
Abstract
Intentional drug overdoses with antidepressant and antipsychotic medications are an increasingly common problem. Currently, there is little guidance with regard to reintroduction of these medications after intentional overdoses. We have used published toxicological and pharmacokinetic data to obtain factors which control the recovery from overdoses. From such data, we have proposed guidance regarding their reintroduction, provided there are no adverse effects or contraindications. Tentatively, we suggest that when adverse effects from the overdose are lost, treatment could recommence after a further mean half-life of elimination. Most antidepressant and antipsychotic drugs are metabolized by cytochrome P450 enzymes and, where cytochrome P450 inhibitors are co-ingested, serial plasma concentrations should optimally be obtained in order to assess a suitable time for reintroduction of the psychoactive drugs. We hope the proposals presented will stimulate research and discussion that lead to better guidance for clinicians concerning reintroduction of psychoactive medication after intentional overdose.
Keywords
Introduction
Self-poisonings account for 1–2% of all attendances to emergency departments. 1 Drugs commonly used in overdose include paracetamol, nonsteroidal anti-inflammatory drugs, opioids, benzodiazepines, antidepressants and antipsychotics. These are often taken in combinations and co-ingested with alcohol. 2 Patients with psychiatric disorders have high rates of deliberate self-poisoning using their prescribed drugs.1,3,4 Recurrent overdoses are also common. 2
In clinical practice, we have been struck by the lack of guidance concerning the timing of reintroduction of antidepressant or antipsychotic medications after overdose. Reintroduction exposes patients to hazards that concern clinicians. These include toxicity if the drug is reintroduced prematurely or return of suicidality or exacerbation of psychiatric condition if recommencement is delayed. This question about when to restart in patients is, in our clinical experience, very common and often a vexed one. However, it has received little attention and there is little help to be found. Other common questions are whether there are drug interactions and whether smoking after an overdose could complicate drug therapy. Although there are well-established guidelines for the management of initial presentation of overdoses, the time of restarting, or dosage of the reintroduced psychoactive medicines requires much further consideration.
To begin addressing the question of the most appropriate time to recommence needed medicines for psychiatric disorders after an overdose, we reviewed the literature to obtain data on the recovery from overdose and guidance on drug recommencement. Subsequently, we made tentative recommendations concerning the re-establishment of pharmacotherapy. Hopefully, this work will stimulate the formulation of guidelines regarding restarting these therapies after overdoses.
We focused on the antidepressant and antipsychotic medications commonly used and sought to answer questions frequently asked by clinicians: ‘How long will the overdosed medications take to reach safe concentrations that will allow recommencement of these psychoactive drugs?’, ‘What are the most severe adverse effects of overdoses of antipsychotic and antidepressant drugs?’, ‘What are the likely interactions with other medications?’ and ‘Will cigarette smoking or nicotine replacement therapy have any impact?’
Literature searches and results
An initial literature search was conducted using the EMBASE, MEDLINE, PubMed and PsycINFO databases. Search terms used were ‘psychotropic, antidepressant, antipsychotic, over-dose, intentional overdose, poisoning, suicide, suicidal’, AND synonyms of ‘restart or re-start, recommence or re-commence, reintroduce or re-introduce, reinitiate or re-initiate, begin again or start again’. This first literature search identified 221 articles, excluding duplicates. All titles and abstracts were read. Criteria for full-text review were any paper concerning cases or reviews of overdose with antidepressants or antipsychotics: four articles were found. Further manual searches of the bibliographies of these four articles were performed to identify further relevant articles, with the final inclusion criterion being any article that documented the approaches taken for the management of these episodes, in particular, with respect to the restarting of antidepressant or antipsychotic medications after overdoses. However, only three fit the final inclusion criterion.5–7 These three reports are summarized in Table 1. Exclusion criteria were publications describing overdoses of primarily illicit substances and accidental overdoses in children.
Reports with discussion on recommencement of psychoactive drug after overdose.

MAOI, Monoamine oxidase inhibitor.
The few relevant references retrieved necessitated further manual searches of the databases to identify other factors, such as pharmacokinetics, which may be significant in the recommencement of these psychoactive medications after overdoses. Consequently, search terms used included names of individual drugs AND overdose, toxicokinetics, pharmacokinetics, cytochrome P450 (CYP) enzyme, metabolism, or active metabolites. The bulk of this review is derived from this category of references.
Factors relevant to recommencement of psychoactive medicines after overdose
The sections below discuss factors which are known to affect the intensities of symptoms of drug overdoses commencing with general principles then followed by a description of the relevant pharmacological, toxicological, toxicokinetic and pharmacokinetic parameters of individual drugs. Many of the latter data are summarized in Tables 2 and 3. The final section, ‘Conclusion and future directions’, contains suggestions for future research that might lead to better guidance for clinicians about restarting psychoactive medications following overdose.
Summary of toxicology and toxicokinetics of antidepressant drugs.
