
Abstract
Background:
Antidepressant withdrawal is experienced by about half of people who try to reduce or come off their medication. It can be a debilitating, long lasting process. Many clinicians misdiagnose or minimise symptoms, inadvertently prolonging suffering. Most are unable to help patients safely taper off. There has been little research into the peer support communities that are playing an increasingly important role in helping people withdraw from psychiatric medications.
Methods:
To illustrate the growth and activities of Facebook withdrawal groups, we examined 13 such groups. All were raising awareness of, and supporting individuals tapering off, antidepressants and were followed for 13 months. A further three groups were added for the last 5 months of the study.
Results:
In June 2020, the groups had a total membership of 67,125, of which, 60,261 were in private groups. The increase in membership for the 13 groups over the study period was 28.4%. One group was examined in greater detail. Group membership was 82.5% female, as were 80% of the Administrators and Moderators, all of whom are lay volunteers. Membership was international but dominated (51.2%) by the United States (US). The most common reason for seeking out this group was failed clinician-led tapers.
Discussion:
The results are discussed in the context of research on the prevalence, duration and severity of antidepressant withdrawal. We question why so many patients seek help in peer-led Facebook groups, rather than relying on the clinicians that prescribed the medications. The withdrawal experiences of tens of thousands of people remain hidden in these groups where they receive support to taper when healthcare services should be responsible. Further research should focus on the methods of support and tapering protocols used in these groups to enable improved, more informed support by clinicians. Support from Governments and healthcare agencies is also needed, internationally, to address this issue.
Introduction
Online support forums and websites
Studies have reported on Facebook groups supporting all manner of ailments from alopecia to cancer.1–3 There are literally thousands of groups providing information and support to millions of people. A systematic review of data on the use of social media for public health topics in general concluded that qualitative benefits can be derived in terms of learning and education for both patients and physicians. 4 The authors also concluded there are both negatives and positives from this form of learning and support.
Previous studies have reported on online forums and websites assisting people withdrawing from all forms of psychiatric medications. In particular, the Surviving Antidepressants forum has been a major focus,5–7 along with some interest in benzodiazepine-withdrawal groups.7,8
Researchers have used forum posts to estimate the longevity and prevalence of withdrawal from antidepressants, 6 and instances of selective serotonin reuptake inhibitor (SSRI)-induced withdrawal anxiety and mood disorders, 5 but did not report on the actual numbers of participants on the sites. Direct, verbatim reports of severe SSRI and serotonin-norepinephrine reuptake inhibitor (SNRI) withdrawal symptoms were reported in both studies. Surviving Antidepressants has around 14,000 members and 6000 longitudinal case reports, all of which are publicly visible on the site, as are the detailed guidelines for safely tapering most psychiatric medications.
Fixsen and Ridge examined the role of online support forums in the management of benzodiazepine withdrawal. 8 They looked at the way in which patients withdrawing from this class of drug articulated their experiences and suffering during the process. They concluded that, although benzodiazepine withdrawal is unique to the sufferer, their experiences should be of great interest and value to practitioners and researchers and should be influencing support strategies in general practice. Unfortunately, there is no evidence this is happening. Fixsen herself wrote a heartfelt and emotional account of her own experience of benzodiazepine withdrawal, during which it seems she received little or no professional support. 9 Most of her support came from online communities. As an example of such online support forums, Benzo Buddies (http://benzobuddies.org) had 72,716 members on 9 June 2020.
