the best possible decision with their patients. However, in hopes of avoiding a re-run of Hamlet’s fate, we will also be giving due credence to the gaps in our current evidence and understanding – the great unknown – and making recommendations for future research.
Why discontinue?
Lithium (Li), antiepileptic drugs (AED), and antipsychotics/dopamine antagonists (DA) perform well in clinical trial settings. However, in naturalistic studies, a much lower efficacy is reported, 36 and even this diminishes over time, with some authors concluding that it may not be possible to achieve long-term stability with Li.21,37 Perhaps one of the reasons for this is that the research criteria for long-term response is usually measured in time to recurrence, number of relapses, time spent in hospital or severity of subsequent episodes, and is perhaps only a fraction of the naturalistic response. 38 The latter is heavily dependent on other factors like polypharmacy, compliance, and disease course before administration of medication, to name but a few. 38
The efficacy of long-term pharmacological treatment has been held under scrutiny and critique by multiple clinicians and researchers alike. One of the reasons for this is the overall modest effect of treatment on mania and none on bipolar depression, 39 and the fact that there are no long-term randomised control trials (RCTs) to compare no pharmacological treatment (essentially untreated cohort of bipolar illness) with treated cohort. 40 There are some who consider the disorder a recent ‘disease-mongering’ ploy by pharmaceutical companies39,41; however, this notion has been contested due to the historical records of melancholia and mania as far back as the Greek Iliad. 42 There is also the argument that post Falret’s description of la folie circulaire in 1864 and later formalization of BD as a diagnosable mental illness, there were hardly any formal diagnoses of the illness in US until 1970, which coincided with the introduction of lithium as a pharmacotherapy. 39 In one study, Harris et al. compare patterns of service utilization in BD in the 1890s (considered pre-lithium era) and the 1990s. 43 They found that, in the 1890s, admissions for BDs occurred at a rate of 4 every 10 years, and in 1990s at a rate of 6.3 every 10 years. Where 100 years ago, there were 16 bipolar patients per million population resident per day in hospital, there were 24 per million residents in acute service beds and more in non-acute beds in 1990 in North Wales. 43 This, along with the increased incidence of diagnosis in paediatric population, 44 is taken to be indicative of both the detrimental nature of pharmacological treatment on the natural course of bipolar illness and BD as a diagnosis being a modern construct to supplement gains of pharmaceutical companies.
The authors advise readers to interpret all evidence – particularly historical evidence, as in this case – with the greatest of care since psychiatric clinical and research practices have changed greatly over the course of history and cannot be generalized for the purpose of comparison. By way of example, in the 1890s psychiatric inpatient admissions were far more protracted and community mental health services scarce; and hence comparison of number of hospitalizations based on the modern concept of reducing bed days and expediting discharge following symptom control for management by community teams is inconsistent.
Some more recent studies do bring up evidence that raises important questions regarding the efficacy of BD treatment. This is particularly the case when looking into treatment-related harm. The top two reasons for mortality in BD patients are physical health side effects, in particular metabolic syndrome and suicide,45,46 mainly in the depressive phase of the illness. Storosum et al. investigated whether there is a greater suicide risk in the placebo arms or treatment arms of acute manic episode and the prevention of manic/depressive episode by analysing 11 placebo controlled Dutch RCTs and found eight completed suicides in treatment versus two in the placebo group, with risk of completed suicides 2.22 times higher in the treatment group.39,47 While the Dutch study concluded this to show that placebo-controlled trials were safe to conduct, their findings do raise the question of long-term efficacy of pharmacological treatment, particularly the light of growing body of evidence that there is limited effect in bipolar depression, which is when most completed suicides occur. In another study by Joukamaa et al. it was found that the risk of premature deaths as a result of physical health complications in neuroleptic treated population was 2.5 per increment of one neuroleptic. 48
Discontinuation is largely assumed to be an issue of the post-remission period of bipolar illness. However, there are myriad reasons cited in literature for patients or clinicians opting to discontinue a mood stabiliser in more acute phases of illness. These include development of side effects, both acute and long term, patient choice on symptom remission, due to partial or inadequate response, emergence of new physical health condition (e.g. cardiac or renal illnesses) or clinician led (e.g. simplification of regimen in maintenance phase, treatment-emergent affective symptoms or relapse) 23
Discontinuation can be divided into the following sub-categories, each in relation to the three phases of treatment of BD (see Figure 2).
