
Abstract
The prevalence of neurologic and psychiatric diseases has been increasing for decades and, given the moderate therapeutic efficacy and safety profile of existing pharmacological treatments, there is an urgent need for new therapeutic approaches. Nutrition has recently been recognized as an important factor for the prevention and treatment of neuropsychiatric disorders. The omega-3 polyunsaturated fatty acids (n-3 PUFAs) eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) play critical roles in neuronal cell function and neurotransmission as well as inflammatory and immune reactions that are involved in neuropsychiatric disease states. A large number of experimental and epidemiological studies provide a strong basis for interventional clinical trials that assessed the clinical efficacy of n-3 PUFAs in various neurological and psychiatric disorders. Most of these trials found beneficial effects of dietary supplementation with EPA and DHA, and no serious safety concerns have emerged. This review gives an introduction to recent findings on the clinical efficacy of n-3 PUFAs in various neuropsychiatric disorders and the underlying biochemical mechanisms. In addition, the reader will be enabled to identify common methodological weaknesses of clinical studies on n-3 PUFAs, and suggestions for the design of future studies are given.
Keywords
Introduction
Neurological and mental disorders continue to be on the rise. The Global Burden of Disease Report 2017 states that from 2007 to 2017, the number of neurological disability-adjusted life years (DALYs) increased by 20.5%, while mental health DALYs increased by 13.5%. 1 Countries with a high sociodemographic index (SDI) are significantly more affected than countries with a low SDI, which suggests a causal role of the Western lifestyle. 1 Diet, physical activity, and social structures are critical factors that have been linked to increases in neuropsychiatric and other disorders that are usually referred to as lifestyle diseases. Concerning diet, high intakes of fruit, vegetables, fish, and whole grains have been recommended to reduce such risk.2–4 The role of nutrition for preventing and treating neuropsychiatric disorders is increasingly being recognized, and it has recently been stated that ‘nutrition and nutraceuticals should now be considered as mainstream elements of psychiatric practice’.3–5
Research on omega-3 polyunsaturated fatty acids (n-3 PUFAs) has grown exponentially since researchers from Denmark visited Greenland in 1970 to study why the cardiovascular mortality among the Inuit population was considerably lower than in the Western countries. 6 The researchers related their findings to the diet of the Inuit, which consisted mainly of fish and meat from seals, whales, sea birds, and fur-bearing animals. These foods contain large amounts of n-3 PUFAs. 6 In the following decades, the health effects of n-3 PUFAs were studied extensively, covering almost all medical conditions, including neurological and psychiatric disorders. Such studies found that more isolated arctic populations with traditional lifestyles and diets have lower rates of depression, anxiety, and suicidality than less isolated or non-arctic populations. These findings have been associated with diet-related factors, that is, n-3 PUFA intake. 7
Research has shown that the significance of n-3 PUFAs for neuropsychiatric disorders is based on their crucial role in neuronal cell functioning. Lipid imbalance in intracellular biochemical processes and neuronal cell membranes may lead to changes in brain functioning that can cause or aggravate neuropsychiatric disorders. 8 The aim of this paper is to give an introduction to the clinical effects of n-3 PUFAs in various neuropsychiatric disorders and their underlying biochemical mechanisms. In addition, the reader will be enabled to identify common methodological weaknesses of clinical studies on n-3 PUFAs. For more in-depth reviews on the role of n-3 PUFAs in specific diseases, the reader is referred to the respective references.
What are n-3 PUFAs and how do they work?
Omega-3 fatty acids (FAs) are a type of PUFA. Polyunsaturated means that their carbon chain contains two or more double bonds. Omega (ω) is the last letter in the Greek alphabet, and omega-3 denotes that the first of these double bonds is located between the 3rd and the 4th carbon atom seen from the last (the omega-) atom of the carbon chain (Figure 1). Another nomenclature uses the Latin letter n instead of the Greek ω. Both nomenclatures are common.

The chemical structure of the two most important n-3 fatty acids, docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA).
