
Abstract
Background:
Aripiprazole lauroxil (AL), a long-acting injectable antipsychotic for the treatment of schizophrenia in adults, can be started with either 21 days of daily oral aripiprazole supplementation or a 1-day initiation regimen consisting of a single injection of a NanoCrystal® Dispersion formulation of AL (ALNCD) and a single dose of 30 mg oral aripiprazole. This phase I study assessed the pharmacokinetics and safety of deltoid versus gluteal ALNCD injections.
Methods:
Patients with schizophrenia or schizoaffective disorder (N = 47) were randomized 1:1 to receive a single intramuscular dose of ALNCD in the deltoid or gluteal muscle. Plasma samples were collected over 85 days to measure ALNCD concentration by injection site. Relative aripiprazole bioavailability for deltoid versus gluteal injection was assessed based on area under the curve (AUC∞ and AUClast) and maximum concentration (Cmax) values. Adverse events were monitored throughout the study.
Results:
Plasma aripiprazole concentrations after a single ALNCD injection were comparable between deltoid and gluteal administration. Mean maximum plasma aripiprazole concentrations were 196.1 ng/ml (deltoid) and 175.0 ng/ml (gluteal). Exposure to aripiprazole was similar, with mean AUC∞ values of 6591 day × ng/ml for deltoid and 6437 day × ng/ml for gluteal. Aripiprazole bioavailability was not significantly different between injection sites. ALNCD administration in the deltoid or gluteal muscle was well tolerated, with similar safety profiles at both sites.
Conclusion:
ALNCD demonstrated similar exposure and safety profiles between the two administration sites, suggesting that ALNCD can be given in either the gluteal or the deltoid muscles as a component of the 1-day initiation regimen for AL.
Keywords
Introduction
Aripiprazole lauroxil (AL), a long-acting injectable prodrug of aripiprazole, is indicated for the treatment of schizophrenia in adults. Because of the slow dissolution of AL, initiation of treatment requires supplementation, either with 21 days of daily oral aripiprazole or a 1-day initiation regimen utilizing a NanoCrystal® Dispersion of AL (known as ALNCD, ARISTADA INITIO®).1–3 The 21-day initiation regimen consists of 21 days of oral aripiprazole supplementation, whereas the 1-day initiation regimen consists of a single dose of ALNCD with a single dose of 30 mg oral aripiprazole administered on Day 1.1,4 ALNCD is made of the same aripiprazole prodrug as AL but contains nanometer-sized particles instead of the micrometer-sized particles associated with AL.1,5 The smaller nanometer particles have faster dissolution properties than the larger micron-sized particles, resulting in the earlier appearance of aripiprazole in the systemic circulation than with AL alone. 6
Previous research evaluating the pharmacokinetics (PK) and safety of the 1-day initiation regimen demonstrated that this regimen was a clinical alternative to the 21 days of oral aripiprazole for starting AL. 1 In this earlier study, the ALNCD injection was administered in the gluteal muscle. All approved doses of AL (441 mg, 662 mg, 882 mg, and 1064 mg) can be administered as a gluteal injection, and additionally, the AL 441 mg dose can be administered in the deltoid muscle. 4 Given that patients who start AL with the 1 day initiation regimen will receive ALNCD on the same day, but at different intramuscular (IM) injection sites, it was important to assess the deltoid muscle as an alternative site for the administration of ALNCD in patients with schizophrenia. Furthermore, previous studies on injection site preferences have found that some patients prefer deltoid over gluteal administration, reporting that they consider deltoid administration easier, less embarrassing or painful, and faster than gluteal administration; similarly, some patients who preferred gluteal injection considered it to be easier and less painful than deltoid injections. 7
We report the findings of a phase I, randomized, open-label, single-dose study comparing the safety, tolerability, and PK properties of deltoid versus gluteal administration of ALNCD for patients with schizophrenia or schizoaffective disorder.
Methods
Study design
This was a phase I, randomized, open-label study that assessed the safety, tolerability, and PK of a single dose of ALNCD in patients with schizophrenia or schizoaffective disorder. Total study duration for each patient was approximately 4 months, including up to 30 days of screening prior to the single dose of ALNCD.