Antidepressant withdrawal
Following the publication of a systematic review of the incidence, severity and duration of antidepressant withdrawal, 10 the subject gained traction in the global media. 11 The review concluded that 56% of those taking antidepressants suffered some form of withdrawal reaction when trying to stop the medication. A further 46% of those suffering had severe symptoms. Another study found that 61% of participants reported withdrawal symptoms and 44% of those affected reported symptoms as severe. 12 Ostrow et al. reported that 54% of their participants rated withdrawal symptoms as severe. 13 Many other studies have also reported on withdrawal symptoms experienced by patients.14–19
Antidepressant withdrawal is characterised by many and varied symptoms that appear days, weeks or months after stopping a medication.10,17,18 The symptoms are often far in excess, in terms of both quantity and intensity, of the problems for which the drugs were initially prescribed.10,20 Moreover, the symptoms are physical as well as emotional and for some they persist for months or years,21–23 sometimes even after a very slow and careful taper.13,19 Despite this evidence, many doctors and psychiatrists are reluctant to accept patients are presenting with withdrawal from the medications.19,24–26
Recent data on antidepressant prescribing rates show large year on year increases.27,28 In England, prescription rates doubled in the decade to 2018 and, in that year, 70.9 million antidepressant prescriptions were issue in the United Kingdom (UK). 29 This was a 4.3% rise on 2017 and an 8.2% rise on 2016. In Wales, Northern Ireland and Scotland, the percentage decadal increase in prescribing was 107%, 101% and 75%, respectively. 29 In the United States (US) a similar picture has emerged. Antidepressant use ‘in the past month’ increased from 7.7% of the general population in 1999–2002 to 12.7% in 2011–2014, a 65% increase. 30
When considering these prescribing statistics, it is reasonable to assume that many more patients will require help and support in the future when they eventually wish to stop taking their medications. In the UK some traction has been gained in changing clinical guidance for withdrawing patients from antidepressants, following the publication of an evidence review on dependence and withdrawal by Public Health England. 28 The previous UK guidelines can be described, at best, as vague so a National Institute of Care Excellence (NICE) modification of its antidepressant withdrawal guidelines was welcome. 29 In addition, the Royal College of Psychiatrists also publicly announced its own new stance on antidepressant withdrawal, 31 accepting that withdrawal can be difficult and long lasting for some patients. Finally, in September 2020, the College published much improved and more accurate information on the subject and course of antidepressant withdrawal, which was greatly welcomed. 32 It remains to be seen if this new advice will result in an increased awareness amongst practitioners of the issues people face when trying to stop these medications. In the meantime, online communities still appear to be a very important avenue of choice for patients seeking support when tapering off these drugs. 24 Once they realise their doctor cannot help them safely withdraw, or mis-diagnose their withdrawal symptoms as relapse or emergence of a new illness, 26 there are few alternate options for support.
Aims of this study
This study aims to begin to fill an important gap in the literature by mapping the size and role of online groups in relation to antidepressant withdrawal. We also consider the impact of these groups on the acceptance of the issue of antidepressant withdrawal by those who should be helping patients. Are these groups dealing with an issue that deserves greater attention, in terms of both research and treatment possibilities, from the psychiatric and medical professions?
Method
Ethics
The study was approved by the University of East London Research Ethics Subcommittee (Application ID: ETH1920-0260). The people whose quotes are presented in Tables were provided with Participation Information Sheets before completing Consent Forms in July 2020.
Group data collection approach
All data in this study comes from Facebook groups. There are two group types on Facebook: public groups, to which anyone can contribute, and private groups requiring people to apply to join. Applying may involve answering questions designed to filter out those without a genuine reason for joining or a simple checklist asking the person to agree to the group rules. This approach is applied to all Private Facebook withdrawal support groups. Private groups can also be secret and therefore only joined by invitation. None of the groups examined were secret, although many secret withdrawal support groups do exist on Facebook. A total of 16 groups were examined. For ease of identification the groups were numbered 1–16 (Table 1).
Summary of the Facebook withdrawal groups sampled during this study.

Admin, administrator; mod, moderator; SD, standard deviation; SNRI, serotonin-norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
Group information came from two sources. The first was using the search function on Facebook to locate groups that are supporting people withdrawing from antidepressants. The second source type is detailed in the description of the examination of Group 1 data, below. The selection criteria for this study were focussed solely on locating public and private groups providing information and withdrawal support to their members. Groups were found by searching using key words ‘antidepressants’, ‘antidepressant’, ‘withdrawal’ and ‘support’ in various combinations. Once located, groups were recorded by their Internet Uniform Resource Locator (URL). Only groups using the word ‘withdrawal’ in the group name or group description were recorded.
Data on the total number of members for groups 1–4, 6–10 and 13–16 (see Table 1) was collected on five dates: 5 May 2019, 16 October 2019, 29 January 2020, 23 March 2020 and 10 June 2020. On 29 January 2020, Groups 5, 11 and 12 were added to the survey. There are three membership observations for these three groups. The observations of group membership are actual membership numbers on each date, which considers new members and those who left the groups.
Membership growth rates were calculated from the period over which membership numbers were observed, and the growth in membership over the same period was recorded (13.1 months for groups 1–4, 6–10 and 13–16; 3.1 months for groups 5, 11 and 12). Data on the number of Administrators (Admins) and Moderators (Mods) was collected on 25 January 2020 as was the number of years the group had been in existence. Group age is displayed to the nearest whole year as shown in the group description on Facebook. There is no requirement to be a group member to observe this data.
Detailed examination of group 1 data
The second data source was via the Facebook ‘Group Insights’ function. It provides the data recorded by Facebook on group activities. It can be accessed only by group Admins. Both Edward White and Sherry Julo were Admins of Group 1 during the study period. Sherry Julo is the founding member of Group 1 and remains the owner of that group. Access to group data was facilitated through the roles of these authors.