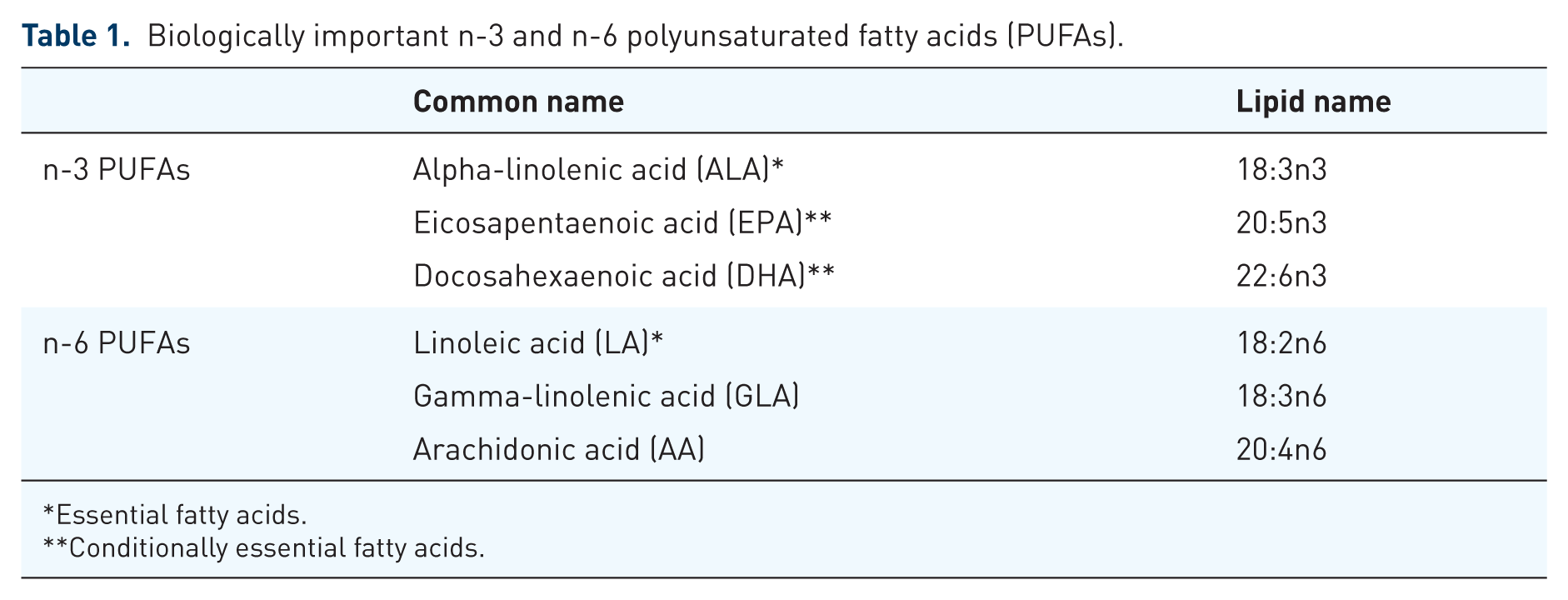
There are over 30 different PUFAs. In addition to n-3 PUFAs, there are n-5, n-6, n-7, and n-9 PUFAs. Of these, n-3 and n-6 PUFAs play the most important biological roles, and the quantitative balance between n-3 and n-6 PUFAs is believed to be a crucial factor in many disease states (discussed in the following). Table 1 gives an overview of biologically important n-3 and n-6 PUFAs.
Biologically important n-3 and n-6 polyunsaturated fatty acids (PUFAs).
Essential fatty acids.
Conditionally essential fatty acids.
There are several different n-3 PUFAs, the biologically most relevant ones being alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). Humans cannot produce ALA and therefore ALA is one of two essential FAs that must be supplied by diet [the other essential FA is linoleic acid (LA), which is an n-6 PUFA]. ALA is found in seeds, nuts, and plant oils. While no major biological effects of ALA on cells or tissues have been identified so far, its biological value lies mainly in being a substrate for the synthesis of other PUFAs. 9 The human body is not able to synthesize DHA and EPA de novo, but can produce them from ALA. However, this capacity is very limited and, in addition, subject to polymorphisms of the genes coding for the involved enzymes (fatty acid desaturase and elongase). 10 Reported conversion rates of ALA to EPA are 0.2–6%, and 0.05% or less for DHA. Women seem to possess a higher conversion capacity than men. 9
Since humans can convert only an insufficient proportion of ALA to EPA and DHA, the latter two are classified as conditionally essential FAs. 9 Dietary sources of EPA and DHA are fish, shellfish, and meat from marine mammals, for example, seals and whales. Like humans, these animals do not produce n-3 PUFAs themselves to a relevant degree. Instead, EPA and DHA are synthesized by marine algae, which are eaten by small fish that in turn are food for larger animals.
