
Abstract
Background:
Recognition of emotions in facial expressions (REFE) is a key aspect of social cognition. Anxiety and mood disorders are associated with deficits in REFE, and anxiolytics and antidepressants reverse these deficits. Recent studies have shown that serotonergic hallucinogens (i.e. ayahuasca, dimethyltryptamine, psilocybin, lysergic acid diethylamide [LSD], and mescaline) have anxiolytic and antidepressant properties, but their effects on REFE are not well understood. The purpose of the study was to conduct a systematic review analyzing the effects of serotonergic hallucinogens on REFE in humans.
Methods:
Studies published in the PubMed, PsycINFO, and Web of Science databases until 19 October 2018 which analyzed the effects of serotonergic hallucinogens on REFE in humans were included.
Results:
Of the 62 studies identified, 8 studies were included. Included studies involved the administration of a single or a few doses of LSD or psilocybin, and most trials were randomized and controlled with placebo. LSD and psilocybin reduced the recognition of negative emotions in most studies and modulated amygdala activity to these stimuli, which was correlated with antidepressive effects in patients. Both drugs were well tolerated.
Conclusions:
Serotonergic hallucinogens reduced the recognition of negative emotions by modulating amygdala activity. Despite the small sample sizes, results suggest that serotonergic hallucinogens show promising beneficial effects on deficits in REFE.
Keywords
Introduction
Social cognition is the individual’s ability to capture, process, and generate responses based on the intentions, reactions, and behavior of other people, one of its aspects being the recognition of emotions in facial expressions (REFE).1,2 Some studies show that people with anxiety and mood disorders have deficits in the recognition of facial expressions. 3 For example, in social anxiety disorder, which is characterized by fear of undergoing criticism or negative judgment in social situations, there is hypervigilance to facial expressions of fear, sadness, and joy, and these expressions act as indicators of threat or social reinforcement according to the phenotype of the disorder. 1
In the experimental and clinical setting, facial expression recognition is assessed through tasks. Usually, six main facial expressions that characterize basic human emotions, that is, anger, fear, disgust, surprise, sadness, and happiness, are used in these tasks. In these tasks, subjects have to determine the emotional state expressed on the face of an actor presented to him by means of an image (stimulus) without other contextual information. Such tasks can be classified by means of accuracy 4 or sensitivity. 1 In accuracy tasks, participants may be asked to identify the emotion expressed to the presented stimuli or to discriminate between two different facial expressions (e.g. which of the two emotions presented is the most expressive). 2 In sensitivity tasks, different intensities of facial emotion from the same image are presented. Therefore, it is possible to calculate the intensity of the corresponding facial emotion so that the expressed stimulus is correctly identified. 2
In recent years, research has suggested that the therapeutic effects of drugs used to treat anxiety and mood disorders seem to be mediated, at least in part, by improvements in REFE.3,5 In the case of depression, for example, the reduction of depressive symptoms produced by traditional antidepressants manifests only a few weeks after the onset of treatment. However, improvement in facial recognition deficits seems to occur more rapidly, indicating a beneficial effect on emotional processing prior to the reduction of depressive symptoms. 3 In the case of medications used in the treatment of anxiety disorders, acute administration of selective serotonin reuptake inhibitors (SSRIs) and/or serotonin/norepinephrine reuptake inhibitors (SNRIs) increases the recognition of happiness, but continuous use of SSRIs (and benzodiazepines) increases the recognition of negative emotions while the use of SNRIs decreases it. 5 However, there is much debate about the observation of changed emotional recognition with acute SSRI administration, since this has not been systematically replicated.
Another serotoninergic drug that shares the mechanism of action with SSRIs and has evident effects on emotion processing is methylenedioxymethamphetamine (MDMA) or ‘ecstasy’. 6 MDMA has been shown to consistently reduce the identification of negative emotions in tasks of face recognition, but the results for the enhancing of identification of positive emotions are less consistent.7–11 MDMA also decreases the activity of the amygdala and increases activity of the prefrontal cortex, 12 a neurobiological mechanism that seems to be the basis of emotional regulation in subjects with anxiety disorders.
