
Abstract
Background:
Hypernatraemia is a serious condition that can potentially become life threatening. It is known that lithium is associated with polyuria and nephrogenic diabetes insipidus, risk factors for hypernatraemia. In this study, we tested the hypothesis that lithium treatment was a risk factor for hypernatraemia.
Methods:
We performed a retrospective cohort study in the Swedish region of Norrbotten into the effects and potential adverse effects of lithium treatment and other mood stabilizers (LiSIE). For this particular study, we included all patients who had experienced at least one episode with a sodium concentration ⩾150 mmol/L between 1997 and 2013. Medical records were reviewed regarding past or current lithium exposure, diabetes insipidus and other potential risk factors for hypernatraemia.
Results:
Of 2463 patients included, 185 (7.5%) had experienced 204 episodes of hypernatraemia within the 17-year review period. In patients 65 years or older, infections dominated as the cause with 51%. In patients younger than 65 years, intoxications, particularly with alcohol, dominated as the cause with 35%. In the whole sample, dehydration accounted for 12% of episodes, 25% of which in the context of suspected or confirmed nephrogenic diabetes insipidus. Of all episodes, 25% resulted in death, with infection being the most common cause of death in 62% of cases.
Conclusions:
In our sample, infections and harmful use of substances including alcohol were the most common causes of hypernatraemia. Both current and past use of lithium also led to episodes of hypernatraemia, when associated with nephrogenic diabetes insipidus. Clinicians should remain vigilant, have a low threshold for checking sodium concentrations and consider even risk factors for hypernatraemia beyond lithium.
Keywords
Introduction
Lithium remains the first-line maintenance treatment for bipolar affective disorder (BPAD). 1 It is also used as augmentation of antidepressant medication and as a mood stabilizer in the treatment of schizoaffective disorder. Only recently has lithium been endorsed as superior in the prevention of suicide and severe affective episodes.2,3 Yet, despite its therapeutic superiority and versatility, adverse effects limit lithium use in clinical practice. Over half of all patients may discontinue lithium at some time, and adverse effects are the most common reason for discontinuation. 4
Lithium is associated with an increased risk of loss of renal function.5,6 Whereas glomerular damage appears only after years of lithium treatment, tubular dysfunction may emerge within weeks after lithium initiation. 7 Tubular dysfunction leads to urine concentration deficits and subsequently polyuria. Later on, this may progress to nephrogenic diabetes insipidus (NDI), 8 where tubular cells have lost their ability to respond to vasopressin [antidiuretic hormone (ADH)]. Up to 20–40% of patients treated with lithium may experience NDI.8,9 It remains unclear whether NDI is reversible once lithium has been stopped.
In the context of polyuria associated fluid imbalances and NDI, the risk of hypernatraemia may increase. Hypernatraemia occurs if more free water is lost than taken in. Hypernatraemia can develop into a serious or even life-threatening condition, if not treated quickly and appropriately. 10 Even mild hypernatraemia can be associated with increased morbidity and mortality. 11 Hypernatraemia can initially present with many unspecific symptoms, such as lethargy, weakness and irritability. Symptoms can then progress to muscle twitching, seizures and coma. 12 Hence, the condition can be easily missed, unless a blood test is taken. For instance, clinicians may mistake hypernatraemia-associated changes in mental status for signs of psychiatric deterioration. Other symptoms, such as dry mouth, hypertension or oedema can occur in the context of many psychotropic medications and not just lithium. Thus, for mental health professionals, it is important to be aware of hypernatraemia and identify factors that can increase the risk.13,14
The aims of this study were (1) to determine the frequency of hypernatraemia episodes, (2) to assess the potential association with past and present lithium exposure and (3) to evaluate the fatality rate of hypernatraemia episodes.
Procedure
We collected the data as part of a retrospective cohort study (LiSIE) into the side effects and effects of lithium treatment as compared with other mood stabilizers for the maintenance treatment of affective disorders. The Regional Ethics Review Board at Umeå University, Sweden, approved this study (DNR 2010-227-31M, DNR 2011-228-32M, DNR 2014-10-32M). Participants provided informed verbal consent. In accordance with the ethics approval granted, no consent was obtained for deceased patients. We have summarized the whole method in a Strobe checklist (Appendix 1 in the supplemental material).