The study was conducted in accordance with the Declaration of Helsinki and with Good Clinical Practice Guidelines agreed to by the International Council on Harmonization in 1997. The study protocols, amendments, and informed consent forms were approved on November 5, 2005, by the Copernicus Group’s institutional review board in Durham, NC, USA (IRB registration no. RB00001313). All patients provided written informed consent before entering the study.
Only patients who exhibited tolerability to oral aripiprazole were eligible for study enrollment. Patients who had never taken aripiprazole received two 5 mg test doses of oral aripiprazole on Day −30 and Day −29. For eligible patients who received oral aripiprazole during screening, there was a 28-day period between the last dose of oral aripiprazole and the IM injection of ALNCD on Day 1. Patients were admitted to the hospital for supervision and received a single IM dose of ALNCD, either into a deltoid or gluteal muscle. Patients remained in the inpatient unit for 8 days (Day −1 to Day 7) and were discharged on Day 8, unless additional assessments were medically indicated. After discharge, patients returned to the study center for outpatient study visits between discharge and Day 85.
Patients continued to take their prescribed oral antipsychotic regimens (excluding oral aripiprazole) throughout the duration of the study, with medication adjustments permitted for clinical reasons (excluding aripiprazole).
Participant selection
Eligible patients were adults aged 18–65 years who were clinically stable, had no hospitalizations for acute psychiatric exacerbations within 3 months before screening, a Clinical Global Impression of Severity score ⩽3, and a diagnosis of schizophrenia or schizoaffective disorder (Diagnostic and Statistical Manual of Mental Disorders, 5th edition criteria). Patients were on a stable oral antipsychotic medication regimen (excluding clozapine and aripiprazole) for at least 2 months before screening, had no change in antipsychotic medication between screening and admission, and either demonstrated tolerability to test doses of oral aripiprazole during screening or had a documented history of tolerating aripiprazole use. Pharmacogenetic testing was also conducted at screening. Cytochrome P450 (CYP) 2D6 polymorphisms were evaluated using Sanger sequencing, TaqMan chemistry, or gel-based genotyping methods. Patients were classified as extensive, intermediate, or poor metabolizers based on haplotype of the genotyped variants. Patients were classified as poor metabolizers if they possessed two nonfunctioning alleles, intermediate metabolizers if they had one nonfunctioning allele and one normal-functioning allele, or extensive metabolizers for any other combination. If the genotype for a single nucleotide polymorphism could not be determined or was missing, the metabolizer status was unknown unless it could be extrapolated from the known genotypes. Key exclusion criteria included patients who had received oral aripiprazole within 28 days, or AL or IM depot aripiprazole within 6 months, before randomization, had taken any other extended-release injectable antipsychotic within 3 months before admission or were receiving clozapine; had a moderate or severe substance use disorder (except tobacco); exhibited elevated suicidal ideation or behavior (as assessed by the Columbia-Suicide Severity Rating Scale, C-SSRS); or had used potent CYP 3A4 inducers or inhibitors or CYP2D6 inhibitors (prescription medications, over-the-counter medications, or dietary supplements) within 30 days before admission; or was a CYP2D6 poor metabolizer.
Study assessments
PK assessments
Plasma samples were collected on Day 1 (within 1 h pre-dose and 1, 4, and 8 h post-dose), Days 2, 3, 5, and 8 [within ±1 h of the Day 1 dosing time and after the electrocardiogram (ECG) assessment, although ECG assessment was not performed on Day 3 or 5], and Days 10, 12, 17, 19, 21, 23, 25, 27, 30, 33, 36, 43, 57, 71, 80, and 85 to evaluate plasma concentrations and the PK of ALNCD and its metabolites. On Days 10–21, a single plasma sample was collected within ±1 h of the Day 1 dosing time, or as close to that timeframe as possible, and for Days 23–85, a single sample was collected within ±2 h of the Day 1 dosing time, or as close to this timeframe as possible. Preparation of plasma samples for pharmacokinetic analysis was described previously. 1
Safety assessments
Adverse events (AEs) were assessed from the time that the patient signed the informed consent form through to the end of the study. Injection-site reactions were evaluated on Days 1, 2, 4, and 8 during the inpatient stay and on Days 17 and 23 during the outpatient period. Movement disorder measures, including the Abnormal Involuntary Movement Scale (AIMS), Barnes Akathisia Rating Scale (BARS) and Simpson–Angus Scale (SAS) were evaluated on Days −1 and 8 and on Days 27, 57, and 80. C-SSRS values were evaluated on Days 27, 57, and 80.