The Group Insights function captures the following data:
membership numbers and growth;
the number of members approved or declined with time;
group post, comment and reaction data;
details of members,
Admin and Mod activities by day and time of day;
age and sex data;
member location data by country and by city.
Any data that identified members personal details have been omitted from the analysis.
Data collected from one private group (group 1) was used to examine details of group composition and activities. Group Insight data for Group 1 was gathered for the period 25 January 2019–25 January 2020.
Facebook only makes 1 year’s data available via Group Insights, but S.J. was able to supply membership growth data for group 1 from her own records from its inception in 2013.
Results
Group membership numbers and growth rates
Table 1 lists the data collected from the 16 Facebook groups that met the selection criteria. Of these, 3 were public and 13 were private. On 10 June 2020, there was a total of 67,125 members in all 16 groups. Of this total, 60,261 were in private groups. Figure 1 shows the total number of members in the sampled groups at each sample date during the study period. The percentage increase of 13 groups’ membership, sampled on five dates, was 28.4% (between the first and last sampling date). For all 16 groups together, the percentage increase in membership between the first and last sampling dates was 7.2%.

The total membership of the studied Facebook groups between 5 May 2019 and 10 June 2020. Solid circles represent the total membership of Groups 1–4, 6–10 and 13–16 (13 groups, recorded on five dates) and solid squares are the total membership of all 16 groups (recorded on three dates).
By far the largest group by membership was Group 3, Cymbalta Hurts Worse, with 24,282 members on 10 June 2020. The second largest was Group 1, Effexor (Venlafaxine) Side Effects, Withdrawal and Discontinuation Syndrome, with 6162 members. Of the remaining groups, all but two (Groups 11 and 16) had a membership of between 1000 and 5000 people.
Membership growth rates vary (Table 1), but 15 of the 16 groups grew their membership in the study period. The fastest growing private groups were Group 3 (386 new members per month in the study period), Group 11 (231), Group 10 (125), Group 13 (108) and Group 1 (85). Group 14 was the only one to lose members during the study period (–18 per month). All three public groups grew their membership. The increase in observed membership is net of recruitment of new members and loss of existing members during the period between observations.
Where group membership growth was positive (n = 15) there was a strong correlation between the number of members in the group and membership growth rate (Pearson correlation coefficient = 0.90, t = 7.59, p < 0.001; Figure 2). This suggests people are attracted to the groups where membership is higher, although it is possible that Facebook algorithms present these larger, more frequented, groups to more prospective members.

Relationship between total group membership on 10 June 2020 and membership growth rate during the study period (5 May 2019–10 June 2020) where group membership growth was positive (n = 15).
It appears the Facebook withdrawal group phenomenon is relatively new as the studied groups had a mean age of 6.1 years [standard deviation (SD) ± 1.9 years].
Medications focussed on by the sampled groups
All the groups sampled support members withdrawing from SSRI and SNRI antidepressants. Most private groups are drug specific (Table 1). Of the 13 private groups sampled, 10 catered for one medication only, namely duloxetine (3), venlafaxine (2), paroxetine (2), sertraline (2) or citalopram (1) (see Figure 3).