Participants
For LiSIE, we identified all patients in the Swedish region of Norrbotten, who were at least 18 years of age and who had been either diagnosed with BPAD (F31) or schizoaffective disorder (F25) irrespective of mood stabilizer use. We also included patients who had been prescribed lithium as a mood stabilizer for other affective disorders. We considered all patients who had consented, or who we were approved to include because they had deceased. The study covered a 17-year period from 1997 to 2013. For this particular study, we included all patients who had experienced at least one episode with a sodium concentration ⩾150 mmol/L as identified in our central laboratory database, where all sodium concentrations were stored. We then reviewed the medical record of all eligible patients and systematically abstracted all data obtained into a database.
Variable definitions
Hypernatraemia
We considered hypernatraemia to be clinically significant when it was at least moderate with a serum sodium concentration of at least 150 mmol/L. 15 For each episode, we determined whether the hypernatraemia was an isolated incident or persistent: hypernatraemia was defined as an isolated incident if sodium concentrations had been normal within 3 months prior to the current episode or persistent if abnormal concentrations had existed for more than 3 months prior to the current hypernatraemia episode.
Cause of hypernatraemia
For each episode, we elicited the main cause of clinically significant hypernatraemia as recorded in the case records. This was our main outcome variable. Causes were divided into cerebrovascular diseases, cardiovascular failure, dehydration, NDI, infection, inflammation, harmful use of alcohol or substances, lithium intoxication, medication, malignancy, hyperglycaemia, renal failure, other or unknown. All episodes were also evaluated for sex, age, treatment provider, underlying mental health problem, treatment, nonpsychiatric comorbidities, surgery, neurologic symptoms, use and length of lithium treatment, laboratory results and outcome of the hypernatraemia episode. As a secondary outcome variable, we examined the fatality rate associated with the hypernatraemia episodes identified.
Lithium exposure
For each hypernatraemia episode, we checked whether the patient had been treated with lithium currently or in the past. Lithium exposure was determined by the presence of at least one blood lithium concentration >0.2 mmol/L recorded in our central laboratory database.
NDI
We also evaluated NDI as a major contributing factor for hypernatraemia. Here, we considered both confirmed and suspected NDI. NDI was considered confirmed when either the diagnosis had been established or urine osmolality was inadequately low in relation to plasma osmolality or suspected when polyuria and/or polydipsia (polyuria–polydipsia complex) was explicitly recorded in the medical records.
Control for bias
In accordance with the ethical approval granted, we controlled for selection bias in the whole retrospective cohort study, comparing age, sex, maximum recorded lithium and creatinine concentrations as key parameters, available in anonymized form. We did not find any difference between participating and nonparticipating patients.
Data collection and analysis
The clinical information was abstracted and rated by two investigators, a specialist in general practice and senior trainee doctor in psychiatry (BF) and/or a consultant physician and specialist in internal medicine and nephrology (MO). All data was anonymized before analysis. We first analysed the data descriptively. We compared episodes of hypernatraemia stratified by age and lithium treatment status, using χ2 test. We assessed the correlation between hypernatraemia and age by linear regression.
We evaluated risk factors for fatal outcome by univariate analysis. To account for potential confounders, we then conducted a logistic regression analysis, entering variables in a stepwise backward fashion. For all analyses, differences were considered statistically significant with a p value of ⩽ 0.05. We used Microsoft Excel 2010 version 14.0 (Microsoft, Redmond, WA, USA) and Statistical Package for the Social Sciences, SPSS 18.0 (SPSS Inc., Chicago, IL, USA).
Results
For this study, 3735 patients were potentially eligible. Of these, we could include 2596 patients according to our consent procedures. Sodium concentrations were available for 2463 patients. Of these, 185 (7.5%) patients had experienced sodium concentrations of ⩾150 mmol/L on at least one occasion during the 17 years of review (Figure 1). For these patients, we identified 204 episodes of hypernatraemia. A total of 11 (5.9%) patients had more than one episode of hypernatraemia. Four patients had three or more episodes.

Selection of study sample.
Sample characteristics
Men and women accounted for approximately the same number of episodes. The mean age per episode was 63.4 [standard deviation (SD) 18.9] and the median 69 years. The age ranged from 19 to 93 years. A total of 59% of episodes related to patients aged 65 years or older. In 42% of episodes, patients had been exposed to lithium at some point, either currently (28%) or in the past (14%) (Table 1).