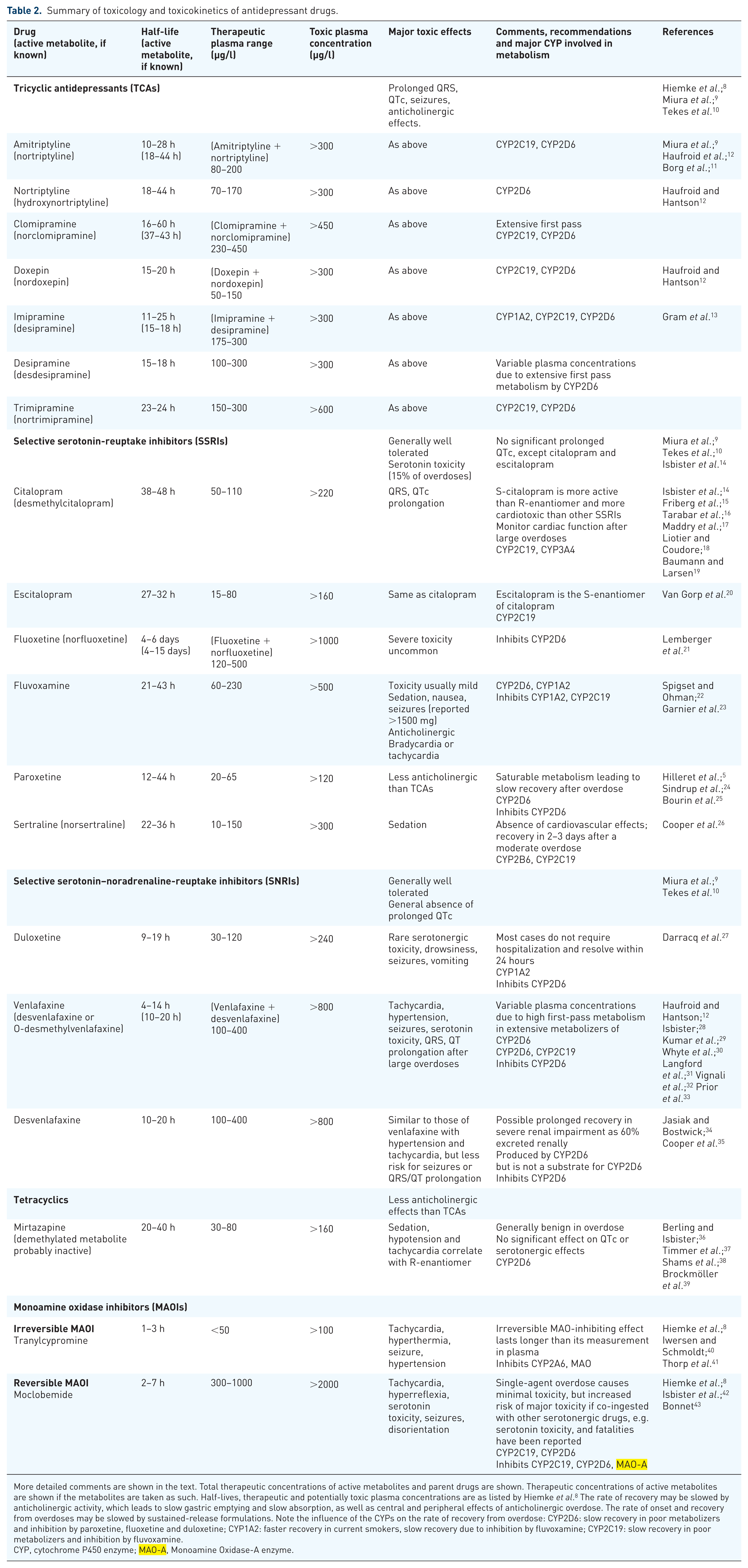
More detailed comments are shown in the text. Total therapeutic concentrations of active metabolites and parent drugs are shown. Therapeutic concentrations of active metabolites are shown if the metabolites are taken as such. Half-lives, therapeutic and potentially toxic plasma concentrations are as listed by Hiemke et al. 8 The rate of recovery may be slowed by anticholinergic activity, which leads to slow gastric emptying and slow absorption, as well as central and peripheral effects of anticholinergic overdose. The rate of onset and recovery from overdoses may be slowed by sustained-release formulations. Note the influence of the CYPs on the rate of recovery from overdose: CYP2D6: slow recovery in poor metabolizers and inhibition by paroxetine, fluoxetine and duloxetine; CYP1A2: faster recovery in current smokers, slow recovery due to inhibition by fluvoxamine; CYP2C19: slow recovery in poor metabolizers and inhibition by fluvoxamine.
CYP, cytochrome P450 enzyme; MAO-A, Monoamine Oxidase-A enzyme.
Summary of toxicology and toxicokinetics of antipsychotic drugs.

CYP, cytochrome P450 enzyme.