Statistical analyses
The safety population was defined as all those who received one dose of ALNCD. The PK population was defined as all those who received one dose of ALNCD and had sufficient plasma concentration data to calculate at least one of the PK parameters for at least one of the analytes. Concentrations of aripiprazole, dehydro-aripiprazole (produced during metabolism of aripiprazole by CYP3A4 and CYP2D6 enzymes), N-hydroxymethyl aripiprazole (produced by enzyme-mediated cleavage of AL by esterases) and aripiprazole lauroxil 8 were quantified in plasma samples, and PK parameters were calculated by noncompartmental methods using Phoenix WinNonlin (version 6.1; Pharsight Corp, Mountain View, CA, USA). For PK parameter estimation, values below the limit of quantification (BLQ) occurring before time to maximum observed plasma concentration (tmax) were treated as zero, and BLQ values occurring after tmax were treated as missing. The following parameters were calculated: maximum observed plasma concentration (Cmax); tmax; area under the plasma concentration–time curve (AUC) from time zero to the last observed concentration above the lower limit of quantification (AUClast); AUC from time zero to infinity (AUC∞); and terminal elimination half-life (t½). All PK analyses were conducted based on the PK population.
The relative bioavailability of aripiprazole comparing deltoid with gluteal injection sites was assessed by the evaluation of log-transformed PK parameters of exposure (Cmax, AUClast, and AUC∞). The geometric mean, geometric mean ratio (deltoid/gluteal) and 90% confidence interval (CI) were obtained from back transformation of the least squares mean and least squares mean difference in the log scale, which were based on an analysis of variance model, including ‘treatment group’ as a fixed factor.
Results
Patients
A total of 47 patients were enrolled in the study: 23 were randomized to deltoid administration (deltoid group) and 24 were randomized to gluteal administration (gluteal group). All randomized patients received one dose of ALNCD. Discontinuations were low throughout the study; overall, 95.7% of patients completed the study (91.7% in the gluteal group and 100.0% in the deltoid group). There were no discontinuations from the study as the result of an AE. Mean age was 47.2 years in the deltoid group and 50.0 years in the gluteal group; mean body mass index was 27.8 kg/m2 in the deltoid group and 29.8 kg/m2 in the gluteal group (Table 1). ‘Extensive’ and ‘intermediate’ metabolizers were represented equally in the deltoid group (47.8% each), although there were more extensive metabolizers (75.0%) than intermediate metabolizers (25.0%) in the gluteal group (Table 1).