Baseline characteristics.

Data completeness
For the main outcome variable concerning the cause of hypernatraemia, data was missing for 8% of episodes. There was no significant difference regarding age and sex between episodes with available and missing data. For the secondary outcome, fatality associated with the hypernatraemia episode, the data was complete.
Features of the hypernatraemia episodes
The vast majority of episodes were detected during treatment in a medical or surgical hospital facility. Only 11% were diagnosed in a psychiatric setting. The mean highest sodium concentration was 157.4 (SD 8.5) mmol/L with a median of 154 mmol/L. A total of 12% of episodes had sodium concentrations of 170 mmol/L or more (Table 2). The highest sodium concentration recorded was 186 mmol/L. The highest sodium concentrations measured correlated significantly with age (p < 0.01) (Figure 2).
Factors that may increase risk of death in the context of hypernatremia.

p < 0.05; **p < 0.01.
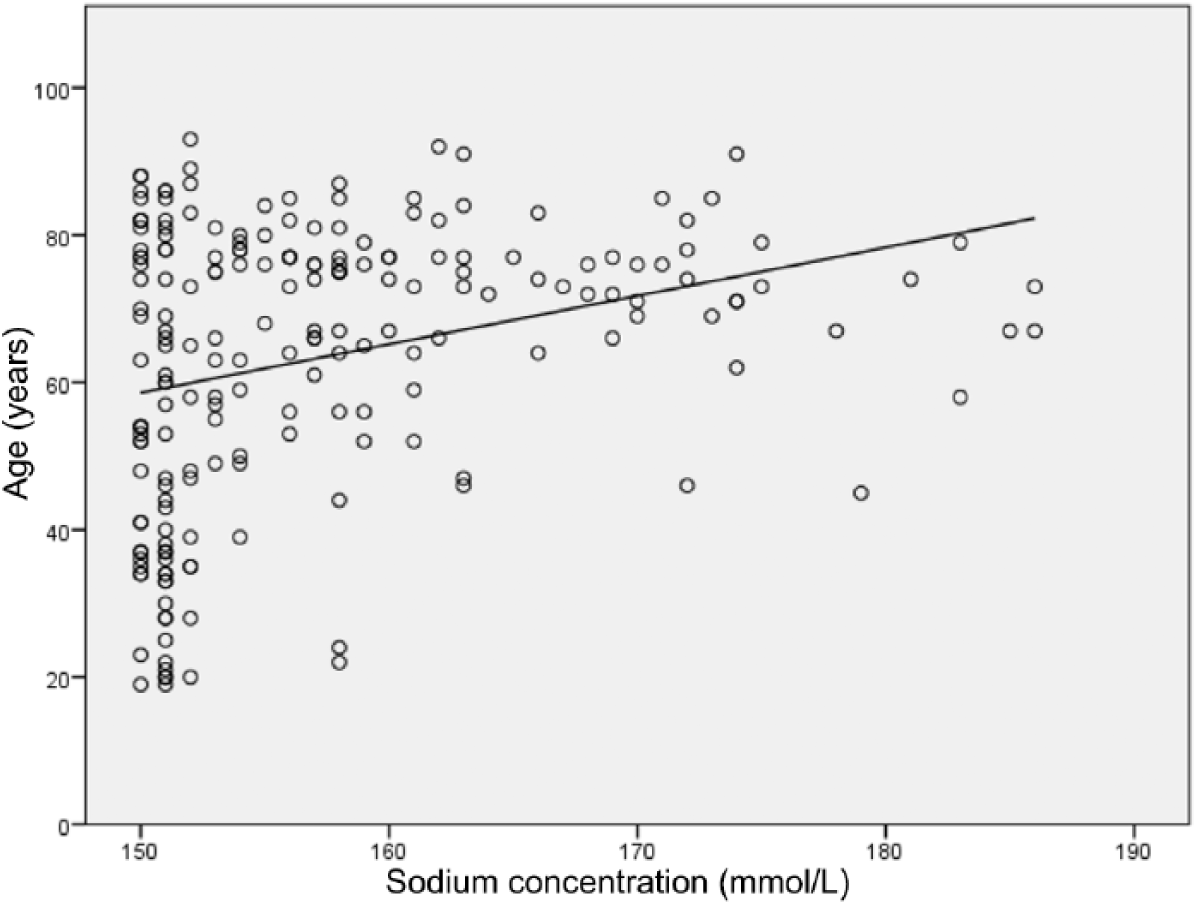
Relationship between age and highest sodium concentration.