(a) Acute side effects
(b) Chronic/long term side effects;
(c) Patient choice (usually on symptom remission);
(d) Clinician-led [e.g. simplification of regimen, treatment emergent affective switch (TEAS)];
(e) Inadequate response;
(f) Emergence of new physical health conditions or their related drug interactions;
(i) Chronic/progressive (e.g. cardiac or renal illnesses);
(ii) Transient/self-limiting (e.g. pregnancy, breast feeding, drug overdose/self-poisoning).
Fuzzy logic of discontinuation and the curious case of mood stability
What is mood stability in BD? In Kraepelinian terms, this is a clear distinction between either poles that is consistently sustained, as indicated by the ideal response curve in Figure 2. 26 However, both from clinical experience and a growing body of evidence we now realize that mood stability or ‘episode resolution’ includes persistent symptoms. These symptoms have been a long-neglected part of bipolar research, to the extent that there might not even be a proper terminology to describe them. 27 ‘Inter-episode mood instability’, ‘subsyndromal mood fluctuations’ and ‘residual symptoms’ are some of the terminologies that have been used to describe these persistent fluctuations. There is also growing understanding that these symptoms vary depending on the predominant mood state of the illness, 28 with a prevalence as high as 68% or 47.3% of symptomatically ill weeks throughout a mean of 12.8 years 29 ; with depressive symptoms more predominant than hypomanic/manic or mixed symptoms.
As shown in Figure 3, the argument between continuing and discontinuing is one of fuzzy logic rather than a clear bivalence as perhaps treatment of hypertension – take the medication and a control is achieved, and vice versa. The problems associated with discontinuation are akin to Schrodinger’s cat paradox, which posits that without opening the box, i.e., add the observer to the quantum state, one can never truly know whether the cat is alive or dead. There appears to be a historic assumption that lithium could be stopped abruptly because it did not induce any withdrawal effects. 49 However, lithium is shown to have clear withdrawal effects not related to relapse of primary illness. 30 This was perhaps first demonstrated by Bunney et al. in 1968 when patients in the placebo arm of abrupt lithium discontinuation had an increased mania reading even if the placebo period lasted for only a day. 30 In the case of lithium, some of the withdrawal effects reported in literature include anxiety, irritability and sleep disturbances,25,30,32,49,50 symptoms that are also consistent with withdrawal from other psychotropic medications. Blockade of the development of supersensitive dopamine receptors; changes in neuronal membranes, cell transport function or other neurotransmitter systems; rebound increase in noradrenaline; and psychogenic-anxiety due to the discontinuation of an effective medication have been suggested as possible explanations of the lithium withdrawal phenomenon. 30

Fuzzy logic: for a disorder that oscillates between two extremes of symptoms there is little surprise that decisions around treatment be equally convoluted and may perhaps never balance and add up to 1. The figure summarises current understanding of the rationale for each treatment approach.
In terms of the discontinuation question, this problem is further complicated due to the heavy overlap of symptoms as illustrated in Table 1. Once a mood stabilizer like lithium is withdrawn and a set of symptoms like irritability, anxiety and changes in sleep emerge, it comes down to laws of deduction to deduce what this could be: subsyndromal fluctuation inherent to the disease course? Or relapse? Or perhaps prodrome to lapse in the opposite pole? Or pure lithium withdrawal?
Pure withdrawal and relapse will have to demonstrate a clear temporal association with discontinuation, whereas subsyndromal states would precede it. However, there are no clear time-cutoffs to delineate withdrawal from early/prodrome symptoms that are specific for mood stabilizers, in particular lithium. However, a classification system for withdrawal symptoms of selective serotonin reuptake inhibitors (SSRIs) proposed by Chouinard and Chouinard would suggest peak of onset between 36 and 96 h and resolution by 6 weeks. 52 This was later used by Cosci and Chouinard to review withdrawals in all psychotropic medications. 32
Despite all this there is danger of oversimplification and falling into the trap of the logical fallacy post hoc ergo propter hoc.
There is a need for clear definitions and broadening our current knowledge of subsyndromal mood fluctuations. There has been some work of significance done in this area by using naturalistic study models like ecological momentary assessment (EMA) and their recent upgraded use via smartphones for continuous daily monitoring. There is further need for standardised diagnostic measures to differentiate between drug withdrawal effects, subsyndromal fluctuation and relapse.