Patient baseline characteristics (safety population).
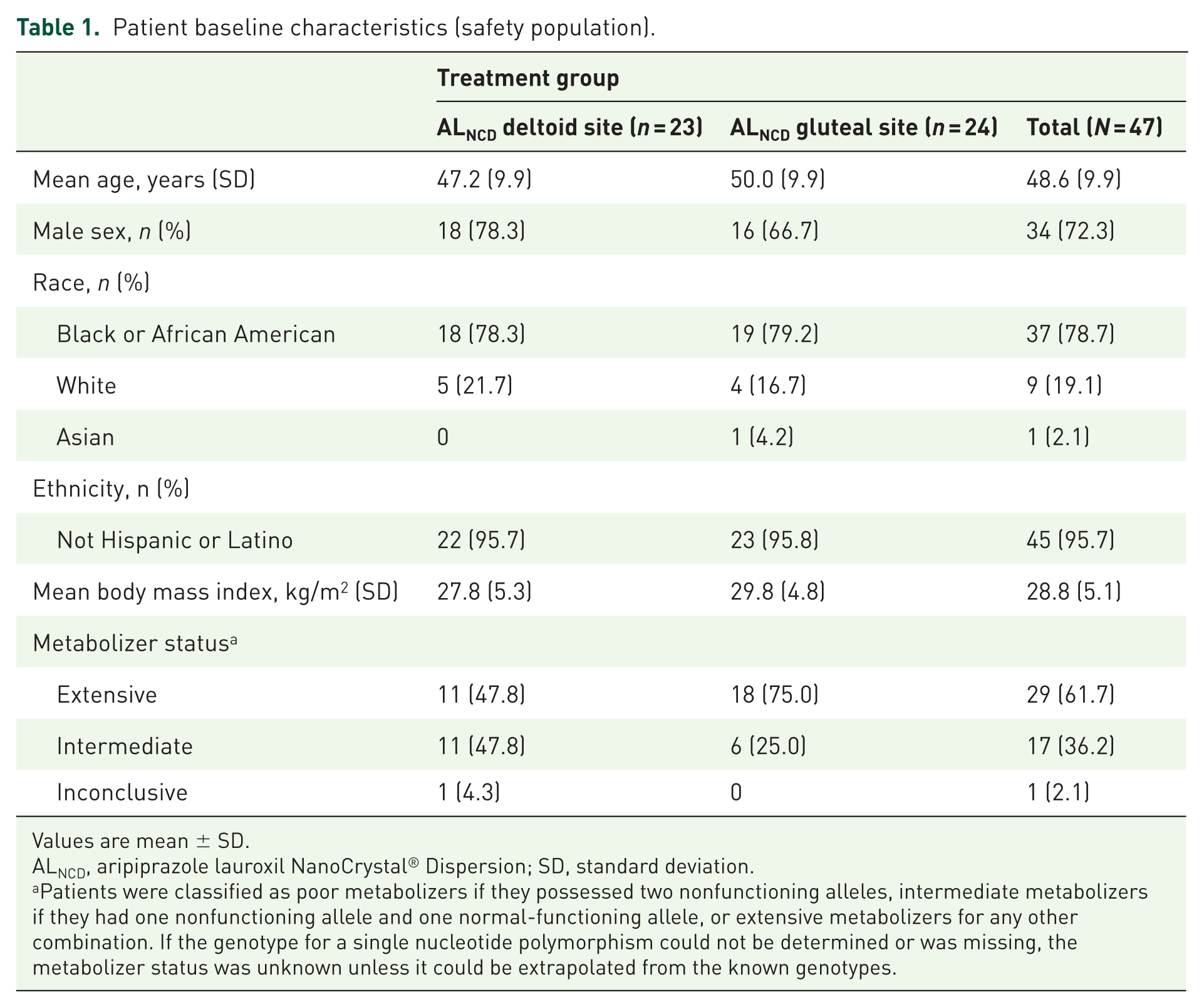
Values are mean ± SD.
ALNCD, aripiprazole lauroxil NanoCrystal® Dispersion; SD, standard deviation.
Patients were classified as poor metabolizers if they possessed two nonfunctioning alleles, intermediate metabolizers if they had one nonfunctioning allele and one normal-functioning allele, or extensive metabolizers for any other combination. If the genotype for a single nucleotide polymorphism could not be determined or was missing, the metabolizer status was unknown unless it could be extrapolated from the known genotypes.
The most frequently reported concomitant medications (>15.0% of all patients) were quetiapine, which was prescribed for 38.3% of patients, followed by risperidone/paliperidone (29.8%), lurasidone (10.6%), and olanzapine (10.6%).
PK evaluation
Aripiprazole
After administration of ALNCD, mean aripiprazole concentrations increased steadily in both groups, then declined through Day 85 (Figure 1). Mean aripiprazole concentrations were numerically higher after deltoid administration, but there were no statistically significant between-group differences.

Mean (SD) aripiprazole concentrations over time after deltoid or gluteal administration of ALNCD (PK population).
Mean Cmax values of aripiprazole after administration of ALNCD were 196.1 and 175.0 ng/ml in the deltoid and gluteal groups, respectively (Table 2). Median tmax was approximately 17.0 days in the deltoid group and 25.5 days in the gluteal group. Exposure to aripiprazole as assessed by AUC was similar between deltoid and gluteal administration, with mean AUC∞ values of 6590.8 and 6437.2 day×ng/ml, respectively. The mean t½ of aripiprazole after deltoid and gluteal ALNCD administration was comparable (14.9 days and 15.2 days, respectively).
Aripiprazole PK parameters in plasma after deltoid and gluteal administration of ALNCD (PK population).

%CV, percent coefficient of variation; ALNCD, aripiprazole lauroxil NanoCrystal® Dispersion; AUC∞, area under the concentration–time curve from time zero to infinity; AUClast, area under the concentration–time curve from time zero to the last measurable concentration–time point; Cmax, maximum observed concentration; PK, pharmacokinetic; SD, standard deviation; t½, terminal elimination half-life; tmax, time to maximum observed concentration.