Overdose ingestion/history
A surprising aspect of drug overdose is the accuracy of estimation of the size of the overdose based upon the patient’s, or family or friend’s history of the overdose. 28 Adequate fitting by the population pharmacokinetic procedure is possible if the doses are known with some accuracy (see section ‘Toxicokinetics’). Accordingly, the general conclusion is that the reported magnitude of overdoses can be reliable although can also be far from accurate in some patients. Polypharmacy drug overdoses are also common; these have important implications in the pharmaco-dynamic and -kinetic interactions (see following sections).
Absorption of overdosed drugs
In the instance where patients have presented early enough following an overdose, decontamination may be undertaken if safe, to reduce absorption or increase elimination. However, not all psychoactive drug ingestions benefit equally from the use of decontamination. 29 The absorption of most orally administered drugs is dependent upon their gastric emptying, as absorption commences significantly in the small intestine. Several drugs, including the tricyclic antidepressants, are absorbed slowly after overdose. Taking the tricyclics as a group, median gastric emptying half-time is 103 min. 67 Adams and colleagues suggested that slow gastric emptying was due to the anticholinergic effects together with the stress associated with the overdose. 67
Ingestion of sustained-release tablets or capsules, such as venlafaxine or quetiapine, can decrease the rate of absorption compared with standard-release formulations. The rate of onset and recovery from overdose may be slowed accordingly. Overdose of sustained-release quetiapine tablets has been reported to form bezoars55,68 (gelatinous masses) in the stomach, which can further prolong or delay absorption.
Elimination of overdosed drugs
Most antidepressant and antipsychotic drugs have moderately long half-lives in the range of 12–36 h (Tables 2 and 3).
Psychoactive drugs are largely metabolized by one or more of the CYPs in the liver. As is the case with all CYPs, their activity is under genetic control and, as a result, the activities of the CYPs show considerable interpatient variation. This results in marked interpatient differences in the half-lives or clearances of antidepressant, antipsychotic drugs and their metabolites.
CYP2D6 is of particular importance because its enzyme activity can be divided into three classes: extensive (i.e. normal metabolizers); poor (with either inactive or low-activity CYP2D6); or ultrarapid metabolizers owing to genetic polymorphisms. The division explains some major differences in the rates of recovery from overdoses of some antidepressant and antipsychotic drugs. Thus, relatively slow recovery is anticipated from overdoses if the patient carries the low-activity or absent CYP2D6, with more rapid recovery in extensive or ultrarapid metabolizers. Between 5% and 10% of Europeans and approximately 1% of Asians are poor metabolizers via CYP2D6. The genetic background to these is complex and the contrast between these divisions is clinically significant.
Seven variants of CYP2C19 have also been associated with slow metabolism of several antidepressants (Table 2). Slow recovery after overdoses is anticipated in patients with low-activity CYP2C19. Slow recovery is also anticipated in patients receiving proton-pump inhibitors, particularly omeprazole and esomeprazole, as these are potent inhibitors of CYP2C19. 69 On the other hand, some patients are ultrafast CYP2C19 metabolizers. They should have relatively rapid recovery from overdoses of drugs that are metabolized by this enzyme.
A frequent initial step in the metabolism of many drugs, including psychoactive drugs, is N-demethylation, commonly catalysed by CYPs. An example of N-demethylation is the conversion of a tertiary amine to a secondary amine by loss of a methyl group (CH3; Figure 1). The prefixes ‘desmethyl’, ‘des’ or ‘nor’ in the metabolite’s name all refer to the demethylated metabolite. The formation of desipramine from imipramine is an example. Demethylation of a methyl ether is less common in psychoactive drugs but venlafaxine undergoes this reaction (Figure 1).

Metabolic demethylation of tertiary amines and ethers catalysed by cytochrome P450 enzymes.
Drug interactions
Two types of drug interaction should be noted.70,71
(1) Pharmacodynamic interactions: potentiation or antagonism due to the mechanisms of action of two or more drugs. For example, the ingestion of more than one drug which is cardiotoxic, such as venlafaxine and amitriptyline, may increase the risks for serious arrhythmias. Another example involves physostigmine which increases the availability of acetylcholine at cholinergic nerve terminals and has been used to overcome the anticholinergic effects of overdoses of some psychoactive drugs. Such interactions do not tend to alter the pharmacokinetics of the overdosed drugs and are therefore unlikely to influence the time to recommencement of these drugs.
(2) Pharmacokinetic interactions: metabolic interactions. The mechanism of this type of drug interaction involves inhibition or induction of the metabolism of one drug by a co-ingested drug. Various CYP enzymes can be inhibited or induced by concomitant drugs. Inhibitory interactions lead to increased recovery times after an overdose. Of the psychoactive drugs, the best-known inhibitors of the metabolism of other drugs are paroxetine, fluoxetine and duloxetine mainly through their inhibition of CYP2D6 (Table 2). Metabolic inhibition of other drugs is also a well-known effect of monoamine oxidase inhibitors (MAOIs). Although not widely used in present-day management of depression, it is of note that prolonged recovery may be produced by combinations of MAOIs and other drugs. On the other hand, induction of CYP3A4 occurs after chronic usage of other unrelated drugs, such as carbamazepine, phenytoin, rifampicin and herbal preparations such as St John’s wort (Hypericum perforatum), 72 with predicted faster recovery times after overdosage of drugs metabolized by CYP3A4. Fluvox-amine also prolongs the half-lives of drugs and consequently slows the recovery from drugs metabolized by CYP1A2 and CYP2C19 (Table 2).