Causes for hypernatraemia
For 92% of episodes, we could establish the cause of hypernatraemia from the medical records. For the whole sample of 204 episodes, infection was the dominating cause, accounting for 37% of all episodes. Intoxications other than lithium came second with 15%. Dehydration accounted for 12% of episodes, 25% of which had occurred in the context of suspected or confirmed NDI. Lithium intoxications only accounted for 1% of all the hypernatraemia episodes.
Causes of hypernatraemia according to age
In patients aged 65 years or older, infections dominated with 51% of all episodes. Dehydration accounted for 10% and suspected or confirmed NDI for 3% of episodes. Intoxications were negligible. However, in patients younger than 65 years, intoxications were the most common cause of hypernatraemia with 35% of all episodes. In this group, 77% of intoxications involved alcohol, either on its own or in combination with tablets. Infection came second with 18.4%. Dehydration accounted for 7% and suspected or confirmed NDI for 4% of episodes (Figure 3).
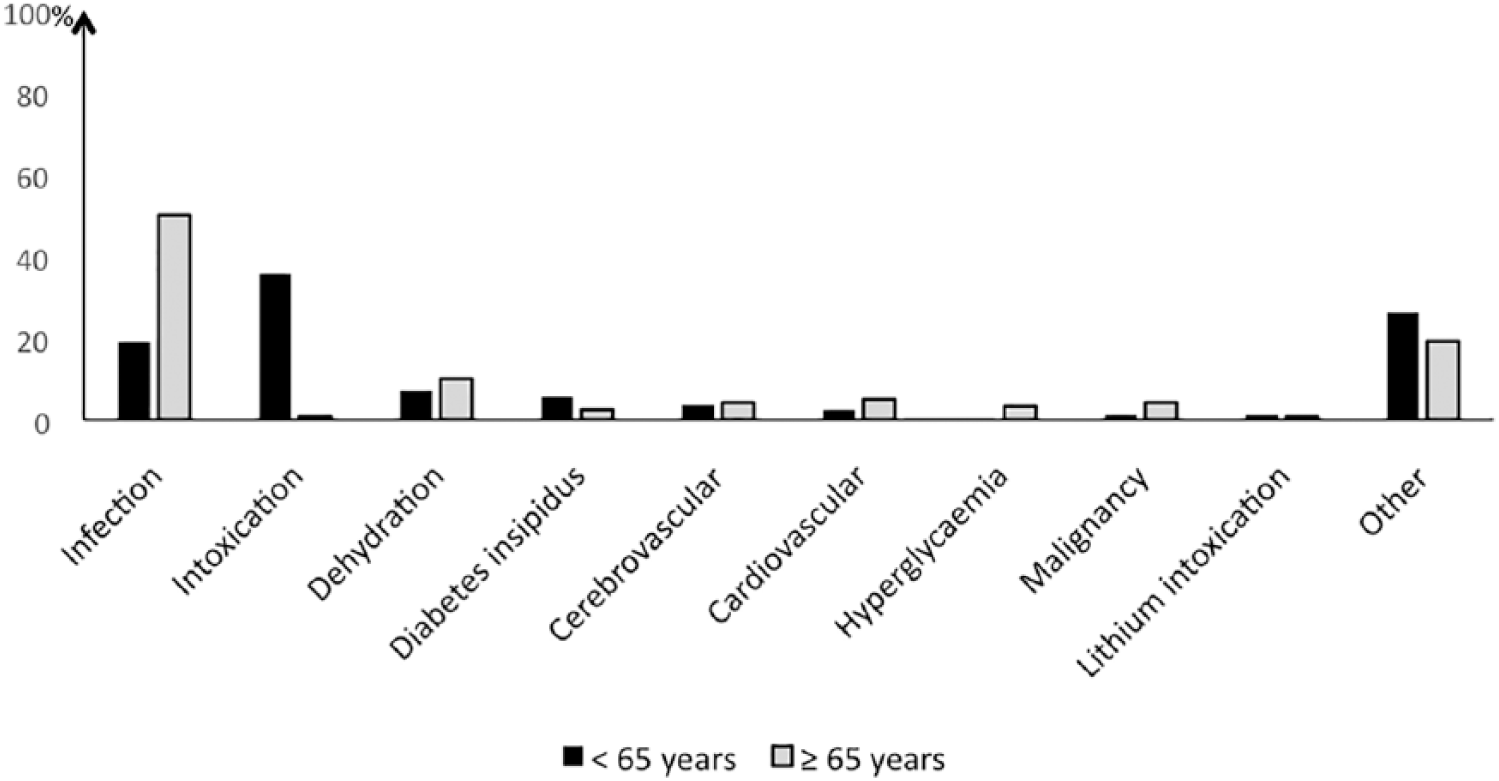
Causes of hypernatraemia according to age at episode.