The phospholipids of the brain’s gray matter and the retina contain high concentrations of DHA and arachidonic acid (AA, which is an n-6 PUFA), which supports the notion that long-chain PUFAs play an essential role in the development and maintenance of proper central nervous system (CNS) function.11–14 Owing to the many double bonds, PUFAs are more bulky than saturated fatty acids (SFAs; Figure 1). When PUFAs instead of SFAs are incorporated into the phospholipid layer of the cell membrane, the physicochemical properties of the membrane become altered; it becomes less rigid and more fluid. More specifically, phase behavior (how a membrane’s mobility changes with temperature) is shifted to the left, that is, more fluid, while elastic compressibility (relative volume change/thickness in response to stress), permeability (passive diffusion of molecules through the membrane), fusion (two membranes merge into one), flip-flop (transverse diffusion of membrane constituents, that is, from the outer layer to the inner layer or vice versa), and protein activity become increased. 15 Incorporation of n-3 PUFAs into cell membranes also leads to reorganization of lipid raft formation. Lipid rafts are membrane domains that contain clusters of receptors and proteins involved in signal transduction. Hence, all these mechanisms affect the function of membrane proteins, such as receptors, membrane-bound enzymes, G-proteins, and ion channels, thereby modulating intracellular and intercellular signaling pathways in neurons and other cell types.16,17 Of special interest for the etiology, prophylaxis, and treatment of neuropsychiatric disorders is the involvement of n-3 PUFAs in the fetal development and later maintenance of dopaminergic pathways in the brain. 18
Another way in which n-3 PUFAs may positively affect CNS functions such as cognition and behavior is by affecting the gut’s microbiota composition, its fatty acid composition, and by reducing intestinal inflammation, which in summary affects the gut–brain axis. This has been demonstrated in both animal and human studies.19–21
n-3 PUFAs are, apart from being building blocks in cell membranes, biotransformed to eicosanoids such as prostaglandins, thromboxanes, and leukotrienes, as well as endocannabinoids and other lipid-based signaling substances that are involved in many biochemical processes in the body, for example, inflammation and immune responses. Eicosanoids derived from n-3 PUFAs, such as prostacyclin I3 and thromboxane A3, are generally considered anti- inflammatory, antithrombotic, vasodilatory, and antineoplastic. The anti-inflammatory effects of n-3 PUFAS most probably contribute to their neuroprotective effects in various neuropsychiatric conditions (see the following). By contrast, signal substances derived from n-6 PUFAs such as AA or LA, for example, prostaglandin E2 or thromboxane A2, have mainly opposite effects. Therefore, the balance between n-6- and n-3 PUFAs has been identified as a critical biomarker for chronic disease. 22 The WHO has stated that there should be an optimal balance in the dietary intake constituted by n-6 and n-3 PUFAs. 23 However, n-6 PUFAs are found in large amounts in most plant oils, and the consumption of plant oils has exploded in the past decades while fish consumption has steadily declined. 22 Consequently, the Western diet is characterized by an over-supply of n-6 PUFAs, a deficiency in n-3 PUFAs, and, thus, a striking imbalance between these two. 22
All PUFAs are highly susceptible to oxidation. Accordingly, oxidative stress in the body has a large impact on lipid metabolism including PUFAs. Lipid peroxidation leads to membrane phospholipid degradation, directly affecting cell membrane function. 24 Similarly, nutritional supplements that contain PUFAs must be protected by effective antioxidants. Fish and other sources of marine n-3 PUFAs contain polyphenols and other compounds that protect n-3 PUFAs from oxidation in vivo. However, these compounds are removed during the production of commercial n-3 preparations, mainly because they also account for the typical fishy taste and odor. Therefore, most manufacturers add vitamin E as a fat-soluble antioxidant. Despite this, studies from different countries have consistently shown that most n-3 PUFA preparations that are sold over the counter are oxidized (rancid) to varying degrees.25–27 Obviously, decomposed n-3 PUFAs have lost their characteristic biological properties. Even worse, peroxidation products of PUFAs may under certain conditions promote oxidative stress, a pro-inflammatory environment, DNA damage, and clinical deterioration.28,29 Since most interventional clinical studies use ordinary fish oil capsules, this may be a major reason why some interventional studies did not find a beneficial effect of n-3 PUFAs or even an increase in clinical symptoms. 30