In this context, recent preclinical and clinical studies have demonstrated the potential of serotoninergic hallucinogens in the treatment of mood and anxiety disorders and drug dependence.13–16 These substances include lysergic acid diethylamide (LSD), psilocybin, ayahuasca/dimethyltryptamine (DMT), and mescaline, and they act as agonists at 5-HT2A serotonergic receptors, which are present in regions of the brain involved in emotional processing, such as the amygdala, hippocampus, and prefrontal cortex. 14 Moreover, neuroimaging studies imply that the anxiolytic and antidepressant effects of serotoninergic hallucinogens appear to be related to the effects of these drugs on brain areas linked to emotional processing in general and social cognition specifically.14,15
Therefore, considering that (a) antidepressant and anxiolytic drugs currently available are not effective for all groups of patients and their use is often accompanied by undesirable side effects, 17 (b) one of the possible mechanisms of action for traditional antidepressants is the improvement in REFE, and (c) recent research suggests that serotoninergic hallucinogens have anxiolytic and antidepressant effects that could be modulated by their effects on emotional processing, the purpose of this study was to present a systematic review of the effects of serotonergic hallucinogens in the recognition of facial expressions, one of the main factors involved in social cognition.
Methods
Data for this systematic review was collected in accordance with the systematic reviews and meta-analyses guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA]). 18
Search strategy
The electronic search was performed using the PubMed, PsycINFO, and Web of Science databases. The following search terms were used: (ayahuasca OR DMT OR psilocybin OR LSD OR mescaline) AND (emotional face discrimination OR emotional face recognition OR facial emotion recognition OR emotional faces OR facial expressions OR emotional face expressions OR emotion recognition). All studies published until 19 October 2018 were included, without any language restriction.
Selection criteria and study selection
The inclusion criteria were: (a) studies in humans without restrictions of sex and age; (b) experimental studies involving the administration of a serotonergic hallucinogen (i.e. ayahuasca, DMT, psilocybin, LSD, or mescaline); (c) studies that evaluated the recognition of facial expressions; (d) articles in any language. The exclusion criteria were: (a) animal studies; (b) articles that did not use a serotonergic hallucinogen as intervention; (c) articles that used a serotoninergic hallucinogen but did not use a task of recognition of facial expressions; (d) review articles; (e) observational studies; (f) case reports; (g) letters to the editor.
After excluding duplicates, the titles and abstracts of all articles were reviewed. Publications that clearly did not meet the inclusion criteria were excluded. The decision to include or exclude publications was based on a revision of the full texts. The entire process was conducted by two reviewers independently: the electronic search was conducted by two of the authors independently, who then checked the selection made by the other and they decided together which would be the selected citations. In cases of disagreement, the reviewers discussed their reasons for inclusion or exclusion and if a consensus was not reached, a third author/reviewer was consulted to decide if that citation should be included based on the exclusion and inclusion criteria.
Recorded variables, data extraction and analysis
The variables included were: authors; year of publication; study location (country); study design (open label or placebo controlled); number of subjects; type of drug (i.e. LSD, psilocybin, ayahuasca, DMT, or mescaline); dosage (quantity and frequency); facial recognition task (primary variable) and other main results such as subjective measures and neuroimaging results (secondary variables).
Results
Identified studies
A flow diagram illustrating the different phases of the systematic review is presented in Figure 1.

Flow diagram identifying the different stages of the systematic review.
Identification of studies
The bibliographic search resulted in 62 articles in the first stage, of which 22 were duplicates. A total of 40 articles were analyzed, and 8 articles were selected in accordance with the inclusion and exclusion criteria. The full texts of these references were obtained for a more detailed evaluation. After reading the studies in full, seven articles were included in this review and one article was excluded because it used a mind theory test (another aspect of social cognition other than recognition of facial expressions) and assessed facial emotions by the eye region. 19 The seven included studies were classified according to the substance under investigation, and comprised five double-blind, randomized, crossover, placebo-controlled trials and two open-label studies, of which two used LSD (both with healthy volunteers and placebo controlled), and five used psilocybin (three studies in healthy volunteers and placebo controlled, and two open-label studies in patients with treatment- resistant major depression disorder). Only articles with psilocybin and LSD were found.