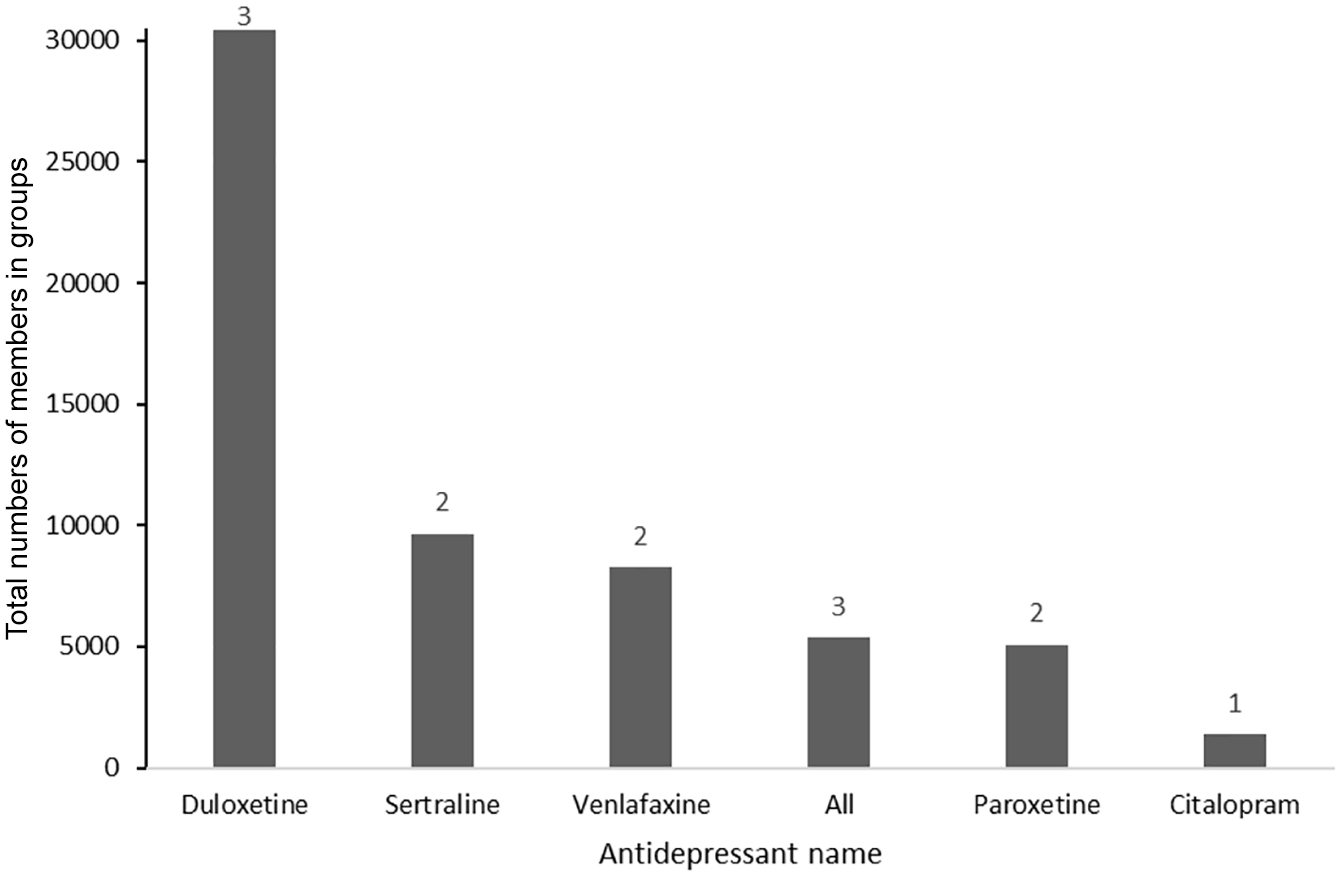
Cumulative number of private group (n = 13) members per medication. Numbers above bars are the number of groups for each medication.
The SNRI duloxetine was the medication with the most group activity (as measured by membership totals and number of groups) in the study. The five duloxetine groups had 34,852 members. Three of these groups were private with a total membership of 30,412 (Figure 3). Sertraline (SSRI) was second (9649 members in two private groups) and venlafaxine (SNRI) third (8290 in two private groups). The three groups supporting either those withdrawing from or on all medications were Groups 14, 15 and 16. Group 15 is a well-established campaign group, but many members also support each other during withdrawal.
Group administration and moderation
Most of the groups studied were initiated in the US and are administered and moderated predominantly by individuals from this region. Clear exceptions were groups 11 and 15, both administered from the UK. The number of Admins and Mods managing each group was recorded on 29 January, 2020 (Table 1). All the private groups had at least one Admin, and most had several. The Admin and Mod accounts were visible in each group description and the number and sex were noted. Some Admin or Mod accounts were generic (e.g. Facebook accounts named the same as the group or other generic names) and it was not possible to record gender. The three public groups had only one Admin, which was always a generic account.
Of the 101 Facebook accounts visible as Admins or Mods, 74 (92.5% of those identifiable by gender) were female and only 6 (7.5%) were male. The remaining 21 were generic accounts.
The ratio of group members per group admins and mods total was calculated during the study period for each private group (Table 1). For private groups where multiple Admins and Mods were observed, the highest ratio was for Group 3 at 1734 members per Admin/Mod total. Group 3 also had the highest membership total. The lowest ratio was from Group 16 at 51. Group 16 was the smallest of the groups observed.
As far as we know, all Admins and Mods of these groups were volunteers, although it is possible some may be part of organisations dealing with medication withdrawal, campaigning or charities. For example, Groups 2, 5, 9 and 10 are run by the International Coalition for Drug Awareness (https://www.drugawareness.org).