Many authorities and professional societies recommend certain amounts of daily intake of n-3 PUFAs, but they do not provide corresponding reference ranges for n-3 PUFA blood levels. 31 Nonetheless, free serum n-3 PUFAs, erythrocyte membrane n-3 PUFAs, and whole blood phospholipid n-3 PUFAs can be measured by many laboratories and used as biomarkers to estimate the risk for disease and to monitor the efficacy of n-3 PUFA substitution with a given commercial preparation. The two best documented biomarkers are (1) the n-3 index, which is the combined percentages of EPA plus DHA measured in erythrocyte membrane FAs, and (2) the n-6/n-3 ratio, which is the ratio of n-6 FA and n-3 FA percentages. 32 A high n-6/n-3 ratio and a low n-3 index are generally associated with poorer medical condition. In Western populations, the average n-3 index varies from 2.9% to 7.7% while a value of 8–11% is required for optimal protection against cardiovascular diseases.33–36 The average n-6/n-3 ratio in Western countries is 15–21 while a value below 5 is generally recommended. 28 The predictive value of the n-6/n-3 ratio has recently been questioned and the n-3 index has been suggested as a more robust biomarker. It should be noted, however, that the author of that paper may be biased, as he has commercial interests related to n-3 index testing.32,37
The reason why the PUFA status should be measured in red blood cells and not in plasma is that the plasma fatty acid profile may change within hours, depending on the type of food and time after intake, while red blood cells have a half-life of 120 days, which provides a much more stable measure of the PUFA content of cell membranes. Moreover, the PUFA content of red blood cell membranes is highly correlated to the PUFA content of major organs.38–40
Effects of n-3 PUFAs in various neuropsychiatric disorders
The effects of n-3 PUFAs have been studied in a large variety of neurological and psychiatric disorders. In the following, a selection of them are discussed. Additional neuropsychiatric disorders that are not discussed in detail are summarized at the end of this section.
Depression
Numerous epidemiological and interventional studies have accumulated strong evidence for a connection between n-3 PUFA status and depression.41,42 Low fish consumption and a low omega-3 index are clearly correlated with a higher risk of developing a major depression.43–48 Accordingly, an increase in the omega-3 index reduced the risk and the severity of depressive symptoms in several clinical studies. One of them found that for each 1% increase in the n-3 index, the risk of developing depression was reduced by 28%.45,49,50 This correlates with findings from clinical studies in nonpsychiatric conditions. 33 Depressed patients also exhibit higher n-6/n-3 ratios than nondepressed controls.50–52
Various studies found an inverse correlation between dietary intake of n-3 PUFAs and the severity of depressive symptoms including suicidality.28,48,52–58 Although some of these studies produced neutral results, several meta-analyses confirmed the antidepressant effects of dietary EPA and DHA.59–63 Daily doses between 1 and 3.5 g have produced therapeutic effects. 42 It is unclear whether EPA and DHA differ in their antidepressant efficacy, as each of them independently has been proposed as the strongest mediator of the beneficial effects of n-3 PUFAs in depression.29,46,60,64,65 Interestingly, the DHA amount in blood phospholipids, but not the EPA amount, distinguished responders from nonresponders in a recent interventional study. 66