In spite of the limited number of studies (mainly because this is a very recent area of investigation and also these substances are banned in most of the world), the small sample size (20–40 healthy subjects, 17–20 patients with depression), and the underexplored potential of serotoninergic hallucinogens for treatment anxiety and mood disorders, the results are unanimous for the good tolerability of these drugs, which were administered in single doses in most studies. The studies also reported that these drugs reduced the recognition of negative emotions. Importantly, considering the heterogeneity of the studies regarding drugs, dosage, sample characteristics, and tasks used, it was not possible to perform a quantitative analysis or meta-analysis. Therefore, we performed a qualitative synthesis of the data. These findings are discussed in detail below and are presented briefly in Table 1.
Main results of the selected studies for the systematic review.
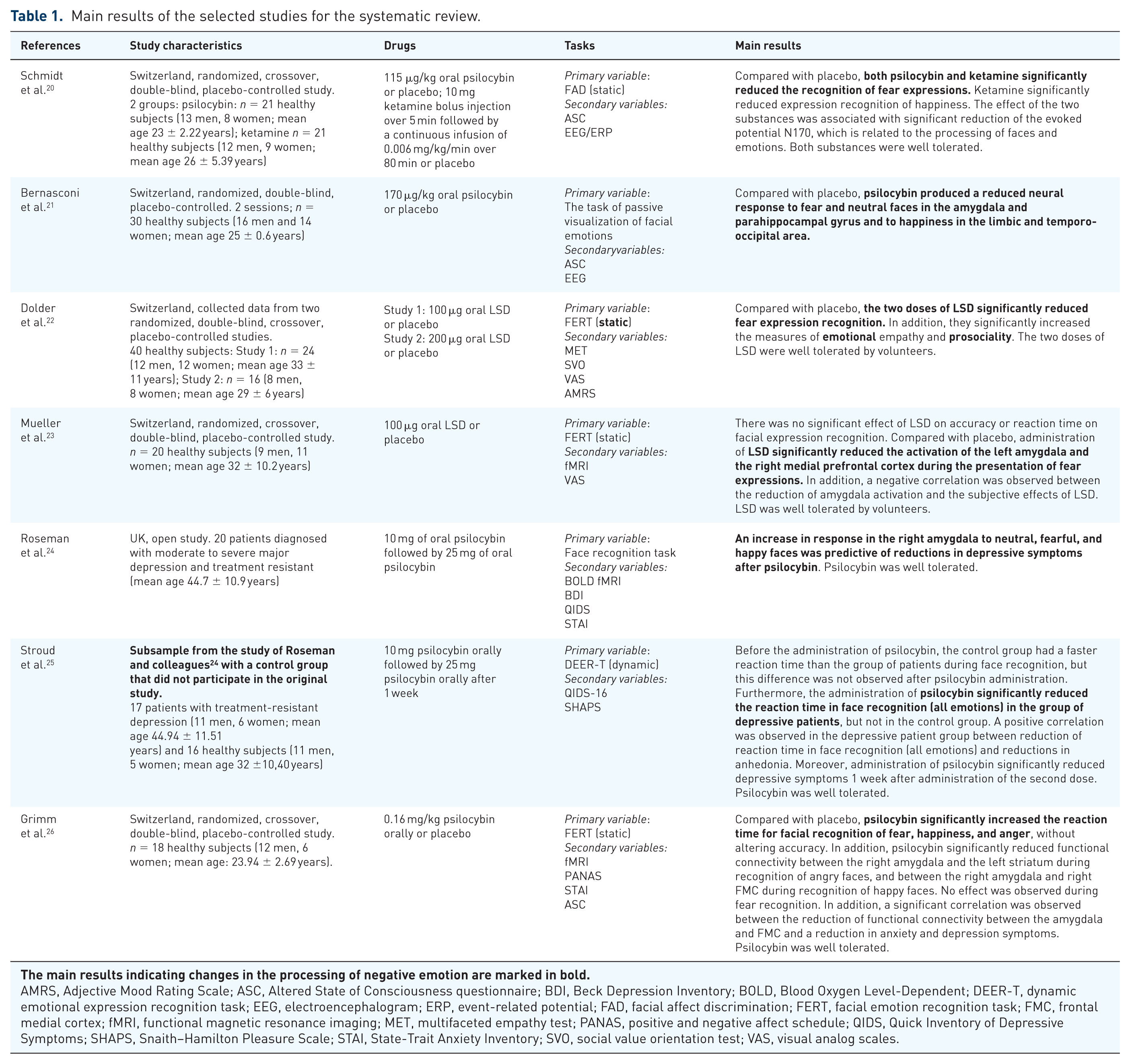
AMRS, Adjective Mood Rating Scale; ASC, Altered State of Consciousness questionnaire; BDI, Beck Depression Inventory; BOLD, Blood Oxygen Level-Dependent; DEER-T, dynamic emotional expression recognition task; EEG, electroencephalogram; ERP, event-related potential; FAD, facial affect discrimination; FERT, facial emotion recognition task; FMC, frontal medial cortex; fMRI, functional magnetic resonance imaging; MET, multifaceted empathy test; PANAS, positive and negative affect schedule; QIDS, Quick Inventory of Depressive Symptoms; SHAPS, Snaith–Hamilton Pleasure Scale; STAI, State-Trait Anxiety Inventory; SVO, social value orientation test; VAS, visual analog scales.
Drugs
Psilocybin
The first study found in the search was by Schmidt and colleagues published in 2013. They conducted a randomized, crossover, double-blind, placebo-controlled study in Switzerland. It was carried out with two groups of healthy subjects: the first group of 21 subjects (13 men, 8 women; mean age 23 ± 2.22 years) received a dose of 115 μg/kg oral psilocybin or placebo; the second group also had a sample of 21 subjects (12 men, 9 women; mean age 26 ± 5.39 years) who received a bolus injection of 10 mg ketamine over 5 min followed by a continuous infusion of 0.006 mg/kg/min over 80 min or placebo. 20 This study used event-related potentials to compare the effects of the two drugs on conscious and nonconscious facial processing. They used a static task, facial affect discrimination (Ekman and Friesen series), to assess the accuracy of the recognition of emotional expressions neutral faces and faces of fear and happiness. 20 It was observed that compared with placebo, both psilocybin and ketamine significantly reduced fear expression recognition. In addition, ketamine also significantly reduced facial expression recognition of happiness. The effect of these two substances was associated with reduction of the evoked potential N170, which is related to the processing of faces and emotions. 20 Both substances were well tolerated.