And now to the final problem of the ‘to continue or discontinue’ conundrum, which is non-response or treatment resistance to previously effective treatment. This is a usually cited as an argument against discontinuation due to discontinuation-induced refractoriness, where following a good long-term response, patients discontinue lithium, suffer a major recurrence, and then do not again respond as well or at all to lithium once it is reinstituted at previously effective doses, despite therapeutic levels. 52 However, non-response is now understood to be a composite of two distinct phenomenon, of which refractoriness post discontinuation is only one. 52 The second is acquired tolerance and the association with reduced response over time, 53 and perhaps even further aggravation of subsyndromal mood states and relapse. However, studies in this area are mired by small sample sizes (often case reports or series) and lack of adequate longitudinal or naturalistic data 52 ; both of these together contribute to treatment resistance over time.
Parameters
Mood Stabilisers
The term mood stabilisers cover three broad categories of medication: Li, AED, and antipsychotics/DA. Their biological mechanisms of action and receptor profile are distinct from one another, and anticonvulsant action is not necessary for mood stabilization. In most guidelines, antipsychotics are not recommended beyond the acute phase of treatment. However, in reality, most BD patients tend to be continued on a combination of Li/AED and DA for long-term management, which is why we have included all three under the somewhat outdated term of mood stabilisers in this review.54–56
Discontinuation
Discontinuation may imply stopping one pharmacological agent while still being on others (in combination therapy regimens) or of switching to others (in monotherapy regimens). It can also imply complete cessation of all pharmacological treatment (often in the maintenance phase but it can happen in any treatment phase). For the purpose of this review, we have considered and tried to address all scenarios of treatment cessation.
Current evidence on how to discontinue
Table 2 lists suggestions from recent clinical practice guidelines for discontinuing mood stabilisers. In summary, they suggest: don’t; only if you must; do it slowly; and keep following the patient up.
Discontinuation recommendations by major guidelines.

Considering treatment-emergent episodes, TEAS and the long-term relapsing-remitting course, maintenance treatment should be indefinite (lifelong) after the diagnosis of BD has been confirmed.19,57,58 There are no data concerning the optimal duration of maintenance treatment. Some practice guidelines recommend ongoing treatment for a period of between 2 and 6 months after the full resolution of symptoms of an acute phase of illness (i.e. remission of index affective state). This is followed by a continuation phase that is poorly differentiated from maintenance phase except that, in the continuation phase the regimen that achieved remission is continued and in maintenance phase it may be switched to lithium as first line or further simplified to one or two mood-stabilising medications in combination. The maintenance phase is then recommended to be lifelong, with a recommendation to carry out 6-monthly or annual clinical reviews, but there is little concrete guidance on discontinuation. All guidelines agree on lithium being first line for long-term maintenance because it is the gold standard, which is usually well tolerated. If needed, it may be combined with other medications such as valproate, lamotrigine, aripiprazole, quetiapine and olanzapine
Most guidelines agree that the only consideration for discontinuing long-term mood-stabilising medication is as a risk versus benefit decision. If the adverse effects outweigh the benefit of continuing medication, then a switch to a different mood stabiliser is recommended over complete discontinuation. However, if the side-effects are intolerable or adherence poor, or there is a gradual lack of efficacy, then there is recommendation for cautious discontinuation in certain circumstances (Figures 4 and 5). These include, extremely low-risk cases or where risk is not clearly established (e.g. first episode mania with no prior affective episode, no family history of BD). If present, then a trial of discontinuation might be attempted. There is no consensus on the duration of the continuation phase prior to gradual discontinuation but suggestions vary from 6 months to 2 years after symptom remission.
The current recommendation for slow discontinuation is to reduce slowly over (at least) 4 weeks with robust data for less risk of severe manic relapse if lithium is tapered very gradually.25,60 This has also been demonstrated for DAs and other psychotropics, although less robustly than for lithium. 61 This has been explained variously in the literature to be a combination of long-term individual pharmacodynamic adaptations to the presence of the drug, 62 leading to neuropharmacological adaptations that include changes in postsynaptic receptor and auto receptor sensitivity, neurotransmitter synthesis and release, and various downstream molecular and genetic mechanisms in multiple brain systems.22,25,63,64 These neurobiological adaptations then lead to physical and sensory phenomenon that become manifest when treatment is abruptly removed, being less severe for treatments with longer half-lives. 63 This is shown to resolve if the treatment is briefly reinstituted, even at much lower doses than were previously therapeutic. 63 This has led to the widely accepted recommendation of slow withdrawal to allow for neurobehavioral readaptation to the psychotropic drug.63,65,66
After discontinuation, the consensus is for the patient to keep receiving regular follow up, ideally by secondary mental health services rather than being discharged back to primary care practitioners. If resources do not allow for such, there should be a low threshold for being seen promptly by secondary psychiatric services in event of recurrence of illness signatures. Newer reports suggest that discontinuation in the absence of medical consultation/follow up leads to more admissions. 60
Current practice guidelines for discontinuation can be seen to have gone in reverse for perinatal psychiatry, where previously both pregnancy and breast feeding were considered one of the few strong indications for discontinuation due to both maternal and neonatal physical health risks. 67 However, there is growing body of evidence that suggests minimally increased to no increased risk of foetal malformations or neonatal physical health sequelae with continued treatment,67–69 weighed against increased risk to both mother and baby in case of untreated illness and relapses.70,71 Therefore the current body of evidence around mood stabiliser (in particular lithium) and management of puerperal affective syndromes leans towards continued treatment or transient antepartum discontinuation with immediate reinstatement postpartum rather than complete cessation of treatment.