The efficacy of n-3 PUFAs in special subpopulations such as children, adolescents, elderly patients with underlying comorbidities, or in related conditions such as bipolar disorder, is only incompletely studied. Most data available so far suggest beneficial effects of supplementation with n-3 PUFAs in these patient groups.29,67–72
How n-3 PUFAs exert their antidepressant action is not fully understood. At present, it appears that multiple unspecific mechanisms of action are responsible. Modulation of G-protein signaling via G-protein coupled receptors and effects on lipid raft formation has been suggested as one possible mechanism. 73 Other mechanisms such as modulation of pro-inflammatory mediators, and changes in telomerase levels may also play a role.48,57,65,74
Schizophrenia
Schizophrenic patients show a marked depletion of essential FAs, particularly AA and DHA, in red blood cell membranes. These two FAs are the most abundant FAs in the human brain, which suggests that they play a crucial role in the function of the CNS.11–13 Accumulating evidence from experimental and clinical studies has led to the ‘membrane hypothesis’, which postulates dietary-related changes in PUFA-dependent membrane function as a major pathophysiologic mechanism in schizophrenia.75,76 Accordingly, diet changes that lead to increased membrane levels of n3-PUFAs can have significant effects on schizophrenic symptoms. 77
Several randomized, placebo-controlled clinical trials have studied the efficacy of n-3 PUFA supplementation in schizophrenia. While some yielded positive results,78–80 others found partial efficacy such as reduced need for antipsychotic medication,81,82 or no beneficial effects at all.30,83 However, the observation time in most studies was only 8–12 weeks and as mentioned earlier in this article, sustained changes in membrane function may take longer time to develop. The only long-term study so far, a 6-month, randomized, placebo-controlled trial in first-episode schizophrenic patients, found a significantly greater decrease in the intensity of symptoms and an improved level of functioning in the n-3 group than in the placebo group. 84
Disturbances in cortical membrane FA homeostasis have been identified as a pathological aspect of schizophrenia, which is one of several possible explanations for the efficacy of n-3 PUFAs.75,76,85 Beyond membrane-related effects on neuronal cell signaling pathways, n-3 PUFAs may act through additional mechanisms, for example, modulation of dopaminergic pathways in the mesolimbic system. 18 In an in vitro model mimicking the involvement of viral infection in the development of neuropsychiatric disorders, n-3 PUFAs showed significant neuroprotective effects. 86 In addition, clinical studies in schizophrenic patients found that n-3 PUFA substitution leads to an increase in telomerase levels as well as a reduction in oxidative stress.84,87,88
ADHD
It is well established that dietary depletion of n-3 PUFAs during fetal development and early childhood may have adverse effects on brain development, neurodevelopmental outcomes, and cognitive health.54,89,90 For example, low maternal intake of n-3 fatty acids during pregnancy is correlated with lower verbal intelligence, attention deficit hyperactivity disorder (ADHD), dyslexia, dyspraxia, autism, and impaired social behavior in the child.89,91–93
Epidemiological studies found that children with ADHD have lower blood levels of n-3 PUFAs than controls.93–96 Accordingly, several randomized, placebo-controlled interventional trials reported positive effects of dietary supplementation with n-3 PUFAs in ADHD.94,95,97–99 However, other trials found only small or no therapeutic effects. Hence, some meta-analyses stated that there is evidence for n-3 PUFAs as a supplement to established therapies while others concluded that the currently available evidence is inconclusive.94,100–107 Major reasons for these contradictory conclusions are different selection of studies, small sample sizes, variability of inclusion criteria, variability of the type and dosage of supplementation, short follow-up times, and different cognitive and behavioral outcome parameters.101,102,105 Moreover, some studies that used multiple outcome parameters observed therapeutic effects in some but not all of them.