Effects of smoking and illicit drugs
Chronic tobacco smokers have induced hepatic CYP enzymes, particularly CYP1A2. It is presumed that the induction is caused by polycyclic aromatic hydrocarbons from tobacco smoke, not by the inhaled nicotine. Not surprisingly, the extent of induction increases with the level of smoking. CYP1A2 is a relevant enzyme in the metabolism of commonly prescribed psychoactive medications, including clozapine, duloxetine, olanzapine and imipramine (Tables 2 and 3). In terms of drug overdose, faster recovery from overdose is anticipated in smokers.
In patients treated for overdose, tobacco smoking usually ceases, possibly for days and even weeks during hospitalization. Cessation of smoking leads to an increased half-life of the drugs over about 4 days as induction of the CYP1A2 wears off,8,73 which may slow the rate of recovery. However, we suggest that cessation of smoking, should not greatly change the rate of recovery of an overdose of any antidepressant or antipsychotic drug. Two reasons may be put forward for this prediction. First, patients recover from most overdoses within 1–4 days. Second, other than clozapine, most antidepressant and antipsychotic drugs with long half-lives (fluoxetine, paroxetine and aripiprazole) are not metabolized by CYP1A2 (Tables 2 and 3).
Similar to tobacco smoking, cannabis smoking induces the metabolism of several drugs via CYP1A2 but effects on the half-lives and rates of recovery of other drugs are limited to regular smokers of marijuana (two or more joints per week). 73
Availability of drug assays
The treatment of many overdoses can be assisted by identification of the overdosed drug and measurement of the plasma concentrations. The identification of drugs in urine is available in many hospitals but the assay of plasma samples generally requires the samples being forwarded to specialized laboratories, thus the receipt of the results is generally slow, often well after the clinical management of the acute features of the drug overdose. This problem may, however, be overcome in the future (see section ‘Conclusion and future directions’). Of note, when considering the rates of decline of the plasma concentrations of the psychoactive medicines, many studies have not distinguished between the individual isomers (see below).
Stereoisomers of antidepressant and antipsychotic drugs
The three-dimensional structures of drugs are critical to their pharmacology. Thus, stereoisomers of drugs may have very different pharmacodynamic and pharmacokinetic properties and metabolism. It is noteworthy that many drugs are available as their racemates, that is, an equal mixture of R- and S-enantiomers (mirror images of each other). Paroxetine, duloxetine, escitalopram and sertraline are available as individual isomers but fluoxetine, mirtazapine, venlafaxine, desvenlafaxine, citalopram and paliperidone are administered as racemates. Optimally, plasma concentrations of racemic drugs should be determined by stereospecific assays in order to determine the concentrations of the individual isomers but this is unusual presently.
Patterns of plasma concentrations
The plasma concentrations of overdosed antidepressant and antipsychotic drugs are of major significance in the onset and recovery from symptoms of overdoses. In this regard, three patterns of the time course of plasma concentrations of antidepressants and antipsychotics have been recorded.
(1) A complex pattern including a slow phase. Peak plasma concentrations are generally attained within 12 h but then decline quite rapidly. This is followed by a slow declining phase which, in some cases, may even be interrupted by temporary increases. This slow phase is followed by a terminal phase in which the plasma concentrations decrease in a log-linear fashion. During this terminal phase, the half-life (t1/2) is constant. This pattern is seen with clozapine [Figure 2(a)].
(2) A biphasic pattern after absorption. The initial decline in plasma concentrations is followed by a log-linear phase. This resembles the pattern seen after oral dosage of many drugs and has been recorded in some patients with clozapine [Figure 2(b)].
(3) A monophasic decline. In this pattern, the plasma concentrations of the psychoactive drug decrease in a log-linear fashion following the attainment of peak plasma concentrations. No intermediate, or terminal, slowly declining phase is seen. This pattern was seen with sertraline [Figure 2(c)].
The very slow decline of plasma concentrations of some drugs following the initial rapid decline is considered to be due, primarily, to the anticholinergic properties of the drug taken. This decreases the rate of transit of drugs into the small intestine where drug absorption occurs. The stress associated with the overdose may also slow the absorption of the drug (see section on Absorption of overdosed drugs). Other medicines taken concomitantly, notably opioids, may also contribute to prolonged gastric emptying and drug absorption.