Group descriptions and mission statements
All groups except Group 6, 9 and 10 had a visible description or mission statement (Table 2). Most described the groups objectives and intentions for members, such as the approach to tapering the medication the group focuses on, which was always a very slow ‘10% of the previous months dose per month’ as a guide; warning members on the perils associated with the wrong withdrawal approach; the perceived hazards of the medications and the groups intention to provide a safe environment to enable members to privately discuss their medication withdrawal and be guided though a safe taper. Some descriptions express very negative opinions about the medications, related mainly to known side effects, withdrawal symptoms and issues with long-term use.
Group descriptions or mission statements for each group as published on Facebook, where available.

Groups 6, 9 and 10 did not publish a description or mission statement.
Some strong metaphors are used to articulate the groups’ missions and stances. The words ‘hate’, ‘toxic’, ‘risk/risks/risky’, ‘distressing’, ‘horrible’ and ‘danger/dangerous’ appear. From a positive perspective, the words ‘caring’, ‘safe/safest’, ‘confidentiality’ and ‘support’ are used.
The groups also provide information on appropriate dietary changes, supplement use and self-care advice for people tapering off the medications.
Detailed examination of Group 1: effexor (venlafaxine) tapering, discontinuation syndrome and protracted withdrawal
Group 1 membership growth data
The membership of Group 1 has grown continuously since it was first established in 2013 (Figure 4). A growth rate of 984 new members per year (85 per month in the study period) was calculated. New members applied to join the group daily. Each prospective member was screened though their answers to the questions they are required to complete as part of the application process, before being admitted to the group.

Cumulative growth of membership in Group 1, effexor (venlafaxine) side effects, withdrawal and discontinuation syndrome since group inception in November 2013.
Using the answer to the questions as a means of filtering new membership, 39% of applicants were declined in the year to 25 January 2020. Reasons for not admitting new members varied. The most common reason was them not wanting help and support to taper off venlafaxine. Other reasons are those just starting the medications, who want information about side effects or who want more focused support for their emotional distress are not admitted. If possible, suggestions for other groups to join are provided.
Group 1 membership age and sex data
Figure 5 shows the age range distribution of men and women in Group 1; 82% of group members were female. Of those, 61.6% of the total membership were aged between 25 and 54; 14.1% of men were in the same age range.
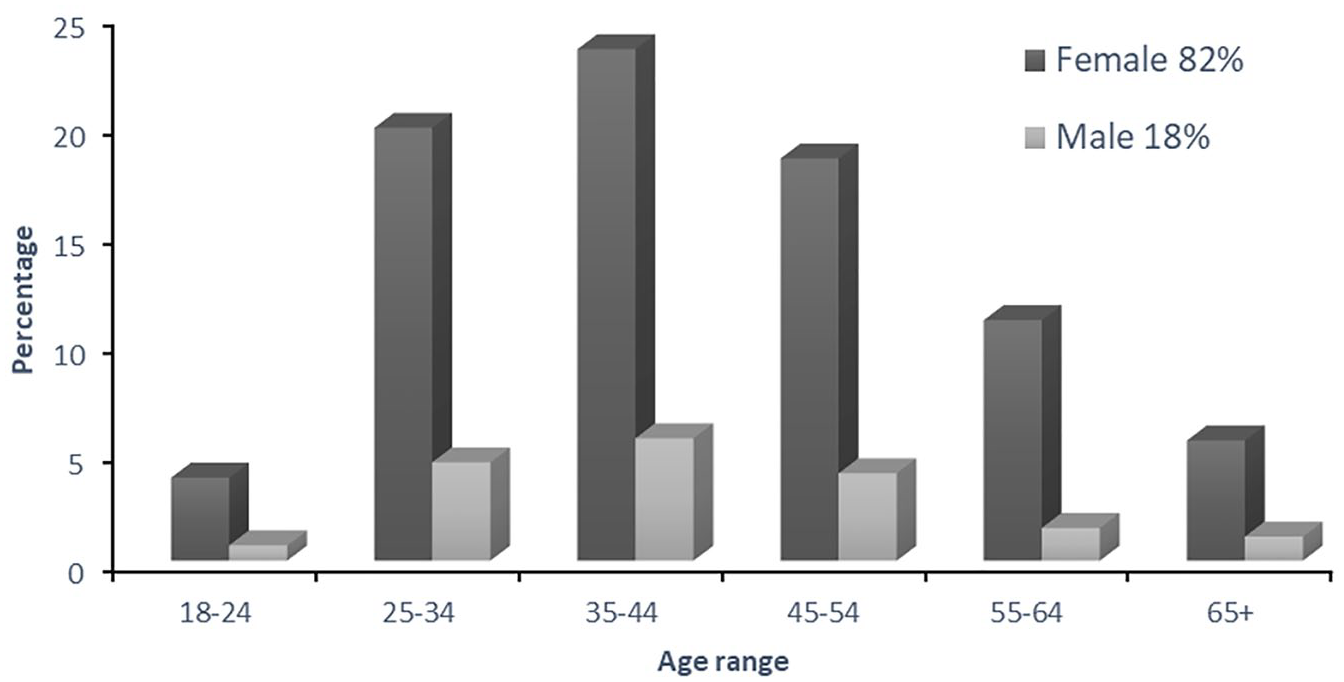
Percentage of male and female members in Group 1 by age range (years) and sex in June 2020; n = 6162.