While the pathophysiology of ADHD is not fully understood, it is generally accepted that brain dopaminergic and noradrenergic systems play a central role. This hypothesis is supported by the clinical effectiveness of medicines such as methylphenidate and amphetamine. In animal experiments, n-3 PUFA depletion induced symptoms that mimic ADHD in humans, while symptom severity was inversely correlated with dietary n-3 PUFA intake. The significance of n-3 PUFAs for the regulation of dopaminergic pathways in ADHD has recently been reviewed. 18
PTSD
It has long been known that both physical and psychological stress are associated with altered blood levels of free fatty acids including long-chain PUFAs.108,109 Cross-sectional studies reported lower n-3 PUFA blood levels in patients with PTSD than in healthy controls.110,111 Similarly, longitudinal studies found an inverse relation between blood levels of n-3 PUFAs and the risk of developing PTSD after accidental injury.112,113
However, only a few clinical trials examined possible effects of supplementation with n-3 PUFAs on post-traumatic stress disorder (PTSD), and they produced mixed results. While one study found that EPA but not DHA reduces the risk of developing PTSD in patients with accidental injury, 114 another study found ameliorated psychophysiological stress responses after combined supplementation with a high dose of DHA + a low dose of EPA. 115 A study in survivors of the great earthquake in Japan 2011 found an effect of 1568 mg DHA + 157 mg EPA in women, but not in men. 116 Further clinical research is clearly needed.
Different mechanisms could mediate possible effects of n-3 PUFAs in PTSD and other stress-related conditions. Since PTSD is associated with increased interleukin 6, interleukin 1β, tumor necrosis factor alpha (TNFα), and interferon γ levels, it has been suggested that the expression of these cytokines may be normalized by the anti-inflammatory and neuroprotective actions of n-3 PUFAs. 117 This hypothesis is supported by experimental findings. 118 Another, more specific mechanism may be an increase in brain-derived neurotrophic factor (BDNF) induced by n-3 PUFAs, which leads to induction of hippocampal neurogenesis by which fear-related memory might be cleared.119–121 A more recent hypothesis assumes a role of the n-3 PUFA-derived endocannabinoids 2-docosahexaenoylglycerol (2-DHG) and docosahexaenoylethanolamine (DHA-EA) in reducing psychological distress. 122
Dementia
The clinical efficacy of established medications for Alzheimer’s disease (AD) and other dementias is weak, and new treatment options are urgently warranted. A large body of evidence suggests a positive correlation between n-3 PUFAs and cognition, and most (but not all) interventional studies reported beneficial effects of n-3 PUFAs on cognitive outcome and quality of life in patients with AD, especially with early stage AD and mild cognitive impariment.20,123–128 While some interventional studies reported neutral results, a recent meta-analysis by Zhang et al. found that n-3 PUFAs from fishery products are associated with a lower risk of cognitive decline in AD patients. 129 This is supported by a study in healthy subjects where both the n-3 index and the n-6/n-3 ratio were correlated with cognitive function as well as hippocampal and total brain volume.130,131
Experimental evidence implies biological plausibility for beneficial effects of n-3 PUFAs in dementia. Antioxidant actions, enhanced brain plasticity, and other mechanisms that are more directly related to the specific pathology displayed in dementia, such as anti-inflammatory, anti- amyloid and anti-tau effects, have been demonstrated.132–134 DHA may have stronger neuroprotective properties than EPA as DHA-deficiency is highly correlated with cortical and hippocampal atrophy.135,136 Experimental data also show that DHA regulates apoptotic processes and the level of Aβ-induced lipid peroxides, which has positive effects on the survival of neurons. 137 In addition, DHA increases dendrite density and reduces beta amyloid and tau protein load.138–141
In addition to these mechanisms, n-3 PUFAs may ameliorate cognitive dysfunction via indirect effects. Both AD and vascular dementia are associated with cardiovascular events such as microinfarctions in the brain, and it has been shown that prevention of cardiovascular morbidity with n-3 PUFAs has beneficial effects on cognitive function.142,143
Factors that might explain the mixed results of clinical studies on n-3 PUFAs in dementia are the large variations in study design (e.g. RCTs versus epidemiological studies), study populations, observation times and follow-up periods, variations in n-3 dosages, different biomarkers for fatty acid status, different cognitive outcome parameters as well as different (and partly low) sensitivity in the neuropsychological tests. Notably, it has been suggested that n-3 PUFAs may exert their most significant effects on cognition before disease onset. This is of special importance in AD which is a disease that probably starts decades before clinical symptoms become overt.131,144