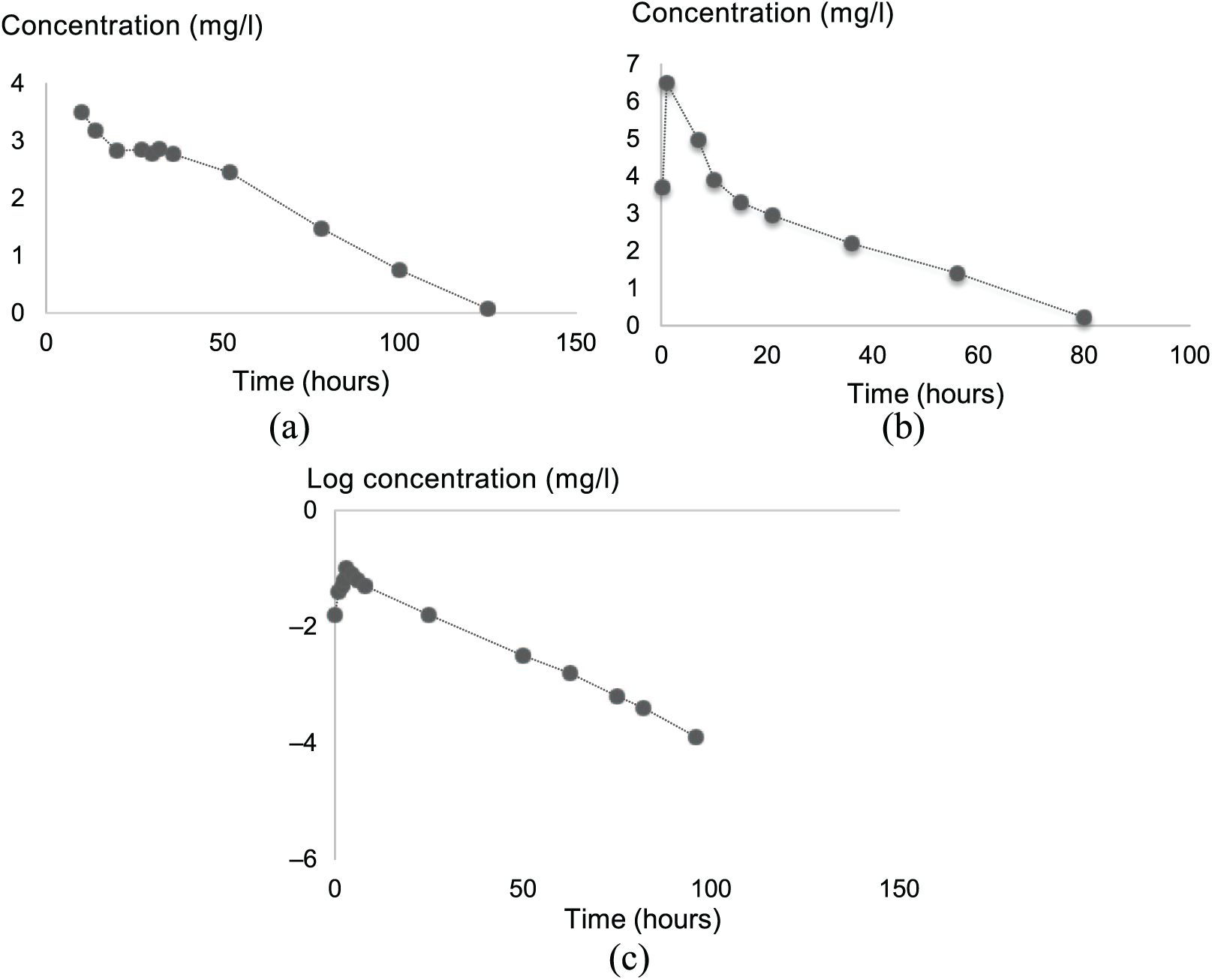
Time courses of plasma concentrations of drugs after overdoses.
Two other mechanisms have been suggested to contribute to the slow initial decline of antidepressants and antipsychotics. The metabolism by the CYPs can be saturated by high concentrations of the drug as seen in overdose. Secondly, secretion of drug or active metabolite into bile can result in enterohepatic recirculation. However, there is no direct evidence for biliary excretion of these psychoactive drugs in man. Saturation or self-inhibition of its own metabolism is uncommon but is, however, probable with paroxetine.5,24,25
Optimally, the approximate time to safely restart psychoactive medications can be based on the plasma concentrations. Alternatively, the estimated initial concentrations following overdose can be based on the putative dose ingested, and reintroduction can be predicated on there being no prevailing adverse effects or contraindications (Figure 3). Once plasma concentrations have fallen to within the range of therapeutic levels (Table 3), the psychoactive drug can be restarted. This is particularly true for drugs with predictable linear elimination kinetics. However, in the instances of expected drug–drug interactions, particularly of inhibitory CYP interactions where the trend of plasma concentrations is difficult to predict, the use of drug concentration measurements is then highly beneficial to guide management, in addition to the standard-of-care clinical assessment.

Flowchart summarizing recommendations for restarting psychoactive medications following overdose.
Active metabolites, especially in high concentrations, should be considered and also be measured in plasma if it is known that they are important contributors to the effects of the drug (Tables 2 and 3; see section on Active metabolites below).