This result was one of the first to show that psilocybin (a 5-HT2A receptor agonist) modulates the processing of facial expressions. 20 However, the spatiotemporal dynamics of the neurophysiological changes associated with these effects was not explored. To further elucidate this issue, Bernasconi and colleagues in Switzerland conducted a randomized, double-blind, placebo-controlled study evaluating REFE (neutral compared with the basic emotional expressions: sad, angry, happy, disgust, surprise, and fear) during the effects of psilocybin compared with placebo measuring evoked potentials with electroencephalography. Two sessions were conducted involving psilocybin (170 μg/kg) administered orally or placebo 2 weeks apart. 21 The sample consisted of 30 healthy subjects (16 men and 14 women; mean age 25 ± 0.6 years). They used the facial emotion recognition task (FERT) (Ekman and Friesen series), comparing neutral faces with other basic faces of emotional expressions. 21 Compared with placebo, psilocybin promoted processing of facial expressions at different regions of the brain and times, inducing a reduced neural response to fear and neutral faces in the amygdala and parahippocampal gyrus at 168–189 ms and a decreased response to the happy faces in the limbic and temporo-occipital area at 211–242 ms. 21
By 2017, no study had evaluated whether psilocybin would cause long-term changes in facial emotional processing in people with depression, and whether this would be associated with changes in depressive symptomatology. In the UK, Roseman and colleagues conducted an open study in a sample of 20 patients with treatment-resistant depression (11 men, 9 women; mean age 44.7 ± 10.9 years). 24 This study investigated the contrast between the recognition of neutral faces and faces of fear and happiness and the response of the amygdala using a passive task, FERT (Karolinska Directed series) and Blood Oxygen Level-Dependent (BOLD) functional magnetic resonance imaging (fMRI) after administration of psilocybin (10 mg followed by 25 mg with 1-week interval) in patients with depression. 24 An increased response to faces of fear and happiness in the right amygdala was observed. It was also noted that altered recognition of fear and neutral faces was predictive of clinical improvement. 24
In 2018, the same group compared the same sample of depressed patients with a control group of 16 healthy subjects that did not participate in the original study (11 men, 5 women; mean age 32 ± 10.40 years) to assess the effects of psilocybin on emotional processing. 25 They used a dynamic task, dynamic emotional expression recognition task (NimStim Face Stimulus Set), and evaluated the accuracy and reaction time to neutral faces and faces of happiness, anger, sadness, disgust, and fear. The control group showed a faster reaction time compared with the depressive patients in face recognition (i.e. neutral, happiness, anger, sadness, disgust, fear), but this difference was not observed after the administration of psilocybin. Furthermore, there was a significant reduction in the reaction time of face recognition (all emotions) in the depressive patients after the intervention, but not in the control group. 25 There was also a significant positive correlation between the reduction in reaction time in face recognition (all emotions) and anhedonia reduction in the depressive patients. Moreover, a reduction of depressive symptoms in patients was noted 1 week after administration of the second dose of drug processing. 25 Psilocybin was well tolerated.
