
Abstract
Background:
Drug related problems (DRPs) occur frequently among psychiatric patients due to common prescribing errors and complex treatment schedules. Clinical pharmacists (CPs) are thought to play an important role in preventing DRPs and, consequently, to increasing the quality of inpatient care. There is, however, limited information available on DRPs within the psychiatric field in Denmark. The aim of this study was to identify rates and correlates of pharmacotherapy-related problems among psychiatric inpatients in a Danish psychiatric hospital.
Methods:
A retrospective descriptive study was conducted by two CPs and data were obtained from the medical records available in two psychiatric wards. Chart-reviews were conducted for the period of June 2015 to February 2017. The analyses focussed on the prevalence of DRP categories, implementation and acceptance rates, and drugs associated with the DRPs. Extracted data were discussed with the wards’ physicians and registered in a DRP-database.
Results:
In total, 607 medical records were reviewed and, on average, 2.5 DRPs per medication review were found. There was a positive correlation between the number prescribed drugs and the average number of DRPs. The most frequent categories of DRPs were ‘drug dosage’, ‘inappropriate drug’ and ‘interactions’. The drugs represented most frequently in DRPs were olanzapine, quetiapine and pantoprazole. The overall acceptance rate was 49% with 33% of those implemented clinically.
Conclusion:
DRPs were commonly observed among psychiatric patients, particularly in those with multiple prescriptions, in relation to drugs dosage, inappropriate prescriptions and drug interactions. Particular attention must be paid to olanzapine, quetiapine and pantoprazole. Strategies to minimise DRPs among psychiatric patients are warranted and CPs can play an important role.
Introduction
Pharmaceutical care was developed initially in the early 1990s, 1 and later recognised as a process to improve the quality of pharmacotherapy. Within this process of implementing and optimizing pharmacotherapy, a need for identification and correction of problems was noted in pharmacotherapy of patients. This led to the concept of drug-related problems (DRPs), defined as problems in the pharmacotherapy of the individual patient that actually or potentially interfere with desired health outcomes. According to Pharmaceutical Care Network Europe (PCNE) classification, 2 a DRP is ‘an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes’ and DRPs are classified as dosing problems, adverse drug reactions (ADRs), drug–drug interaction, inappropriate prescription and patient adherence to the drug. In DRPs, the impact of the problem on health outcome of the pharmacotherapy must be reported. DRPs can occur within the entire course of implementing pharmacotherapy, including prescribing, dispensing, and drug usage phases. 3
Previous studies have indicated that hospitalised patients often face DRPs. In Norway, 4 2.6 DRPs were reported to occur per patient in a medical ward. In addition, occurrence of DRPs per patient has been found to increase with the number of prescribed drugs in a positive and linear fashion. 4 DRPs often cause safety issues for hospitalised patients and consequently lead to reduced quality of life, increased hospital stay, increased overall cost for health care systems and increase risk of morbidity and mortality.4–6 Therefore, improving drug therapy by preventing DRPs would be beneficial to enhance patients’ quality of life, and to reduce treatment-related costs. In addition, insurance issues must be taken into account in countries where a welfare-based healthcare system might not be available. Several tools and strategies have been developed to address DRP issues, for example, computerised alerts. Several studies have also highlighted the potential role of clinical pharmacists (CPs). The role of the CP continue to increase in diversity, and CPs are recognized as part of the multidisciplinary team within healthcare systems. Among their roles, improving medication management within the hospital setting has been noted, including medication review.7,8 CPs increase the quality of inpatient care and reduce the number of DRPs.9,10 Since DRPs can occur in any medication specialty and in any wards in the hospital, many hospitals around the globe have implemented medication review by CPs. Denmark has also implemented the performamce of medication reviews by CPs; however, little is known about DRPs in psychiatric hospitals and role of CPs. Harm and early death can be the result of prescribing errors in psychiatric patients.11,12 With common prescribing errors,11–13 such as incorrect or irrational drug choices, failure to apply clinical knowledge, 14 or complex treatment schedule due to psychiatric and somatic comorbidities,13,15 psychiatric patients are at risk of facing DRPs. Furthermore, treatment with antipsychotics increases the risk of DRPs because of the association with interactions and side effects that can be potentially fatal. 15 Studies have shown that psychiatric patients frequently experience DRPs,11,13,15–17 and it is known that the type of DRP differs markedly among different patient groups. 18 Only a few studies have looked into the prevalence and type of DRPs in the psychiatric setting.15–17,19 Two of these studies found ‘drug interaction’ as the largest category of DRPs,15,19 whereas the other studies found ‘inappropriate drug’ and ‘dosage’, along with antipsychotic polypharmacy and the need for monitoring.16,17 Therefore, this study aimed at identifying the pattern and type of DRPs in a psychiatric hospital in Denmark and the acceptance and implementation rate of DRPs, along with clarification of which classes and drugs are mainly involved in DRPs.