Active metabolites
Several antidepressants and antipsychotics have active metabolites (Tables 2 and 3). Where there are active metabolites, one should consider whether their concentrations and half-lives are similar or differ from those of the parent drug.
In several cases, the half-life of the active metabolite is longer than that of the parent. The combined effect in overdose may then considerably delay the recovery beyond that expected, given the half-life of the parent drug. For such drugs (e.g. venlafaxine, risperidone), the effective half-life of elimination is the half-life of the active metabolite. These ‘effective’ values are shown in Tables 2 and 3.
In some cases, the active metabolites are used per se. Examples of active metabolites used clinically and their parent drugs are: nortriptyline (amitriptyline), desipramine (imipramine) and desvenlafaxine (venlafaxine).
Lower plasma concentrations
It is expected that larger overdoses will produce very high plasma concentrations but, in some patients, plasma concentrations and drug effect for a given overdose are far lower than expected. There are several reasons for this:
(1) vomiting is common;
(2) intake in overdose may be ‘staggered’ over hours or even days, and the times patients report they took the drugs may be inaccurate;
(3) smoking or other drug–drug interaction induces the metabolism of some of these medications (see sections on Drug interaction and Smoking);
(4) prolonged presence of active metabolites may maintain pharmacological effects al-though parent drug concentrations are low;
(5) faster-than-average metabolism (see section on Elimination of overdose drugs, above).
Toxicokinetics
Half-lives and putative serum therapeutic and toxic ranges of medications of interest are important in the analysis of the clinical significance and time course of effects of overdoses of antidepressant and antipsychotic drugs (Tables 2 and 3). These factors were derived from the databases listed above and particularly from the review by Hiemke et al. 8
A good estimate of mean toxicokinetic parameters and their variations can be obtained after overdoses from timed plasma concentrations in 20 or more patients. Such estimates of mean parameters (e.g. half-lives) and variations have been obtained for several drugs, including citalopram, 15 escitalopram, 20 quetiapine,56,57 sertraline, 26 venlafaxine, 29 olanzapine 52 and clozapine. 47
Quite accurate determination of toxicokinetic parameters (half-life, clearance, etc.) can be obtained in an individual patient after the measurement of several timed plasma concentrations following an overdose. However, a further step is to use the prior estimates of half-life, clearance and volume of distribution and a limited number of blood samples from the patient to estimate their individual toxicokinetic parameters accurately using the techniques of population pharmacokinetics linked to Bayesian forecasting. When plasma concentrations have decreased well into the therapeutic range, dosage of the antidepressant or antipsychotic drug can be restarted, guided by the individualized toxicokinetic parameters estimated.
Toxic plasma concentrations and recommencement of antidepressant or antipsychotic dosage
Plasma concentrations associated with toxicity of most drugs are poorly documented. In this communication, we have referenced the consensus data listed by Hiemke et al. 8 They described a ‘laboratory alert level’ (Tables 2 and 3), a dangerously high plasma concentration ‘at or above which the therapeutic drug monitoring services laboratory should immediately inform the treating physician’.
The ‘laboratory alert level’ is often arbitrarily defined as twice the upper limit of the therapeutic range. 8 If plasma concentrations of the overdosed drug are available, then the time for a 50% decline in plasma concentrations (i.e. one mean t1/2) from the ‘laboratory alert level’ would decrease the plasma concentrations approximately to the upper level of the therapeutic range. It follows that one to two half-lives after attainment of ‘laboratory alert levels’ would be a reasonable time at which an antidepressant or antipsychotic drug could be recommenced.
Toxicology of antidepressants and antipsychotics
The toxicity of antidepressants and antipsychotics in overdose is very largely an extension of their therapeutic and adverse effects seen during therapeutic dosage. However, cardiovascular adverse effects are typically more severe or more common in overdoses than during therapeutic dosage. Sedation may also be greater after overdose than during therapeutic dosage. Serotonin toxicity and neuroleptic malignant syndrome (NMS) are serious, potentially life-threatening adverse effects that can occur with the use of antidepressant and neuroleptic (e.g. dopamine antagonist, antipsychotic) drugs, respectively.
Cardiovascular toxicity
Cardiac toxicity is one of the major concerns with many of these psychoactive drugs taken in overdose. 74 In particular, it is accepted that QRS widening in an electrocardiogram is an important predictor of serious arrhythmias, especially in the case of tricyclic antidepressant overdose. 75 Although the concerns of serious cardiotoxicity related to older antidepressants and antipsychotics have decreased with the advent of selective serotonin reuptake inhibitors (SSRIs) and atypical antipsychotics, there is still justified caution in overdose with these newer agents. Depending on the types of drugs ingested in the overdose, cardiac toxicity can be more pronounced in combination drug overdoses. Of the cardiac effects of the overdoses reviewed (Tables 2 and 3), tachycardia is the most common, followed by prolonged, corrected QT interval (QTc). Based on variable criteria which include improvement of overall clinical status, return to normocardia and improvement of QTc, patients are usually then deemed medically stable for discharge, transfer to psychiatric wards or safe recommencement of required psychoactive drug(s).