Origin of Group 1 membership
Figure 6 shows per country membership distributions for Group 1. Facebook records membership details for the top 100 countries. Where country membership was greater than 20 (Figure 5), 94.5% of the total group membership was accounted for by five countries. The US was by the far the most common country of origin (51.2% of members on 29 January 2020). The UK had 17.3%, Canada 9.2%, Australia 6.8% and New Zealand 3.2%.

Country distribution of Group 1 members where country membership is greater than 20. Recorded on 29 January 2020.
Using country population data to the nearest million people (from https://www.worldometers.info/world-population/population-by-country/), it was possible to show a correlation between the total country population and the number of group members from each country (Pearson correlation coefficient = 0.76, n = 14, t = 7.59, p < 0.001; Figure 5). This suggests that the number of group members and therefore the prevalence of the withdrawal issue in each country is relative to population size.
Group 1 Facebook post and comments activity
Group 1 activity as measured by the number of posts and comments from the group membership during the year to 25 January 2020, was 7127 posts (daily mean and SD = 20 ± 6) and 103,670 comments (285 ± 91). The mean daily number of active members in the group generating this activity was 1428 ± 212.
Group 1 administration and moderation
Of the 10 Admins and Mods managing group 1, 7 were from the US, two from the UK and one from Australia. Previous Admins and Mods have also come from Canada and Australia. All these people have either withdrawn, or are withdrawing from, venlafaxine.
Why do people join Group 1?
Table 3 shows a sample of typical Posts made by members in Group 1 when expressing why they sought out and applied to join the group. All these posts described issues experienced when faced with clinician-led withdrawal protocols. It is clear these group members were not able to withdraw safely from the medication (venlafaxine) when following their doctor or psychiatrist instructions. Failed clinician-led tapers off venlafaxine were by far the most common reason (estimated at 80–90%) for requesting to join Group 1.
Examples of Group 1 members’ reasons for seeking support online.

Discussion
Group membership numbers, growth rates and reasons for seeking peer support
We believe this is the first study to examine the role of Facebook groups in supporting people discontinue antidepressants or indeed, any psychiatric medication. Other studies have examined certain facets of mental health support via Facebook groups,33–36 but none have looked at the role such groups play in ending a patient’s treatment with antidepressants or any other medications. In addition, there appears to be no studies that look at the growth in membership of this type of peer support group.
Although the sample of groups in this study is by no means exhaustive, it is clear this form of peer support is growing rapidly. There are also many other withdrawal support groups on Facebook that were not included in this study. It is therefore likely the total group membership recorded in this study is an underestimate of the overall number of people using Facebook groups as a source of support to withdraw from antidepressants and other psychiatric medications. What this research also shows is the far reaching and borderless support these groups provide.
By far the most common reason for people seeking out and joining these groups is following failed doctor- or psychiatrist-led tapers. Most clinicians use the standard doses of the medications to taper patients over short periods of, at most, months but often weeks or days. This approach frequently leads to significant patient suffering and distress, followed by a complete loss of belief and faith in the ability of their clinician to support them to safely taper. Hence, they seek support via these groups, where they find an array of support options, and as demonstrated by this study, often focusing on the drug they are trying to taper off. Here they can ask questions and find answers to questions directly relating to other people’s experiences and knowledge of the symptoms, and of a safe tapering process.37,38
In most groups, members are guided through a carefully managed tapering process usually starting at 10% of the previous dose per month and as directed by the group rules, advice and Admin and Mod input. These protocols are well established and documented,39–41 with extensive documentation on open forums such as https://survivingantidepressants.org and https://withdrawal.theinnercompass.org. However, despite being publicly available, they are rarely administered by clinicians, who tend to be bound by governmental and healthcare agency guidelines.