Methods
Design, setting and study population
This study was designed as a retrospective descriptive study using data registered in a Danish Drug Related Problems Database (DRP-database). 20 Data were anonymised in the DRP database. The database is owned by Amgros that holds an umbrella approval, which permits users’ access without a need for an extra approval. No ethical approval was therefore required for this study based on the regulations set by The National Committee on Health Research Ethics. Chart-review was conducted for the period of June 2015 to February 2017.
The study was conducted at two wards, with total of 34 beds with speciality in psychosis at the psychiatry hospital, Northern Jutland, Denmark. The wards provide mental health services for adults in the entire Northern region of Denmark. The psychiatric wards had daily ward rounds and afterwards a nurse and physicians held team meetings, where they assessed all hospitalised patients within the wards. The psychiatric wards had never had affiliated pharmacists prior to this study. In addition, the CPs had practical experience (approximately 5 years) with medication reviews in somatic patients, but no experience with psychiatric patients. The board of directors at the psychiatric hospital requested the CPs not to intervene on antipsychotic polypharmacy before counselling. This was due mainly to the fact that attending CPs at the psychiatric wards was a new initiative, and the board of directors wished to avoid resistance from physicians. The ultimate goal was to explore the potential for identification of DRPs and hence improve medicine management in psychiatric patients if required.
Two CPs attended the wards weekly and screened newly admitted patients. Based on the screening, the patients were prioritised with no exclusion for medication review, and patients with the highest number of drugs were reviewed first. The next week, the CPs followed up on the recommended interventions.
The CPs conducted a medication review on patients admitted to the wards using patient data from the electronic patient chart (EPC) including medical record, laboratory data and drug history. The CPs identified DRPs with respect to interactions, impairment of body function, duration of treatments, contraindications, adverse drug reactions, medication reconciliation and untreated indications.
In the process of determination of DRPs, drug knowledge, available clinical guidelines and consultation with nurses and physicians in assessment of the patients were utilized, which resulted in a consensus to apply. For each identified DRP, a recommended intervention was given, and it was also documented in the EPC. The DRPs were then discussed with the attending physicians who made the final decision (accept/reject). If the DRP was accepted, the physician or the CPs corrected the medication and the DPR was implemented. If the attending physician was not on the ward, the DRPs were only documented in EPC. Subsequently, the CPs assessed the acceptance or rejection of the recommended interventions and documented those in the DRP-database. The CPs also classified each DRP and registered those in the DRP-database electronically.
Data handling and analysis
For each DRP, demographic data of the patients (age, gender), number of drugs, and date for medication review were registered in the DRP-database. Each DRP was categorized in the DRP-database by registration of drug [Anatomical Therapeutic Chemical (ATC) code], 21 a text field for registration of the recommendation presented for the physician and follow-up on the DRPs (accepted and implemented, rejected, no/other action identified, no action identified, patient discharged).
The DRP-database contains the following 13 categories: dose, dosing time and interval, side effects, interaction, drug form and strength, non-adherence to guidelines, therapeutic duplication, drug allergies, length of treatment, supplement to treatment [e.g. PPI (proton-pump inhibitors) to NSAID (non-steroidal anti-inflammatory drugs)], EPC-related (related to the set-up and use of the EPC), inappropriate drug (e.g. NSAID when having ulcer) and no DRP identified. 22
Each DRP was registered with one ATC-code and, when relevant, with, for example, two interactions. Consequently, the number of drugs is higher than the numbers of DRPs.