Serotonin toxicity and NMS
Serotonin toxicity can be characterized by altered mental state (e.g. agitation, delirium), autonomic hyperactivity (e.g. tachycardia, hypertension, fever), and neuromuscular abnormalities (e.g. tremor, clonus, hyperreflexia, rigidity) while NMS is characterized by altered mental state (e.g. agitated delirium), fever, muscle rigidity, and autonomic instability (e.g. tachycardia, labile blood pressure). These phenomena can occur idiosyncratically as a result of therapeutic use, drug–drug interaction, or in higher- or overdoses. 7 NMS has been reported in one case of overdose which developed within 1–2 days after an overdose of chlorpromazine and olanzapine. 76
Treatment of toxicity of psychoactive drugs
Discontinuation of the precipitating drug(s) is key, together with other general supportive management. Other measures include symptomatic drug treatment where appropriate for the patient’s condition. Examples include decontamination if appropriate (charcoal, gastric lavage), benzodiazepines or anticonvulsants for seizures and sedatives for psychomotor agitation. Appropriate cardiorespiratory support and cardiac monitoring is essential depending on the patient’s condition. Hypotension is common but treatment with vasopressors should be with caution due to potential complexities of alpha–beta effects in some overdoses. 77 Serotonin toxicity can be treated with benzodiazepines or with the serotonin antagonist cyproheptadine.6,78 NMS requires careful management, including fluid replacement, electrolyte or acid–base correction and active cooling. 79 Dopamine agonists such as bromocriptine and amantadine may be useful for more severe cases.7,79 Another drug treatment is dantrolene, a muscle relaxant that reduces muscle rigidity and metabolism, thereby reducing heat production. 79
Antidepressants
The toxicology of the five classes of antidepressants is important because of their current place in clinical use and implications in overdoses. Practically all antidepressants are metabolized hepatically by the CYP oxidizing enzymes (see section on Elimination and Table 2).
Tricyclic antidepressants (TCAs)
TCAs are toxic in overdose because of their potential for fatal arrhythmias (Table 2). The high affinity of TCAs for alpha1 receptors explains the orthostatic hypotension commonly associated with their overdose. 80 In addition, inhibition of cholinergic receptors by TCAs produces a varying degree of the anticholinergic adverse effects including blurred vision, dry mouth, urinary retention and constipation. More severe adverse effects may include sedation, impairment of memory and concentration, and delirium. Their powerful anticholinergic effect also slows gastric emptying and decreases intestinal motility. This leads to lower peak but more sustained plasma concentrations. 81 The anticholinergic actions may also decrease the peak concentrations and prolong the plasma concentrations of other drugs taken concurrently.
Selective serotonin-reuptake inhibitors (SSRIs)
The SSRIs are considered to be less toxic in overdose than the TCAs. 14 As the name indicates, SSRIs inhibit the neuronal reuptake of serotonin after its release within the central nervous system. Consequently, serotonin toxicity occurs in approximately 15% of overdoses of SSRIs.14,26 Blocking of serotonin reuptake by SSRIs may also lead to gastrointestinal adverse effects.
Selective serotonin–noradrenaline-reuptake inhibitors (SNRIs)
Overdoses of SNRIs are generally well tolerated, with symptoms including mild hypertension and tachycardia. Seizures have been reported with venlafaxine overdoses. 30 Cardiac toxicity with prolonged QTc is thought to occur more commonly in large overdose cases with venlafaxine.28,34
Tetracyclics
The toxicity of the commonly used tetracyclic, mirtazapine, following overdose is benign, with mild tachycardia, sedation and hypertension. 36 More severe toxicity can be seen in overdoses of mirtazapine in combination with other drugs, but this is dependent on the effects of other co-ingested drugs. 36 Deaths have been reported as a result of synergistic toxicity following combination drug overdose.82,83 The anticholinergic activity of mirtazapine is less than the tricyclics, but this effect may still slow its own rate of absorption or the absorption of other drugs.
Monoamine oxidase inhibitors (MAOIs)
Two metabolic classes of MAOIs have been used as antidepressants: irreversible inhibitor (e.g. phenelzine and tranylcypromine); and reversible competitive MAOI (e.g. moclobemide). They can produce toxicity when taken as a single overdose, but when taken in combination with other serotonergic drugs, can often produce serotonin toxicity.42,78 Important pharmacokinetic and pharmacodynamic interactions in the use of MAOIs include inhibitory effects on hepatic CYP enzymes, in particular, CYP2C19 and 2D6, and a tyramine-induced sympathomimetic response. 43 Therefore, dietary tyramine-containing food and indirect sympathomimetic drug restriction are important to prevent potentiated risks of tyramine reaction and hypertensive crisis. 84
The irreversible MAO inhibition means that function will only return once the enzymes are restored, while reversible MAO inhibition means that activity is restored as soon as the inhibitor dissociates from the MAO enzyme. 84 Irreversible inhibition of MAO may take several weeks and, consequently, any extension of therapeutic dosage of MAOIs or other antidepressants should be delayed. Similarly, reintroduction after overdose will require care.