In the same year, Grimm and colleagues in Switzerland tested whether psilocybin would alter the connective pattern of the amygdala during facial expression recognition. To verify this hypothesis, they performed a randomized, double-blind, placebo-controlled, crossover study using a static task, FERT (STOIC face database), to verify the accuracy and reaction time in the recognition of faces of happiness, anger, and sadness using fMRI. 26 The oral dose of psilocybin was 0.16 mg/kg with a sample of 18 healthy subjects (12 men, 6 women; mean age 23.94 ± 2.69 years). It was verified that psilocybin significantly increased the reaction time for fear, happiness, and anger face recognition without altering the accuracy when compared with placebo. 26 A reduction in functional connectivity was observed between the right amygdala and the left striatum in anger face recognition and between the right amygdala and the right frontal medial cortex during the recognition of happy faces. No effect was observed in fear recognition. There was also a significant correlation between reduced functional connectivity in the amygdala and frontal medial cortex and a reduction in anxiety and depression scores. Psilocybin was well tolerated. 26
LSD
In 2016 a study conducted in Switzerland by Dolder and colleagues collected data from two randomized, crossover, double-blind, and placebo-controlled studies involving the administration of LSD to healthy volunteers. In the first study, 100 μg of oral LSD or placebo was given to 24 healthy subjects (12 men, 12 women; mean age 33 ± 11 years); in the second study, the dosage was 200 μg oral LSD or placebo in 16 healthy subjects (8 men, 8 women; mean age 29 ± 6 years). 22 The experimental sessions had a washout period of at least 1 week. The study evaluated the acute effects of LSD on the recognition of facial expressions using FERT (Ekman and Friesen series) to evaluate the accuracy of the recognition of faces of fear, anger, happiness, and sadness, and also assessed empathy using the multifaceted empathy test. 22 Authors observed that both doses of LSD significantly reduced fear expression recognition and increased emotional but not cognitive empathy and enhanced prosociality measures when compared with placebo. In addition, the two doses of LSD were well tolerated by volunteers. 22
In a subsample of 20 subjects from the study above, Mueller and colleagues evaluated the effect of LSD on the amygdala response to fear stimuli and whether this would be associated with the subjective effects of that substance. 23 They used a static task, FERT (Ekman and Friesen series), and evaluated the recognition of neutral faces and faces of fear. Compared with placebo, LSD significantly reduced the activation of the left amygdala and the right medial prefrontal cortex during the presentation of fear expressions. Moreover, a negative correlation was noted between the reduction of amygdala activation and the subjective effects of LSD. As in the study cited above, LSD was well tolerated by volunteers.