Parkinson’s disease
After AD, Parkinson’s disease (PD) is the second most common neurodegenerative disorder with a prevalence of about 2% in people over 65 years. 145 While the etiology of PD is still not fully understood, its pathophysiology is well studied and involves dysfunction of the mitochondria and inflammatory and oxidative stress reactions.146–148 Despite this knowledge, the standard pharmacological approach to treat PD is still more or less limited to enhancing dopaminergic signaling. However, dopaminergic medications may lose effect over time and can induce serious side effects.149,150
Only few clinical studies examined n-3 PUFAs in PD. All but one reported beneficial effect. Observational studies found a correlation between higher intake of n-3 PUFAs from fish and lower prevalence of PD.151,152 In the Rotterdam Study, a prospective population-based cohort study of 5289 subjects, each SD increase of energy-adjusted intake of PUFAs reduced the risk of developing PD by 34 %. 153 A randomized, double-blind placebo-controlled trial found that supplementation with n-3 PUFAs improved clinical symptomatology in PD patients, as indicated by a decrease in the average Unified Parkinson’s Disease Rating Scale score. 154 A case–control study, however, found that dietary intake of n-3 PUFAs was not predictive for the risk of developing PD. 155
Part of the positive effects of n-3 PUFAs on PD is probably due to their neuroprotective properties, since oxidative stress and neuroinflammation are ameliorated by n-3 PUFAs. 156 Indeed, a clinical study found that supplementation with n-3 PUFAs decreased C-reactive protein and increased glutathione concentrations as well as total antioxidant capacity. 154 These results are supported by experimental findings demonstrating a reduction of inducible nitric oxide synthase activity in the CNS and increased levels of BDNF after supplementation with n-3 PUFAs.120,157,158 Apart from neuroprotective effects, n-3 PUFAs may enhance dopaminergic signal transduction through different mechanisms. 18
Other neurological and psychiatric disorders
In addition to the conditions discussed above, the effects of supplementation with n-3 PUFAs have been clinically studied in other neuropsychiatric disorders, such as epilepsy,159–162 multiple sclerosis,163–167 bipolar disorder,168–170 anorexia nervosa,171–173 borderline personality disorder,174–176 and autism spectrum disorders.177–181 Apart from these systematic clinical trials, numerous case reports have been published for these and even more neuropsychiatric conditions including rare metabolic diseases such as Zellweger syndrome. 39 The majority of these interventions reported beneficial effects of supplementation with n-3 PUFAs. These findings are supported by numerous epidemiological studies that found strong evidence for an inverse relation between dietary n-3 PUFA intake/blood n-3 status and the prevalence and severity of the conditions mentioned above.182–189
Safety of n-3 PUFAs
Most of the clinical studies cited in this paper did either not report any clinically significant adverse effects or no difference versus placebo. Few studies reported mild to moderate adverse reactions, mainly nausea or loose stools, especially with high doses.
A much-debated study in men with prostate cancer, the SELECT trial, reported that higher plasma omega-3 fatty acid levels were associated with increased risk for developing prostate cancer. 190 However, several comments on that study pointed out that this conclusion was inappropriate and not supported by study data. Moreover, other studies found opposite effects of n-3 PUFAs on prostate cancer.191–193
Although it has been postulated that n-3 PUFAs may increase LDL cholesterol, affect glucose metabolism and prolong bleeding time, recent studies as well as reviews and meta-analyses do not support this.194–196 Given the widespread use of n-3 supplements and the experience from a large number of clinical studies, it must be concluded that these potential effects may gain clinical significance only in rare cases. Accordingly, the United States FDA has ruled that the daily intake of up to 3 g of n-3 PUFAs is generally recognized as safe (GRAS). 197 This ruling took into consideration the postulated effects on glucose metabolism, bleeding, and low-density lipoprotein (LDL) cholesterol. Similarly, the European Union’s EFSA Panel on Dietetic Products Nutrition and Allergies concluded that supplemental intake of EPA and DHA at combined doses up to 5 g per day, and supplemental intakes of EPA alone up to 1.8 g per day, do not raise safety concerns for adults. 198
Recommendations for future research
Most clinical trials that assessed the effect of dietary supplementation with n-3 PUFAs in neuropsychiatric conditions yielded positive results. However, a considerable number of studies produced neutral or even negative results. The conflicting findings may be attributed to several reasons.