Dehydro-aripiprazole
After administration of ALNCD, dehydro-aripiprazole concentrations increased slowly and steadily through approximately Day 25 and the concentration–time curve of dehydro-aripiprazole paralleled that of aripiprazole. Mean Cmax values of dehydro-aripiprazole were 65.0 and 69.8 ng/ml in the deltoid and gluteal groups, respectively. Median tmax was approximately 21 days in the deltoid group and 25 days in the gluteal group. Total dehydro-aripiprazole exposure (AUClast) was, on average, approximately 32% (deltoid) and 38% (gluteal) of that for aripiprazole exposure. Exposure to dehydro-aripiprazole, as assessed by AUC, was similar between deltoid and gluteal administration, with respective mean values of AUC∞ of 2248 and 2529 day×ng/ml. The mean t½ of dehydro-aripiprazole was similar between the treatment groups (deltoid, 17.3 days; gluteal, 16.0 days).
N-hydroxymethyl aripiprazole
After IM injection of ALNCD, mean N-hydroxymethyl aripiprazole concentrations increased through approximately Day 5. Following peak levels, concentrations declined until undetectable by, on average, Day 57. Mean Cmax values of N-hydroxymethyl aripiprazole were 25.0 and 20.8 ng/ml in the deltoid and gluteal groups, respectively. Exposure to N-hydroxymethyl aripiprazole, as assessed by AUC, was similar between deltoid and gluteal administration, with respective mean AUC∞ values of 533 and 567 day×ng/ml. Median tmax was approximately 7 days in the deltoid group and 10 days in the gluteal group. Total N-hydroxymethyl aripiprazole exposure (AUClast) was, on average, approximately 7% (deltoid) and 8% (gluteal) of that for aripiprazole exposure. The mean t½ of N-hydroxymethyl aripiprazole was similar between treatment groups (deltoid, 14.4 days; gluteal, 12.5 days).
Aripiprazole lauroxil
A total of 54 of 1114 (<5%) measurable plasma AL concentrations were detected in 23 patients (13 in the deltoid group; 10 in the gluteal group) following administration of ALNCD. As most patients with measurable plasma AL concentrations had these at only one or two time points, no PK parameters were calculated for AL.
Relative bioavailability assessment of ALNCD
The relative bioavailability of ALNCD from deltoid compared with gluteal administration was evaluated for aripiprazole. Geometric mean ratios were near unity and 90% of CIs included 1, indicating that aripiprazole bioavailability after deltoid administration was not significantly different to that following gluteal administration for Cmax (1.12; 90% CI, 0.91–1.38), AUC∞ (1.01; 90% CI, 0.85–1.20), and AUClast (1.05; 90% CI, 0.88–1.24; Table 3).
Relative bioavailability assessment of aripiprazole after deltoid and gluteal administration of ALNCD (PK population).

ALNCD, aripiprazole lauroxil NanoCrystal® Dispersion; AUC∞, area under the concentration–time curve from time zero to infinity; AUClast, area under the concentration–time curve from time zero to the last measurable concentration–time point; Cmax, maximum observed concentration; CI, confidence interval; GM, geometric mean; PK, pharmacokinetics.
Safety
AEs were reported in 15 (65.2%) patients in the deltoid group and 19 (79.2%) patients in the gluteal group. AEs were mostly mild (44.7%) or moderate (23.5%) in severity. Overall, two patients (both in the gluteal group) had severe AEs; one patient had a cyst on the back and one patient had a limb injury, neither of which was deemed related to study drug.
The most frequently reported AE was injection-site pain, with 30.4% (n = 7) for the deltoid group and 20.8% (n = 5) for the gluteal group (Table 4). AEs that were reported in ⩾2 patients in either group and reported more frequently in the deltoid group than the gluteal group, were weight gain and hypertension (both 8.7%, n = 2, in the deltoid group; both 0% in the gluteal group). There were no AE reports of akathisia in either group.
AEs occurring in at least two patients in either treatment group (safety population).

AE, adverse event; ALNCD, aripiprazole lauroxil NanoCrystal® Dispersion.