Discussion
We performed a systematic review to evaluate the effects of serotonergic hallucinogens in REFE. Included studies involved the administration of a single or a few doses of LSD or psilocybin. Both drugs were well tolerated. Our most consistent finding was that these drugs reduced the recognition of negative emotions and modulated amygdala activity to these stimuli. This effect was correlated with antidepressive effects in depressed patients, but since this was observed only in a single study with an open-label design, it is difficult to conclude if this result has any clinical relevance.
Most of the selected studies met the basic methodological rigor required for clinical trials by using double-blind, placebo-controlled designs, but all studies were of small size, and some did not use placebo or an adequate control group. Moreover, the use of different drugs, doses of the same drugs, and distinct tasks to evaluate REFE with different variables presented for analysis show how heterogeneous the studies were. For instance, the facial expression recognition tasks (primary variable) utilized in the studies presented divergent characteristics: (a) type of task (dynamic, static, or passive visualization); (b) image database (Ekman and Friesen series, NimStim Face Stimulus Set, Karolinska Directed, while others did not cite the database); (c) facial expressions (e.g. some studies used all the basic facial expressions, others compared neutral facial expression with the maximum intensity of facial expression of a given emotion, etc.); (d) measured variable (some evaluated the accuracy, others the accuracy and reaction time, and still others neurophysiological variables and neuroimaging). However, the variety of tasks used could be considered a strength of the studies, since results were similar in different tests. Indeed, it is interesting to note that despite the differences between tasks, the results consistently reported a change in the recognition and processing of negative emotions.
Moreover, these compounds share a common mechanism of action, which consists in an agonism at cortical 5-HT2A receptors expressed in areas of the brain related to emotional processing, such as the amygdala. 14 Since the amygdala is a region of the brain involved in the processing of anxiety and fear, the modulation of activity in this region rich in 5-HT2A receptors by classic hallucinogens seems to be the neural basis behind the effects of these compounds on emotions. 14
Furthermore, the present results with classical serotoninergic hallucinogens show similar and overlapping results with the effects of traditional drugs used to treat anxiety and mood disorders regarding alterations in REFE. REFE plays an important role in mood and anxiety disorders. For instance, a feature common to these disorders is deficits in the recognition of basic facial expressions.1–5 In addition, there is evidence that positive changes in REFE are predictive of clinical improvement.1–5 Studies indicate that traditional drugs used in the treatment of anxiety and depression cause positive changes in REFE, for example, 7 days of treatment with SSRIs results in a reduction in the recognition of negative facial expressions (i.e. anger, fear, disgust, and surprise), while acute administration of SNRIs increases the recognition of happy faces.3,5 Moreover, administration of benzodiazepines is associated with decreased identification of negative emotions. 5
The present review suggests that these effects also appear to be common with classic hallucinogens. Indeed, the studies reviewed showed that a single dose or a few doses of LSD or psilocybin was associated with a modified pattern of recognition of negative emotions that could be interpreted as beneficial, since several of these studies showed that these modifications were correlated with increases in positive mood and/or anxiolytic and antidepressant effects. Although the present review analyzed only a few studies with small sample sizes, it does suggest that the effects of these compounds on REFE could be at least one of the mechanisms involved in their anxiolytic and antidepressant effects.15,17,27 Furthermore, there is also evidence that the serotonergic drug MDMA consistently reduces identification of negative emotions in tasks of face recognition7–11 and decreases the activity of the amygdala. 12 These mechanisms, associated with the capacity of MDMA to enhance serotonergic tone in the prefrontal cortex, could be shared mechanisms with traditional antidepressants and classic hallucinogens for emotional regulation in subjects with mood and anxiety disorders.
However, it is important to acknowledge that traditional antidepressants and anxiolytics do not necessarily share common pharmacological mechanisms of action. Indeed, serotonergic hallucinogens are partial agonists of cortical 5-HT2A receptors, while traditional antidepressants are often inhibitors of monoamine uptake (especially serotonin and norepinephrine). What seems to be common among these drugs is their capacity to increase neuroplasticity, which could be involved in their capacity to improve symptoms by changes in the neurocircuitry involved in emotional processing.3,5,14
Furthermore, serotonergic hallucinogens also act as agonists at other serotonergic receptors, such as the 5-HT1A and 5-HT2C, which could contribute to the effects of these drugs on emotional processing. 14 In order to assess the causal role of the 5-HT2A receptor in the effects of classical hallucinogens and traditional antidepressants, it would be necessary to administer a specific 5HT2A antagonist along with psychedelics and SSRIs in an emotional processing paradigm.