What is clear is that these groups play a significant role in supporting those who have been failed by the medical and psychiatric approaches used to taper patients off these medications. Both the overall growth of the studied groups and the apparent ability of the well-established, larger groups to attract considerable numbers of new members is remarkable and should be very worrying from a care delivery perspective. Indeed, the overall ethos and attitude of these groups towards the established medical and psychiatric approaches to supporting patients withdrawing, can be described as at best unsympathetic and at worst dismissive.
Medications focussed on by the sampled groups
The groups followed in this study concentrated on some of the more commonly prescribed SSRI and SNRI medications. No groups were found supporting those withdrawing from the older tricyclic and monoamine oxidase inhibitors (MAOI) antidepressants. However, there were groups supporting those withdrawing from novel antidepressants such as Mirtazapine (e.g. two groups with a total of 2075 members on 5 May 2020 https://www.facebook.com/groups/RemeronandMirtazapine/; https://www.facebook.com/groups/324433844869045/). The latter of these two groups is approximately 1 year old but had already gained 1121 members. There are also some groups supporting those withdrawing from second-generation antipsychotic medications such as quetiapine (e.g. two groups with a total of 1249 members on 5 May 2020 https://www.facebook.com/groups/605535796261627/; https://www.facebook.com/groups/384836649074075/) and Olanzapine (e.g. two groups with a total of 1078 members on 5 May 2020 https://www.facebook.com/groups/1514958838828543/ https://www.facebook.com/groups/1851655491831047/), but data from these groups were not fully reported in this study.
Duloxetine is a widely used SNRI medication in the US (https://clincalc.com/DrugStats/Drugs/Duloxetine) with over 16.5 million prescriptions issued in 2017, which may account for the high numbers of group members wanting to withdraw from it. That said, venlafaxine has comparable prescribing statistics (https://clincalc.com/DrugStats/Drugs/venlafaxine), but fewer group members were found. Like venlafaxine and paroxetine, duloxetine has a short half-life, which does make it harder to withdraw from.11,19,42–44 However, it is possible the group membership numbers attributable to the different medications are simply an artifact of the way the Facebook searches were executed in this study.
Group administration and moderation
The private groups supporting people tapering from antidepressants are very likely all managed by those with lived experience of tapering off these drugs. In Group 1, all the administrators and moderators have either experienced severe, long-lasting withdrawal or have been long-term users of the medication and are tapering themselves while they also support others during the same process. They have all been recruited from the group membership. Merely joining and browsing some of the other groups studied (Edward White is a member of Groups 1, 3, 11 and 15) suggests the situation is similar in most of the private groups.
Group descriptions and mission statements
The language used in the group descriptions and mission statements makes it clear these groups are rarely supportive of the use of the medications they help people to withdraw from. Although it is likely that some group members had previously found these medications helpful, as in other withdrawal ‘population’ studies,5,12 these groups do not exist to help people stay on them. Most concentrate entirely on assisting members to safely taper off.
Group 1: effexor (venlafaxine) tapering, discontinuation syndrome and protracted withdrawal
Membership is truly global but is dominated by countries that have adopted the western model of medicalised psychiatry. What is overwhelming obvious, however, is the dominance of women in both the group membership and the administrator and moderator communities. Other studies have found similar female:male ratios in patient populations, for example, 70.8% female, 44 76% female, 45 and 66.9% female. 46 One possible explanation of this female dominance may be due to prescribing rates. Taylor and colleagues reported that antidepressants were prescribed to women at 1.8 times greater rate than for men. 28 Pratt and colleagues found that women were twice as likely to have taken this class of medication than men. 30 Women also seem to be far more prone to over-medication, resulting in almost a doubling of adverse drug events compared with men and therefore may have a greater desire to taper off. 47 Off-label use of these medications for pain, fibromyalgia and menopausal symptoms may also contribute. 46
Limitations
The data is this study cannot be used to estimate the incidence or severity of antidepressant withdrawal in the general patient population. Similarly, we are unable to use these data as an estimate of the proportion of patients on antidepressants finding their way to these groups.
The numbers of administrator and moderators change in the groups as people start and leave the roles. Only one observation was made for these data, so current numbers may have changed.
It is quite possible that group members who have completed their taper successfully remain to support others on their journey and boost apparent membership numbers. It is also probable that some double counting may have occurred, in that some people may have been members of more than one group.
Why do these groups exist and what is their context in the antidepressant withdrawal issue?