Other AEs that were reported in ⩾2 patients in either group and reported more frequently in the gluteal group than the deltoid group were headache (16.7%, n = 4, versus 0%, respectively); dyspepsia, nausea, and increased appetite (all 8.3%, n = 2 each, versus 0%, respectively); nasopharyngitis (12.5%, n = 3, versus 8.7%, n = 2, respectively); and constipation (12.5%, n = 3, versus 4.3%, n = 1, respectively). A serious AE (suicidal ideation) was reported in the deltoid group but was deemed not to be related to the study drug by the investigator. No patients discontinued the study because of an AE, and there were no deaths during the study. There were no clinically meaningful trends observed for laboratory, vital signs, or electrocardiogram results. Parkinsonism (i.e. SAS total score >3) was reported for one patient in the gluteal group. No patients had treatment-emergent akathisia or dyskinesia based on the BARS or AIMS, respectively.
Discussion
In this phase I PK and safety study, a single dose of ALNCD administered into a deltoid or gluteal muscle resulted in similar PK profiles. Mean exposure from gluteal or deltoid administration was similar, and the range of exposures overlapped between the two injection sites. The relative bioavailability of aripiprazole following deltoid administration of ALNCD was similar to gluteal administration, suggesting that both administration sites can be used interchangeably. ALNCD was well tolerated when administered at the deltoid and gluteal sites, with no new types of AEs emerging with deltoid administration during this study.
Participants who were CYP2D6 ‘poor metabolizers’, as determined by pharmacogenetic testing performed at screening, were excluded from the study as they have significantly altered clearance of aripiprazole and, as a result, require dose adjustment of aripiprazole-containing products. Extensive and intermediate metabolizers were equally represented in the deltoid group, whereas the gluteal group had more extensive metabolizers than intermediate metabolizers. However, as neither extensive nor intermediate metabolizers required a dose modification, the differences in distribution between the two groups were not considered relevant. It must be noted that, although the sample size was small, it was sufficient to assess the bioavailability of ALNCD at the gluteal and deltoid sites. However, exclusion of poor metabolizers in this study does not allow for analysis of the effect of CYP2D6 metabolizer status on total exposure of ALNCD.
Offering the choice of administration into either a deltoid or gluteal muscle has the benefit of meeting patient and clinician preferences. A European survey of healthcare professionals found that as many as 86% of respondents considered it beneficial to have the choice of a deltoid or gluteal administration site compared with not having that choice. Overall, two-thirds of respondents also agreed that medication administration via the deltoid muscle may reduce social embarrassment and demonstrate respect to the patient, more so than administration into the gluteal muscle. 9
Limitations of this study include its open-label nature, as both the investigator and the participant were aware of the injection site, thereby potentially increasing the risk of bias; as well as the lack of a placebo group in this study, the addition of which could have allowed a more robust comparison of the treatment groups at each injection site.
The comparable safety, tolerability, and PK profiles between the deltoid and gluteal muscles support the deltoid muscle as an alternative injection site for administration of ALNCD.
Conclusion
The results from the present study demonstrate that gluteal and deltoid injection sites can be used interchangeably for administration of ALNCD. Having the flexibility to administer ALNCD in either the deltoid or gluteal muscles increases treatment options for physicians and patients, who may value the opportunity to select or alternate the administration site. Enabling patients to make a choice about their treatment is likely to facilitate shared decision-making and is an element of effective medication management.
Footnotes
Acknowledgements
NanoCrystal® and ARISTADA INITIO® are registered trademarks of Alkermes Pharma Ireland Limited. Medical writing and editorial support for the preparation of this manuscript, under the guidance of the authors, was provided by Tabasum Mughal (ApotheCom, UK) and Jane A. Phillips (Peloton Advantage, NJ, USA, an OPEN Health company).
The study sponsor was involved in the study design and the collection and analysis of the data. The authors interpreted the results and made the decision to submit the manuscript for publication in Therapeutic Advances in Psychopharmacology.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Alkermes, Inc., Waltham, MA, USA. Funding for editorial support was provided by Alkermes, Inc., Waltham, MA, USA.
Conflict of interest statement
Marjie L. Hard was an employee of Alkermes at the time the study was conducted.
Angela Wehr, Lisa von Moltke, and Yangchun Du are employees of Alkermes.
Sarah Farwick has received travel and conference compensation from Alkermes.
David P. Walling has received grants from Alkermes, Janssen, Otsuka, Forum, Lundbeck, Sunovion, Acadia, Allergan, IntraCellular, Noven, Merck, AbbVie, and Roche.
John Sonnenberg has received grants to conduct clinical trials on behalf of Alkermes.