Algorithm for indication for maintenance treatment (Dutch guidelines (Nolen et al. 2008 (Nolen, Kupka and Schulte, 2008)) from Grunze et al. (2013)(Grunze, Vieta and Goodwin, 2013) 59
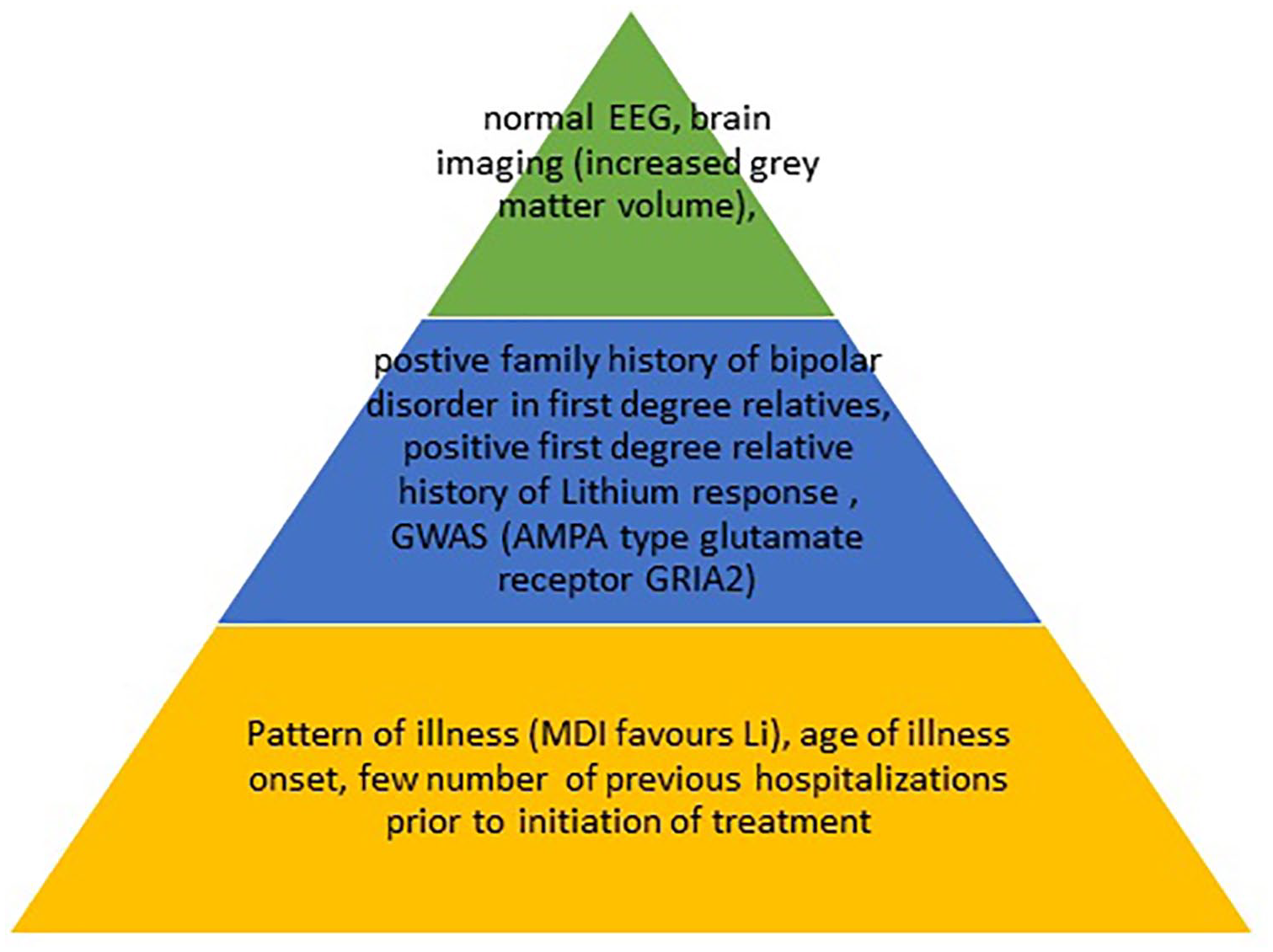
Predictors of lithium response from Tighe et al. 16 and Kleindienst et al. 17 If the patient fits this particular cohort perhaps there is great value in advocating and continuing on lithium in the long term, even indefinitely. For all other combinations of patient and disease factors, discontinuation of pharmacologic treatment should be approached with an open mind due to lack of robust evidence supporting continued treatment. The green tier corresponds to weak evidence, the blue tier with moderate and the orange tier with strong evidence. MDI pattern is a positive predictor of response, while the DMI pattern was negatively correlated with lithium response.