The DRP-database also contained one unauthorised ATC-code; Z02 (= no specific drug was involved). Z02 was used to register missing clinical data such as lack of monitoring of electrocardiogram (ECG), blood pressure and laboratory data.
The data were extracted from the DRP-database to Microsoft Excel® v. 2013 and were used for further analysis. The data were analysed using descriptive statistics and presented as frequencies and percentages. Furthermore, we tested if any correlation existed between number of prescribed drugs and average number of DRPs, by application of Pearson correlation test to identify the correlation coefficient and p value; a p value below 0.05 was considered significant. For this test, SigmaPlot 14.0 was used.
Results
In total, 1385 DRPs were identified; 788 (57%) DRPs were discovered in females (mean age 48; range 18– 81 year) and 597 (43%) DRPs were discovered in males (mean age 45; range 20–79 years).
The CPs performed 607 medication reviews during the study period (June 2015 to February 2017). A total of 81 (13%) patients with no DRP identified were excluded from further analysis. The remaining patients [526 (87%)] had 1304 DRPs, which were presented for the physicians. The average number of DRPs per medication review was 2.5 (σ = 2.84).
With an increasing number of drugs prescribed, the average number of DRP increased. Figure 1 shows the correlation with a correlation coefficient of 0.811.
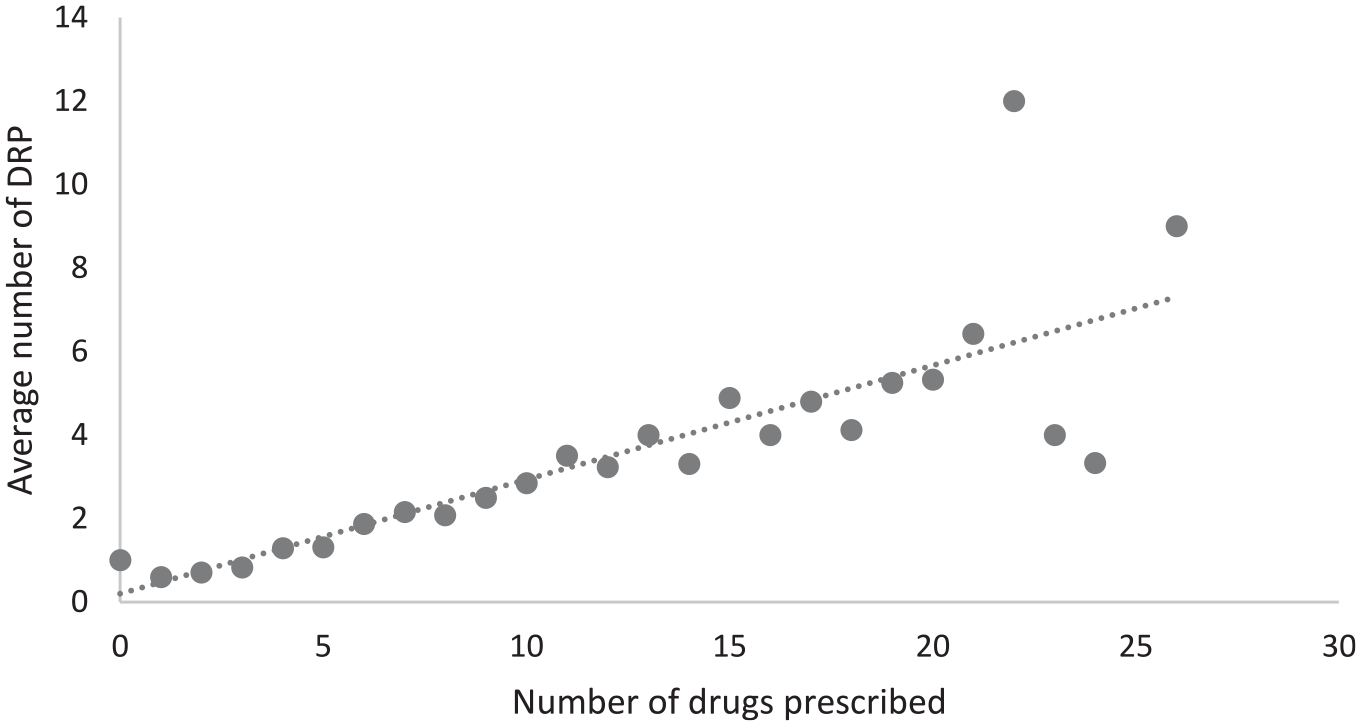
Correlation between number of drugs prescribed and the average number of DRP (Pearson correlation with coefficient of 0.811 and p value of 0.000000512).