Lithium exposure and NDI
For 6 of the 204 episodes, NDI was explicitly diagnosed and recorded in the patients’ journals. However, based on the information found in the patients’ records, NDI was suspected in 27 further episodes. Thus, even if not considered the main cause, NDI or substantial polyuria had been present in 16% of all hypernatraemia episodes. A total of 35.1% of hypernatraemia episodes occurred in the context of current lithium treatment were associated with suspected or confirmed NDI. In the context of past lithium treatment, 25.9% episodes were also associated with suspected or confirmed NDI. However, only 5% episodes occurring in patients never exposed to lithium were associated with suspected or confirmed NDI. Episodes with confirmed or suspected NDI were significantly associated with current lithium exposure compared with no lithium exposure ever (odds ratio (OR) = 10.3; 95% confidence interval (CI): 3.8–27.5, p < 0.01). Episodes with confirmed or suspected NDI were still associated with past lithium exposure compared with no lithium exposure ever (OR = 6.7; CI: 2.0–21.8, p < 0.01). The odds of having an episode with confirmed or suspected NDI were nine times greater for lithium exposure ⩾5 years compared with lithium exposure <5 years (OR = 9.4; CI: 1.2–75.4, p < 0.05).
Persistence of hypernatraemia
In 86.8% of all episodes, the hypernatraemia was an isolated incident. The hypernatraemia was persistent in 13.2% of all episodes. Hypernatraemia was persistent in two-thirds of episodes associated with definite or suspected NDI.
Fatality
A total of 50 (25%) episodes resulted in death. The leading cause of death was infections with 62%. Confirmed or suspected NDI accounted for 12% of all deaths. There were many potential risk factors for a fatal outcome. On univariate analysis, in which each risk factor was assessed on its own merit, older age and residential care were significantly associated with death (Table 2).
On stepwise logistic regression, age remained the only variable significantly associated with death. Individuals 65 years or older were more likely to die of hypernatraemia than individuals aged 65 years or less (OR = 4.1; CI: 1.9–9.2; p < 0.01). Severity of hypernatraemia was not associated with death. Residence lost its significance in the multivariate model, because older people were more likely in residential facilities.
Discussion
Whereas sodium gain is a possible cause in different iatrogenic settings, deficit of free water is the main reason for hypernatraemia in general. Impaired water intake, water losses or a combination thereof often lie behind high serum sodium concentrations. Apart from the apparent causes of dehydration, such as gastroenteritis or fever, medicines often are the reason that water is lost. Diuretics are widely used, but water losses even may occur through acquired diabetes insipidus, both central and renal (Table 3).

Episodes of hypernatraemia occur in the context of lithium exposure, but infections and harmful use of substances including alcohol were more common. Of all psychotropic medicines, lithium is most likely to lead to polyuria and NDI, main risk factors for hypernatraemia. One study in 55 elderly patients found a lithium-associated hypernatraemia of ⩾150 mmol/L in 11%. In this study, the hypernatraemia risk was 3% in patients who were treated concurrently with antidepressants and 25% in patients who were not. 16 However, at population level, other reasons for hypernatraemia may be much more common. In our study, infections were the main reason for hypernatraemia in older patients. Intoxications, particularly those involving alcohol, were the main reason for hypernatraemia in younger patients.