Research suggests those who are fully supported during drug withdrawal, either by peers (via groups such as those followed in this study), healthcare experts or support staff have a more successful outcome.8,13,48 Yet very few funded healthcare organisations support patients withdrawing from psychiatric medications if they are unable to do so via clinician-led tapers. It is clear, however, that the longer patients take these medications, the more severe the withdrawal symptoms they may experience and the more difficult and protracted their withdrawal experience may be.20,42,44,49 Hence, far greater investment is required in terms of coaching patients and guiding them through a process that can be difficult and complicated and, for some, unpredictable and debilitating if completed too quickly. 14
Fully informed consent is crucial and currently severely lacking,50,51 as most of the people who seek support from Facebook groups are questioning the diagnosis of their healthcare provider when withdrawal symptoms emerge. A major aim of the process of reducing or stopping a patient’s medication is the minimisation or avoidance of adverse outcomes and severe withdrawal symptoms. This point raises several important questions in the context of the existence of Facebook withdrawal support groups and other forums and sites helping patients taper off and recover from the use of antidepressants. It seems these groups exist because clinicians either do not understand how to taper patients off antidepressants safely or do not have the time to guide each person as these groups can. It also appears that patients get better advice on how to taper medications in these groups than they do from clinicians. That said, those clinicians that realised patients need to taper more slowly than standard doses allow are clearly hampered by the lack of available manufactured dose sizes to do this. More importantly, clinicians do not recognise the symptoms of antidepressant withdrawal, often misdiagnosing it as relapse of previous symptoms.21,24,26 There is also evidence of huge denial of withdrawal severity and duration from clinicians.9,52 These appear to be the primary reasons patients seek help elsewhere. Their clinicians are relegated to the role of providers of the medication they need to safely taper, often without the knowledge their patient is doing so.
So how should clinicians be educated to recognise the symptoms of withdrawal when they occur and, subsequently, how to taper patients safely off these medications?26,53 There is no doubt that the required guidance from governments and health agencies to clinicians need to be revised. Next, clinicians must work with patients and allow them to taper medications at their own pace and not enforce fast tapering regimes on them. Many group members find doctors’ tapers difficult to tolerate and are seeking a more responsive approach to their desire to taper slowly off their medication. At present the guidance received from healthcare providers risks causing significant patient harm.
Apart from the Horowitz–Taylor tapering method, 20 and the work of Peter Groot and Jim van Os in the Netherlands,54–56 there seem to be no good studies on how to safely taper patients off these medications. This may be due to the lack of opportunity to conduct such research and the lack of means available to clinicians to slowly taper patients. Certainly, a lot of the existing literature on this matter does not describe ‘slow and safe tapering’. Therefore, more research is urgently needed, especially in the context of the growing peer support communities and their approach to successfully tapering members off their drugs.
Meanwhile many ‘depression’ websites, where some will look first for help, are drug company funded, espouse a bio-genetic view of the causes of depression, promote antidepressants and minimise the adverse effects, including withdrawal effects. Unsurprisingly perhaps, they offer no support for people wishing to reduce or withdraw.57,58
Conclusion
This study clearly shows that tens of thousands of people’s experiences remain hidden, on social media platforms, from clinicians, researchers and policy makers, whilst they taper off their medications under the guidance of lay experts or ‘experts by experience’. Most seek out this form of support due to failed clinician-led tapers, despite instructions for more appropriate and safe means of tapering being publicly available on the Internet. As has been previously suggested for other online communities, 33 clearly a wealth of data on patient experiences (of antidepressant tapering or discontinuation) exists within the private groups examined in this study, as do the required protocols to safely taper. The overarching question is, at what point do their experiences persuade clinicians, healthcare organisations and governments that there is an issue that needs to be fully addressed? 55 Even with the relatively small membership of these groups compared with the likely number of people in the general population who are taking antidepressants, the numbers are still significant. These people deserve more credence and support than they are getting from the clinicians they have mostly deserted, or been deserted by. In the UK, they deserve that all the recommendations made by the recent Public Health England report, 28 including withdrawal services embedded in the National Health Service (NHS), are implemented rapidly.
It is encouraging that a recent survey of UK general practitioners (GPs) (albeit with a curtailed sample size due to Covid-19) just reported that although there was ‘a marked lack of consistency in GPs’ knowledge about the incidence and duration of withdrawal effects’ two-thirds said they would welcome more training on these matters. 59
Lastly, the lay people who run these groups deserve a great deal of credit. They give support to patients who want to taper off medications that they may otherwise continue to take for an unnecessarily extended period, suffering side effects, having dosages increased, or worse still have other drugs added to treat their withdrawal symptoms. Although there will always be an important role for peer-support, these people are currently undertaking a complex, stressful, unpaid, undervalued role that should be provided by the original prescribers.