There is also evidence of increased responses from the amygdala to negative faces in patients with depression.28,29 Treatment with antidepressants has a modifying effect on the amygdala, for example, after 7 days or more of treatment with an SSRI there is a normalization of hyperactive responses from this brain region that precedes changes in clinical status. 3 Regarding classical hallucinogens, the neuroimaging studies analyzed in the present review observed a reduction of amygdala activity during the recognition of the faces of fear after a single dose of LSD or psilocybin. Furthermore, other studies not included in the present review because they did not evaluate the effects of classical hallucinogens on REFE also suggest that modulation of amygdala activity is a core effect of these drugs, although other frontal and limbic structures also seem to be involved.15,17,27
It is interesting to note that there is a direct relationship between these substances and the amygdala in healthy subjects, since hyperactivation of this brain structure is directly related to anxiety and mood disorders. In addition, the modifications observed in the amygdala suggest that the neural basis of the anxiolytic and antidepressant effects of these substances may be directly related to this brain structure, as well as the classic antidepressants and anxiolytic drugs. However, Roseman and colleagues reported an increased response of the amygdala to the faces of fear in patients with treatment-resistant depression and psilocybin, which was associated with reductions in depressive symptoms. It is possible that the neural effects of psilocybin and other classic hallucinogens are different in healthy volunteers and patients with anxiety and mood disorders. 24 For instance, neuroimaging studies with ayahuasca reported different brain activation patterns between healthy volunteers and depressed patients. 30
Finally, LSD and psilocybin showed good tolerability, evidenced by the occurrence of few adverse reactions in all the studies evaluated. These results are consistent with the research performed in the last decades involving the acute administration of classic psychedelics.14,17
Conclusion
This systematic review presented data suggesting that serotonergic hallucinogens produce modifications in REFE leading to reduced recognition of negative emotions, which could have therapeutic utility in disorders characterized by deficits in facial expression recognition such as anxiety and depression. If these results are replicated, this would mean that these drugs could be clinically useful in treating these deficits and, thus, depression and anxiety symptoms.
The effects of classical hallucinogens seem to be shared with traditional antidepressants and anxiolytics, but the effects of both classes of drugs in social cognition still need to be replicated in larger trials. Moreover, these two classes of drugs have different mechanisms of action. Therefore, experimental studies using antagonists of the 5-HT2A receptor would shed light in the possible causal role of these receptors in the observed effects produce by these drugs. Functional neuroimaging studies would also improve our understanding of the possible participation of regions of the brain rich in 5-HT2A receptors (such as the amygdala) in the effects of serotonergic hallucinogens on facial expression recognition.
Major limitations of the present systematic review include the limited number of studies included and their small sample sizes, and the lack of placebo or an adequate control group. However, despite these important limitations, the revised results suggest that although the mechanisms of action responsible for the effects produced by serotonergic hallucinogens are not fully understood, the evidence indicates that these drugs reduce recognition of negative emotions and these effects were predictive of clinical improvement in an open-label trial with depressed patients.
Further controlled studies with larger samples and long-term administration to clinical populations are needed to determine better the effects of serotonergic hallucinogens on REFE and the possible use of these drugs to treat anxiety and mood disorders.
Footnotes
Authors’ Note
Rafael G. dos Santos is also affiliated with National Institute of Science and Technology - Translational Medicine, Ribeirão Preto, SP, Brazil and ICEERS Foundation (International Center for Ethnobotanical Education, Research and Services), Barcelona, Spain.
Funding
JMR received funding from the Fundação de Amparo à Pesquisa do Estado de São Paulo, Brazil. GNR received funding from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, Brazil. RGS is a Fellow of the Programa Nacional de Pós-Doutorado, Brazil. JASC and JECH received a CNPq (Brazil) Productivity Fellowship Award. Sponsors had no role in the study design, data analysis, data interpretation, or writing of the report. All authors had full access to all the data and had final responsibility for the decision to submit for publication.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.