Antipsychotics
Typical antipsychotics
Typical antipsychotics produce their major therapeutic effects through inhibition of dopamine D2 receptors which is accompanied by extrapyramidal adverse effects. 85 These effects may also occur after overdoses, but cardiovascular adverse effects are the major concerns of overdosage. These include hypotension, tachycardia and prolonged QTc. QT prolongation due to haloperidol is dose dependent; 7 however, this relationship was not observed with chlorpromazine. 44 Seizures are frequent and dose dependent; higher doses producing higher risk. 45
Atypical antipsychotics
Atypical antipsychotics have lower incidences of extrapyramidal adverse effects compared with the typical or conventional antipsychotics. Unlike typical antipsychotics, the atypical group have mixed affinities to D2 receptors and produce other adverse effects such as metabolic and cardiovascular disorders, 85 more commonly seen in chronic therapy.
Recommendations
As high plasma concentrations are likely for some time following an overdose, psychoactive medications are less likely to be restarted in an emergency or intensive care setting where the physical manifestations of the overdose are clearly obvious. Our recommendations include serial serum concentration estimations, including in some cases active metabolites, as standard practice, to facilitate clinical decisions.
Where serum concentrations are available, we suggest obtaining several samples in the initial period. For example, concentrations obtained at the time of, or at early presentation may document peak concentrations. Serial concentrations at various time intervals after presentation also can help document the time versus drug concentration trend(s). Having access to this data will be a useful guide to clinical management, particularly with respect to the optimal times for safely restarting medication and also for titration of drug doses after overdose.
If serum concentration measurements are unavailable, as illustrated in Figure 3, careful consideration of potential complex toxicokinetics and drug interactions is important to estimate the likely time to achieve safe drug concentrations ranges prior to recommencement of these psychoactive medications.
It is important to note that the resolution of some adverse effects following overdose may not occur concurrently with the achievement of serum concentrations within ‘safe or therapeutic’ ranges. In this instance, once the physical effects have almost or completely dissipated, the recommencement of psychoactive drugs (Figure 3) should still be modulated by the ongoing clinical evaluation and psychiatric need of each patient.
The common practice of restarting psychoactive drugs at a lower dose than was previously taken makes sense and up-titration should be slow in order to decrease adverse effects, in addition to other clinical considerations such as the previous therapeutic maintenance dose, comorbidities and other potential drug interactions. Where multiple psychoactive medications have been taken in overdose, it makes sense to restart the most clinically important drug first. Alternatively, the medication with the shortest half-life can be reintroduced first, as therapeutic concentrations will be reached sooner than those with longer half-lives.
When an alternative psychoactive drug is considered for commencement instead of the patient’s previous psychoactive treatment, important considerations would include the drug(s) ingested in the overdose event, the absence of contraindications to the new therapy, time to recovery from the overdose including acceptably low serum drug concentrations (if available), and the potential pharmacokinetic and -dynamic interactions with the new medication. Clinicians should also be guided by the relevant best-practice guidelines and the local psychiatric services expertise in the switching of antidepressant and antipsychotic drugs.
Conclusion and future directions
The limited experimental data on which our recommendations and comments are based raises many matters for future research and discussion. Patient outcomes based on recommendations should be investigated, including long-term outcomes in terms of mental health relapse rate, future overdoses and drug toxicity.
Genetic polymorphisms of the CYPs contribute to drug clearance, particularly for CYP2D6 and CYP2C19. Being able to identify fast or slow metabolizers of these cytochromes would be useful in overdoses involving their substrates. The influence of pharmacogenetics on medication clearance in overdose is an important research direction, especially as assays for variants of key CYP enzymes become more available.
We recognize that many hospitals do not have facilities for serum concentration measurements of these psychoactive drugs, and that this entails considerable expense that needs to be considered and justified. However, therapeutic drug monitoring is becoming more widely recommended in the adjustment of drug dosage of individual patients taking psychoactive medications. 8 With increasing numbers of hospital laboratories capable of conducting these assays and being expert in pharmacokinetics, particularly population pharmacokinetics, rapid measurement of plasma concentrations and pharmacokinetic analysis after overdose should become more standard practice.
Assays of many of the drugs discussed are inadequate because the assays are often of the total drug, that is, the total of the R- and S-enantiomers. As discussed previously, the pharmacokinetic parameters and pharmacological activities of the two isomers can be very different. Enantiomeric-specific assays of some drugs need to be facilitated.
We hope our review promotes discussion and action towards providing a reasonable evidence base and subsequent clinical pathways to guide practice in this challenging area.
Footnotes
Acknowledgements
We thank Neil Hardie and Priya Srikanthan of the NSW Medicines Information Centre, Darlinghurst, for their assistance in sourcing articles to enable completion of literature review.
Funding
Richard Day’s research is supported by National Health and Medical Research Council Programme Grant number APP 1054146.
Conflict of interest statement
The authors declare that there is no conflict of interest.