Assessing the risk of hypernatraemia in patients with severe affective disorders
Mental health professionals need to bear in mind that although lithium treatment is a ‘classical’ risk factor for dehydration, there are other risk factors as well. Thus, hypernatraemia should be excluded as a differential diagnosis in any patient experiencing an unexpected mental status change. In particular, older patients may be at risk. 16 Psychiatrists working in acute or addiction services may encounter hypernatraemia in patients presenting acutely intoxicated. Psychiatrists working in liaison settings are likely to see hypernatraemia in a variety of medical conditions. Our findings suggest that clinicians should be particularly vigilant in the context of infections. We also recommend careful review of the medical chart since there are several agents apart from lithium that can raise sodium concentrations7,10 (Table 3). Acute hypernatraemia can present with dramatic symptoms, such as lethargy, seizures, weakness, irritability and coma. Persistent hypernatraemia states may present with much fewer symptoms if any. 17 This can make persistent hypernatraemia difficult to diagnose and justifies a low threshold for requesting sodium concentrations.
Alcohol intoxication and the risk of hypernatraemia
In our study, acute alcohol intoxication was the most common cause for hypernatraemia in patients younger than 65 years old. These findings are in line with other,10,18,19 although estimates vary widely. In an Austrian study of 161 patients admitted for acute alcohol intoxication to the emergency department, 41% patients had sodium concentrations >145 mmol/L. 19 In a Finnish study of 196 patients treated for acute alcohol intoxication, hypernatraemia was present in 15% patients. 18 Alcohol associated hypernatraemia occurs secondary to alcohol induced polyuria. The reasons why alcohol induces polyuria are still not fully understood. However, alcohol can reduce vasopressin secretion from the posterior pituitary gland, 20 causing central diabetes insipidus.
Assessing the risk of hypernatraemia in patients with current or past lithium exposure
Polyuria and polydipsia are common adverse effects of lithium treatment. 4 NDI with polyuria as primary disturbance occurs when the distal renal tubular cells become impaired in their ability to respond to vasopressin and reuptake water through aquaporines. 8 Estimates for the prevalence of polyuria and renal diabetes insipidus vary widely. Up to 70% patients treated with lithium may experience urine concentration deficits. 21 Up to 40% may experience NDI. 8 Hypernatraemia can occur, when patients with lithium treatment have developed urine concentration deficits and lose more water than they actually take in. For instance, this can happen in the context of an acute infection, surgical interventions, excessive sweating when changing to a warmer climate or increased concentrations of exercise. It still remains unclear how far NDI is reversible once lithium has been discontinued. This question has not been investigated in recent years. NDI reversibility may depend on length of treatment. Long-term lithium treatment may render NDI irreversible.7,22 However, it remains less clear what happens after intermediate lithium exposure. Grandjean et al. 22 suggest that NDI is ‘usually’ reversible after lithium treatment up to 6 years. Garofeanu et al. 7 pooled data from several studies of patients who had been treated with lithium for a mean of 8 years and who had developed NDI. In 5% of all cases, NDI was reversible and in 25% partially reversible. In the remaining 70% cases, NDI persisted. Our study also suggests that lithium associated NDI may not be reversible in all cases. We found hypernatraemia episodes with confirmed or suspected NDI not only associated with current but also with past lithium use. We could also endorse a time trend: length of lithium exposure increased the likelihood of suspected or definite NDI. Despite a high prevalence of NDI in patients taking lithium, tubular function is not routinely assessed in clinical practice. Checking urine osmolality, plasma osmolality and daily urine output could improve the detection rate of NDI, thereby reducing a lithium-specific risk factor for hypernatraemia.
Lithium intoxication
As dehydration leads to prerenal impairment of the kidney function, we had expected to find an association between hypernatraemia episodes and lithium intoxications. However, in our study, there were only two patients in whom lithium intoxication was thought to have caused the hypernatraemia episodes. This ties in with our previous study of 91 episodes of severe lithium intoxications in the same cohort, in which only one patient was found to have a high sodium concentration. 13 As the symptom of lithium intoxication and hypernatraemia overlap, we recommend taking both lithium and sodium concentrations when faced with unexpected mental and somatic status changes.