The proposed plan
This should be based on a risk-versus-benefit evaluation of treatment for a chronic life-long illness (Figures 6 and 7). This should also include a full understanding of the BD specific to the individual patient. For example, a patient with early onset illness, predominantly depressive polarity with subsyndromal symptoms, features of rapid cycling, high risk of metabolic syndrome, concomitant substance misuse, multiple compulsory hospital admissions due to relapses and no first-degree family history of BD have almost no factors in their illness to recommend continued long-term treatment (Figure 5). In such a case, there is more to recommend a safe graduated discontinuation regimen rather than abrupt discontinuation in order to mitigate risks.

Discontinuation due to side-effects algorithm, where complete cessation of all treatment is not anticipated.

Proposed discontinuation algorithm for complete cessation of all treatments.
When there is a need to discontinue medication, then current evidence suggests slow discontinuation over a period of (at least) 4 weeks or more – in the case of lithium up to 3 months – and robust monitoring of mental state for earliest signs of relapse. This can be extended in the case of lithium to not be more than a decrement of 0.2mmol/l in serum levels at any given time. Monitoring should be every 1–2 weeks by a mental health professional with a robust formulation of acute treatment plan in case of relapse. 63 This is particularly important because newer findings suggest that having a medical follow up after discontinuation is very effective is reducing severe deterioration and admissions. 60 In a combination regimen scenario, the discontinuation strategy should be aimed towards stopping lithium only as the last resort.
Discussions around prospective discontinuation of treatment with patients should take place proactively in clinical settings. This can help in short-term compliance and negotiation of treatment goals. 79 Many patients are more likely to consider adherence if there is an ‘end in sight’ than to be told that they must take the medication indefinitely. 79 This helps with building a therapeutic alliance and prevents the covert and abrupt discontinuation, which is associated with more negative outcomes than a graduated and tapered approach.80,81
The focus of discontinuation of treatment is a clear understanding by both clinicians and patients that withdrawal of treatment is not equal to being left untreated. The reverse should be true, i.e. that discontinuing treatment should prompt even closer monitoring and follow up for up to 12 months when the risk of relapse is highest.21,82,83 For, as proclaimed by one of the greatest heroes in English literature: ‘Not a whit, we defy augury. . . if it be not now, yet it will come – the readiness is all’.
Future perspectives
In terms of future research, there is a clear need for more naturalistic data and pragmatic trials with non-enriched patient samples. There is also a clear need to understand the natural course of illness in untreated or treatment on as-need-basis patient cohorts, which includes more understanding of subsyndromal mood fluctuations, clear definitions and structured diagnostic tools. Most current prescribing guidelines lack any well-defined algorithms to guide clinical practice about discontinuation. Most clinical trials of BD take remission as the end point rather than the starting point to build a more in-depth understanding of this complex illness. There have been recent developments and moves towards a Multistate Outcome Analysis of Treatments in Bipolar disorder (MOAT-BD), 84 which allows for completion of survival analyses at various points of illness rather than a single end point as in Kaplan–Meier survival curves.8,85 This, along with the development of transition matrices, has been used in recent trials to estimate long-term treatment response, and prognosis can be invaluable in future research in order to further understand the course of illness and the overall therapeutic effect of treatment. 85
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AHY is funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Ethics review
This is a perspectives review article and is not subject to ethical approval considerations. This is because the study does not involve any direct or indirect participation of or access to data from patients, individuals identified as research participants including healthy volunteers, individuals identified as potential research participants because of their status as relatives or carers of patients, individuals identified as research participants but deceased, or access to data, organs, or other bodily material, or foetal material, and in vitro fertilisation