In the study population, 418 (79%) patients had more than 5 drugs, 192 (37%) patients had more than 10 drugs, and 62 (12%) patients had more than 15 drugs. Of the 1304 DRPs, 404 (31%) DRPs were registered with two ATC-codes, which resulted in 1708 drugs. Table 1 shows an overview of the DRPs categories included in the most intervened drug in each category. The frequency of DRP categories varied, with the most frequent being ‘drug dosage’ (n = 259, 19.9%), followed by ‘inappropriate drug’ (n = 212, 16.3%), ‘interactions’ (n = 203, 15.6%), and ‘side effect’ (n = 154, 11.8%), which together comprised more than 60% of the DRPs.
Frequency of DRP categories.

DRP, drug-related problem; EPC, electronic patient chart.
It is worth mentioning that many drug–drug interactions are resulted from cytochrome P450 enzymatic reactions that can be induced or inhibited by drugs, leading to clinically significant consequences for example, unanticipated adverse reactions or therapeutic failures. CYP 2D6, 2C19 and 2C9 are the most commonly studied cytochrome P450 enzymes, and several pharmacogenetic factors have been identified where CYP enzymes are involved in treatment-associated side effects of psychotropic drugs. 23
The most frequently represented drugs in the top three of the categories were olanzapine, quetiapine and pantoprazole. Olanzapine was the top in the following five DRP types; interactions, side effects, dosing time and interval, drug form and strength, and drug allergies (Table 1).
Figure 2 summarises the overall distribution of drugs according to ATC-class. ATC N (nervous system), ATC A (alimentary tract and metabolism) and ATC C (cardiovascular system) were the most frequent ATC-classes, and contributed to 80.7% (n = 1379) of all the DRPs.

Frequency of drug groups at ATC 1st level.
Olanzapine, quetiapine and paracetamol were the drugs present most frequently in ATC N (nervous system), and pantoprazole, vitamin B-complex and cholecalciferol were the drugs most frequent in ATC A (alimentary tract and metabolism). Within ATC C (cardiovascular system), simvastatin, atorvastatin and omega-3-triglycerides were the most frequent drugs (Table 2).
Frequency of drug group at ATC level 2 with most common drug within the drug group.
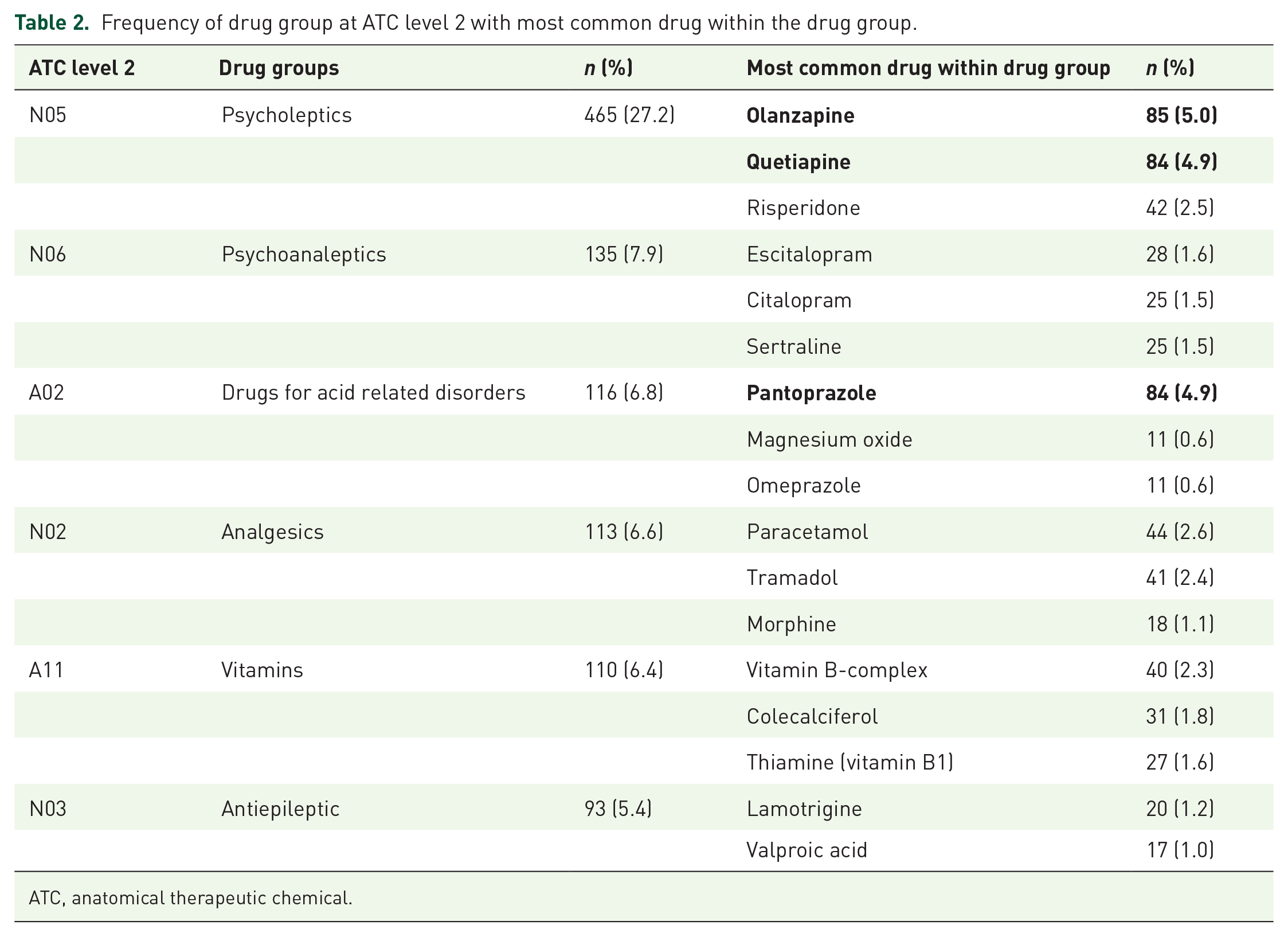
ATC, anatomical therapeutic chemical.
The three drug groups (psycholeptics, psychoanaleptics and drugs for acid related disorders) comprised 41.9% of all DRPs. Examples of these drugs are illustrated in Table 3, with categories and suggested intervention.