Almost all interventional studies used fish oil capsules. That may have seriously distorted the results from these studies since most commercial n-3 preparations are oxidized (rancid) to varying degrees.25–27 Future studies using such capsules should therefore report the degree of oxidation in the preparations used, for example, by stating the peroxide value (PV), the anisidine value (AV), or the total oxidation value (TOTOX).
Omega-3 preparations are manufactured from different natural sources, containing different amounts of n-3 PUFAs, different DHA:EPA-ratios and different chemical composition of these FAs (mostly as ethyl esters, but also as triglycerides, diglycerides, monoglycerides, phospholipids, or free carboxylic acids) as well as different types and amounts of antioxidants (e.g. various types of tocopherols, astaxanthin, etc.). These different formulations naturally lead to differences in bioavailability, susceptibility for oxidation, and biological activity.199–203 Being classified as food or food supplements, commercial n-3 products are not subject to bioequivalence requirements or other stringent forms of pharmaceutical/pharmacological standardization the way licensed medical drugs are. Disregarding the fact that all these n-3 preparations are not pharmaceutically and biologically equivalent represents a major weakness of clinical trials and, particularly, meta-analyses of these trials.
Most clinical studies used fixed doses and did not measure blood levels of n-3 PUFAs. Owing to the uncertainties inferred by varying degrees of oxidation and varying bioavailability (see above), future clinical studies should rather use individual dosing guided by the n-3 index and the n-6/n-3 ratio. Target ranges for these biomarkers should be defined before study start. A striking example for a failed clinical study and the necessity of defining target ranges is the recently published VITAL study. 204 After 1 year of treatment, the average n-3 index had risen from 2.1% to 4.1% and the researchers did not find a cardioprotective effect of n-3 PUFAs. It is well documented that this index must be at least 8% to obtain a cardioprotective effect, while an index below 4% is classified as ‘high risk’ for cardiovascular disease. 33 Consequently, the study merely confirmed the previous knowledge that an n-3 index below 8% does not provide cardioprotection.
While an effect of n-3 PUFA substitution on the synthesis of lipid-based signaling substances and other cytokines usually can be seen after a few days (due to the short biological half-life of these compounds), their incorporation into cell membranes and the onset of related biological effects may take longer time, depending on the turnover rate of these cells, the phospholipid-layer of their cell membrane and of the incorporated proteins. Thus, the length of the observation period is crucial, and 8 weeks may not be enough in all cases. For the same reason, n-3 PUFAs appear less suitable as acute treatment of neuropsychiatric disorders, but more useful for long-term prevention.
Conclusion
A connection between nutritional factors and neuropsychiatric disorders should be regarded as established. Numerous epidemiological studies have shown a strong correlation between low n-3 PUFA status and higher prevalence and severity of different neuropsychiatric disorders. Accordingly, many interventional studies that assessed the efficacy of n-3 PUFA supplementation in different neuropsychiatric disorders have found positive effects. A large body of experimental data provides a solid biological and pharmacological basis for these findings. At present, n-3 PUFAs appear to be more useful in long-term preventive approaches rather than treatment of acute episodes. However, not all clinical studies found beneficial effects. Possible reasons for conflicting findings have been discussed in this review, and future clinical studies as well as meta-analyses of such studies should address them. Measurement of n-3 PUFAs in blood for diagnostic purposes, risk assessment, and therapeutic drug monitoring is cheap and already available at many laboratories. The use of n-3 PUFAs as a therapeutic option in the treatment of neurological and psychiatric disorders may be still in its infancy, but their therapeutic potential, favorable safety profile, ease of administration, and low treatment costs are promising. The increasing number of clinical studies and other research papers suggests that supplementation with n-3 PUFAs may play a greater role in the future treatment of neuropsychiatric disorders.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
AR has received speaker’s honoraria and consultant fees from GlaxoSmithKline, UCB, and Zinzino. HL has nothing to declare.
Ethical Statement
Our study did not require an ethical board approval because it did not contain human or animal trials.