Fatality rate associated with hypernatraemia
Recognising hypernatraemia early is important because it carries substantial mortality. In our study, 25% of hypernatraemia episodes resulted in death. After adjusting for confounders, age was the only significant risk factor for a fatal outcome. There was no difference in fatality rate in patients who were taking lithium at the time of the hypernatraemia episodes and those who were not. A survey of 256 patients presenting to an emergency department with sodium concentrations >160 mmol/L found an even higher fatality risk; about half of all patients died. In this study, patients had a mean age of 74 years. 23 In intensive care, fatality rates between 30% and 50% are reported. 24 This confirms the importance of proactively taking sodium concentrations in patients who present acutely to psychiatric emergency departments.
Strength
As we had access to medical records over a period of 17 years, we could conduct a comprehensive in-depth assessment of the clinical data, laboratory findings and clinical outcome to determine the cause of the hypernatraemia. Access to medical records allowed validation of clinical data beyond what is possible in register studies. A further strength was the high rate of consent for participation into the study. As age and sex distribution of consenting or not consenting patients was similar, the likelihood of selection bias was low. To the best of the authors’ knowledge, this is the largest study ever conducted on this topic.
Limitations
LiSIE was designed to provide an in-depth analysis of clinical records to avoid association bias that can occur with nonvalidated data from register studies. LiSIE was also designed to focus on rare but potentially dangerous adverse effects of lithium treatment. To increase the sample of patients with current or past lithium exposure, we not only included patients with BPAD or schizoaffective disorder, but also depressed patients treated with lithium. For patients with BPAD or schizoaffective disorder, we included both patients having and not having been exposed to lithium. For patients with depression, we did not include a control group of patients without lithium treatment, because recruiting all other depressed patient in our catchment area would not have been practically feasible. As this may lead to an overestimation of lithium associated adverse effects, we have not reported incidence figures here. Instead the starting point of this study was hypernatraemia episodes, which were then analysed in detail.
There were only 15 urine osmolality samples and no plasma osmolality samples available. Thus, diagnosis of suspected NDI had to rely solely on the documentation of polyuria–polydipsia complex in the medical records. Patients with psychogenic polydipsia or excessive fluid intake due to xerostomia can also present with a polyuria–polydipsia complex, clinically indistinguishable from NDI. This may have led to an overestimation of the NDI prevalence. In NDI, polydipsia is a consequence of polyuria. Primary polydipsia, for instance psychogenic polydipsia, however, usually leads to hyponatremia and is unlikely to cause hypernatraemia.
There may have been concomitant treatments modifying the risk of hypernatraemia. For instance, diuretics may lead to dehydration and increase the risk of hypernatraemia. Antidepressants on the other hand, for example, selective serotonin reuptake inhibitors (SSRI) and tricyclic antidepressants (TCA), may decrease the risk of hypernatraemia through inappropriately increased vasopressin secretion (SIADH). 16 We could not assess the use of fluid management, because this was only reported inconsistently.
Conclusion
In our study, infections and harmful use of substances including alcohol were the most common causes of hypernatraemia. Both conditions increase the risk of water depletion. Water depletion may occur more quickly in the context of NDI. Lithium use is associated with an increased risk of NDI. Clinicians should remain vigilant, have a low threshold for checking sodium concentrations, and consider even risk factors for hypernatraemia beyond lithium. Patients treated with lithium should be educated about diabetes insipidus, the risk of hypernatraemia and the importance of adequate fluid intake.
Supplemental Material
Appendix_1_STROBE_Statement – Supplemental material for Lithium treatment, nephrogenic diabetes insipidus and the risk of hypernatraemia: a retrospective cohort study
Supplemental material, Appendix_1_STROBE_Statement for Lithium treatment, nephrogenic diabetes insipidus and the risk of hypernatraemia: a retrospective cohort study by Michael Ott, Björn Forssén and Ursula Werneke in Therapeutic Advances in Psychopharmacology
Footnotes
Funding
This work was supported by a grant of the Research & Development Fund of Norrbotten Region, Research and Innovation Unit, Sweden.
Conflict of interest statement
Michael Ott has been a scientific advisory board member of Astra Zeneca Sweden, 2018.
Björn Forssén declares that there is no conflict of interest.
Ursula Werneke has received funding for educational activities on behalf of Norrbotten Region (Masterclass Psychiatry Programme 2014–2018 and EAPM 2016, Luleå, Sweden): Astra Zeneca, Eli Lilly, Janssen, Novartis, Otsuka/Lundbeck, Servier, Shire and Sunovion.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.