Examples of interventions on the three most frequent drugs reported in the DRP-database.

DRP, drug-related problem; ECG, electrocardiogram.
The overall acceptance rate of the DRPs was 641 (49%) and the implementation rate was 429 (33%). In 212 (16.3%) of the accepted DRPs, the recommended intervention was not followed, or another action was taken (Figure 3).

Acceptance and implementation of DRPs.
The group ‘not-accepted’ accounts for 23.5% of DRPs, where ‘no action identified’ comprises 22% of the DRPs. For the 288 (94%) ‘not-accepted’ DPRs it was not possible to detect any acceptance or implementation during follow up, and therefore it was categorized as ‘no action identified’. The psychiatric physician rejected only 18 (5.9%).
DRPs were categorised with no information about acceptance and implementation (n = 357, 27.4%) when patients were discharged before follow up was possible.
Discussion
In this pharmaco-utilisation study, we found an average of 2.5 DRPs per medication review and the more drugs prescribed, the more DRPs were registered. The most frequent DRP-categories were drug dosage, inappropriate drugs and interactions, despite the fact that many drugs were involved; the most frequent drugs were olanzapine, quetiapine and pantoprazole. For the drugs where a follow up was possible, an overall acceptance rate was 49% and the implementation rate was identified as 33%.
Rate of DRP occurrence and correlation with multiple factors in the psychiatric wards’ pharmacotherapy
In a systematic review, the average DRP rate varied from 0.13 to 10.6 per patient in different medical departments and the average DRP of 2.5 in the present study falls within the current reported range. 24 However, the majority of the studies included in the review found an average DRP rate lower than in the present study. The differences in average DRP can be explained by the difference in the methods of conducting medication reviews and the number of medications prescribed per patient. This study included very ill inpatients at psychiatric wards with a high average number of drugs, and this may consequently cause a higher average DRP number.15,18,25–27 It is also important to mention that different DRP categorisation methods have been used and many departments were involved 24 ; hence, a direct comparison is not possible. Furthermore, the skills and clinical experience of the CPs and the physicians involved may influence the results.19,24,28 In addition, the average DRP in this study could be higher because the CPs did not comment on antipsychotic polypharmacy.
The present study found that the numbers of prescribed drugs correlated with the increased number of DRPs. This result is in accordance with previous studies,15,18,25–27 and it is important to take this into account particularly among psychiatric patients because their pharmacotherapy is often highly complex due to both somatic and psychiatric illnesses.
The CPs were able to propose a large number of DRPs related to all available categories investigated in the present study; however, the four most frequent DRPs consisted of ‘drug dosage’ (19.9%) followed by ‘inappropriate drug’ (16.3%), ‘interactions’ (15.6%) and ‘side effects’ (11.8%). The most frequent category of recommendation was ‘drug dosage’ and similar findings were identified in other international studies.5,18,22,29–31 Several studies have shown other categories as the most frequent DRP, for example, inappropriate drugs, interactions, drug choice problem and non-adherence to guidelines.26,27,32,33 It is not clear as to what reason the adherence is poor and, to identify the potential reasons and seek solutions, further studies are required. However, it might be speculated that this factor might be a consequence of the complexity that exists within pharmacotherapy of psychiatric disorders. In addition, habits and clinical practice experience might influence prescription more than careful counselling with updated guidelines.
The differences between reported frequencies can be explained by the variation in ward settings, different focus on DRPs by the CPs, different classification system and methods. Despite different results, the dosage is often described in the literature as a DRP, which indicates that dosage has the potential to cause DRPs and requires attention by the prescribing physician.
A recent study performed by Soerensen et al. at the psychiatric department of Aalborg University hospital investigated potentially inappropriate prescribing (PIP) of psychotropic and somatic medications in inpatient units. 15 The most frequent PIPs in this study were found to be ‘interactions between drugs’ (36%) and ‘too high doses of drugs’ (16%). 15 In another psychiatric setting in Billings (MT, USA), the most common identified DRPs were ‘adverse drug reaction’ (27%), ‘unnecessary medication’ (20%), and ‘dose too high’ (13%). 34 These findings concur with the current study results.
DRPs occurrence and ATC-classes
The most common ATC-classes (ATC level 1) intervened upon in this study were ‘nervous system’ (n = 894), ‘alimentary tract and metabolism’ (n = 343) and ‘cardiovascular system’ (n = 142). This is consistent with other studies.27,31 Even though these three ATC-classes contributed in total to 80.7% of all DRPs, the DRPs consisted of several drug classes, due to the complexity of the pharmacotherapy in psychiatric patients.
A large proportion of the DRPs in this study involved somatic medicines (e.g. simvastatin, ibuprofen, pantoprazole). The physician at the involved wards indicated that they have limited knowledge of somatic medicines. Therefore, the CPs recommended interventions that were extremely relevant due to the high mortality among psychiatric patients due to physical illness.35,36
In this study, ‘psycholeptics’ (N05, ATC level 2) were the most common intervened drug group (n = 465, 27.2%); however, the severity of the DRPs was not assessed. Nevertheless, Soerensen et al. found PIPs were potentially serious for inpatients at psychiatric wards and especially the use of antipsychotics and antidepressants were associated with PIPs. 15 The most frequent intervened drugs in this study were olanzapine and quetiapine, both antipsychotics, and these drugs may pose a higher risk for causing DRPs.
Some drugs are considered as high-risk drugs, and analgesics are in this category. 37 NSAIDs (ibuprofen), opioids (tramadol, morphine) and paracetamol were represented in the present study as frequent drugs, which indicated that analgesics prescribed for psychiatric patients should be a field of attention.
DRPs occurrence, acceptance and implementation
In the present study, 49% of the recommended interventions were accepted and the physicians implemented 33%. A total of 27% percentage of the patients were discharged before follow up, and, in 22% of the recommended interventions, no action was identified. The acceptance and implementation rates may be even higher than suggested by our findings, because some of the recommended interventions were implemented but not registered in the DRP-database by the CPs before the patients were discharged. In addition, some recommended interventions were not implemented until later in the admission or after discharge by the general practitioner, and in some cases the physician accepted the recommended intervention, but it was not implemented, because the patient did not want to change the medication.
A systematic review has identified that acceptance rates for pharmacist interventions in hospitalised patients vary between 39% and 100%. 24 However, one should consider that the definition of acceptance and the study design could be different among different studies; if, for example, the discharged patients were excluded in the present study, the acceptance rate would have been 68% and the implementation rate 45%.
It has been suggested that the physician acceptance rate depends on the relationship between the prescribing physician and the CP.19,31 In one of the wards in the present study, there was a high turnover of physicians, which could influence the implementation rate because it was time consuming to obtain a good relationship between the CPs and the physician. Another explanation of variation in the implementation rate is the communication of the recommended interventions. Studies have shown that when communication was oral, the implementation rate was higher, compared with electronic communication of interventions.9,31,33 In the present study, the communication of some of the recommended interventions was only in the EPC because there were no physicians on the wards.
Study limitations
This study was the first of its kind to highlight the value and importance of systematic medication reviews for all patients by CPs as an important step towards improving patient safety in psychiatric hospitals. Our findings paved the way for awareness towards DRPs, specifically drug dosage problems, inappropriate drug prescriptions and interactions within psychiatric wards in Denmark. However, like all first-time studies we faced some limitations. We included only psychiatric inpatients in the Northern region of Denmark; hence, this may affect generalisability to other regions. Entering errors might have occurred while entering data in the DRP-database, this is due to the fact that data entry was not controlled by another person in our study. However, the DRP-database has been validated, and demonstrated to have high reliability and reproducibility. 20
Our CPs had no experience with medication reviews in psychiatric patients at the beginning of the study and additionally, the CPs were a new profession in the psychiatric departments, which required an adoption period for both the CPs and the physicians. Some studies used experienced pharmacists.19,24 Furthermore, the introduction of the CPs was not discussed with the team at the wards prior to the project, which may have had implications for the acceptance of the DRPs. In addition, we did not assess the clinical relevance and severity of the DRPs. It was the CPs who decided if the finding was a DRP and no independent arbiter was included in the decision-making process. For the future studies, it would be valuable to consider a study design where review of the retrospective information can be followed by a cohort of patients exposed to same treatment modalities (best matched with overlapping diagnoses and severity) to identify whether, and how, vulnerability factors might play a role besides pharmacological rationales in experiencing a DRP. In addition, stratification of outcome would be optimal if presented across different diagnoses, the severity of the index episode at treatment (in case of phasic or multi-polarity illness), history for therapeutic resistance, and comorbidity-associated issues. In addition, to enhance the clinical value of subsequent studies, recommendations offered as actions on identified DRPs must be formulated clearly to both raise concern and awareness, and to provide actions that can be used clinically. In this study, we have mostly raised awareness in combination with alternative ways put forward. However, recommendations can be improved with a consensus among the clinical team on a ward and CPs to identify optimal interventions for implementation.
One must also consider that, since a welfare health care system is established in Denmark, insurance issues are not problematic compared with other countries in which a welfare-based healthcare system might not be implemented. This aspect of DRPs must also be taken into account when conducting future studies of this kind.
Conclusion
Among psychiatric patients, DRPs were commonly observed, particularly in patients with multiple prescribed drugs. Our findings demonstrated that drug dosage, inappropriate drugs, and drug interactions were critical elements in the formation of DRPs. Olanzapine, quetiapine and pantoprazole were the drugs observed most frequently among the identified DRPs, which suggest higher attention should be paid to classes of psycholeptics, psychoanaleptics and drugs for acid-related disorders amongst psychiatric patients. This study provided first evidence that medication reviews conducted by CPs could help in identification of DRPs and application of corrections; hence, strategies to integrate CPs in psychiatric wards to minimise DRPs are recommended.
Footnotes
Acknowledgements
The authors would like to thank the physicians and nurses from the psychiatric wards, who were very helpful during the project. We are grateful for their assistance and cooperation. Special thanks go to Kirsten Fauerholt; Agnes Süveges and Evelina Saviceviené for competent feedback and support.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.