
Abstract
Background:
Black people are over represented in mental health services and prescribing of antipsychotics differs by race in some countries. Our previous UK research into the prescribing of antipsychotics in large, multicentre studies found no important differences for black and white patients. However, we received several comments challenging our findings. We wanted to test the validity of these anecdotes by devising two case vignettes that differed only by race and asking prescribers to choose antipsychotic treatment.
Method:
A case study was sent to all medical prescribers in the South London and Maudsley NHS Trust. Half of the prescribers for each grade of staff were sent the case study where the ethnicity of the patient was white and the other half where the ethnicity was black. Participants were asked to describe what they would prescribe for the patient. Outcomes were total percentage maximum dose, high dose, type of antipsychotic, route of administration and antipsychotic polypharmacy.
Results:
We received 123 completed case studies and demographic data forms from prescribers. There were no differences in percentage maximum dose, high dose, type, route and number of antipsychotics prescribed by case study ethnicity.
Conclusions:
Prescribing for UK black and white patients is broadly similar when tested in clinical and theoretical studies.
Introduction
Black people are over represented in mental health services [Care Quality Commission, 2010] and they are more likely to be admitted and detained than their white counterparts [Morgan et al. 2006; Care Quality Commission, 2010]. In addition, deaths of black service users [Norfolk, Suffolk and Cambridgeshire Strategic Health Authority, 2003] have resulted in accusations of institutional racism in UK mental health services [McKenzie and Bhui, 2007]. The implication is that this racism is reflected in different prescribing practices for black people.
Prescribing of antipsychotics differs by race in some countries. Studies, mostly in the United States, show black patients are more likely to receive higher doses, typical antipsychotic agents and greater numbers of antipsychotics than white patients [Diaz and De Leon, 2002; Kreyenbuhl et al. 2003; Taylor, 2004]. However, several UK studies have not shown major differences in prescribing quality between black and white patients [Connolly et al. 2007, 2011; Connolly and Taylor, 2008]. Previously we examined dose, type, polypharmacy and costs of antipsychotics in large, multicentre studies. There were no important differences between treatments for black and white patients. Possible reasons for this difference in findings from US studies include a more equitable healthcare system in the UK, a diverse multicultural mental health workforce [Goldacre et al. 2004] and changing attitudes to racism.
After publication of our studies examining antipsychotic prescribing in black and white patients, we received several comments challenging our findings. Black and minority ethnic group prescribers reported disbelief at our results. They claimed that black patients have a longer duration of untreated psychosis (a suggestion disproved in the UK by the AESOP study [Morgan et al. 2006]) and a greater illness severity (a potentially confounding factor not accounted for in our previous study) on admission [Arnold et al. 2004]. Because of these differences, prescribers told us, they purposefully prescribed larger doses for black patients.
We wanted to test the validity of these anecdotes in a formal way in a wider population of prescribers at one centre from our original study [Connolly et al. 2011]. We did this by devising two case vignettes that differed only by race and asking prescribers to choose antipsychotic treatment(s) and dose(s).
Method
A case study (see Appendix 1), demographic data form (collecting age, gender, grade of staff and prescriber ethnicity) and explanatory letter were sent to all medical prescribers in the South London and Maudsley NHS Trust. Half of the prescribers for each grade of staff were sent the case study where the ethnicity of the patient was white and the other half where the ethnicity was black. Respondents could reply by email or anonymously in the post. Prescribers who did not respond were sent a reminder email after 2 weeks.
The case study asked two questions: what antipsychotic(s) would you prescribe for this patient and what dose(s) would you use? The explanatory letter asked prescribers to complete a survey of antipsychotic prescribing. It stated that the reasons for the study could not be revealed as they would invalidate the results. The case study was piloted before distribution to ensure it was fit for purpose and could be easily completed. Study permission was obtained from the South London and Maudsley NHS Trust Drugs and Therapeutics Committee.
Statistical analysis
The outcomes analysed were: total percentage maximum dose (calculated as dose divided by maximum British National Formulary (BNF) dose [BMJ Group and Pharmaceutical Press, 2014], multiplied by 100); high dose (more than 100% of BNF maximum dose); type of antipsychotic (typical or atypical); route of administration (oral or intramuscular); and antipsychotic polypharmacy (being prescribed more than one antipsychotic). Descriptive statistics were calculated for prescribers’ demographic data and inferential statistics were used for each outcome by case ethnicity. In addition relationships between outcomes and prescriber demographic data were explored using inferential statistics, i.e. t-test and analysis of variance (ANOVA) for continuous and chi-squared for categorical outcomes. Continuous variables were transformed when lacking normality and categorized where appropriate to ease interpretation. All analyses were performed using IBM SPSS software.
Results
Study population
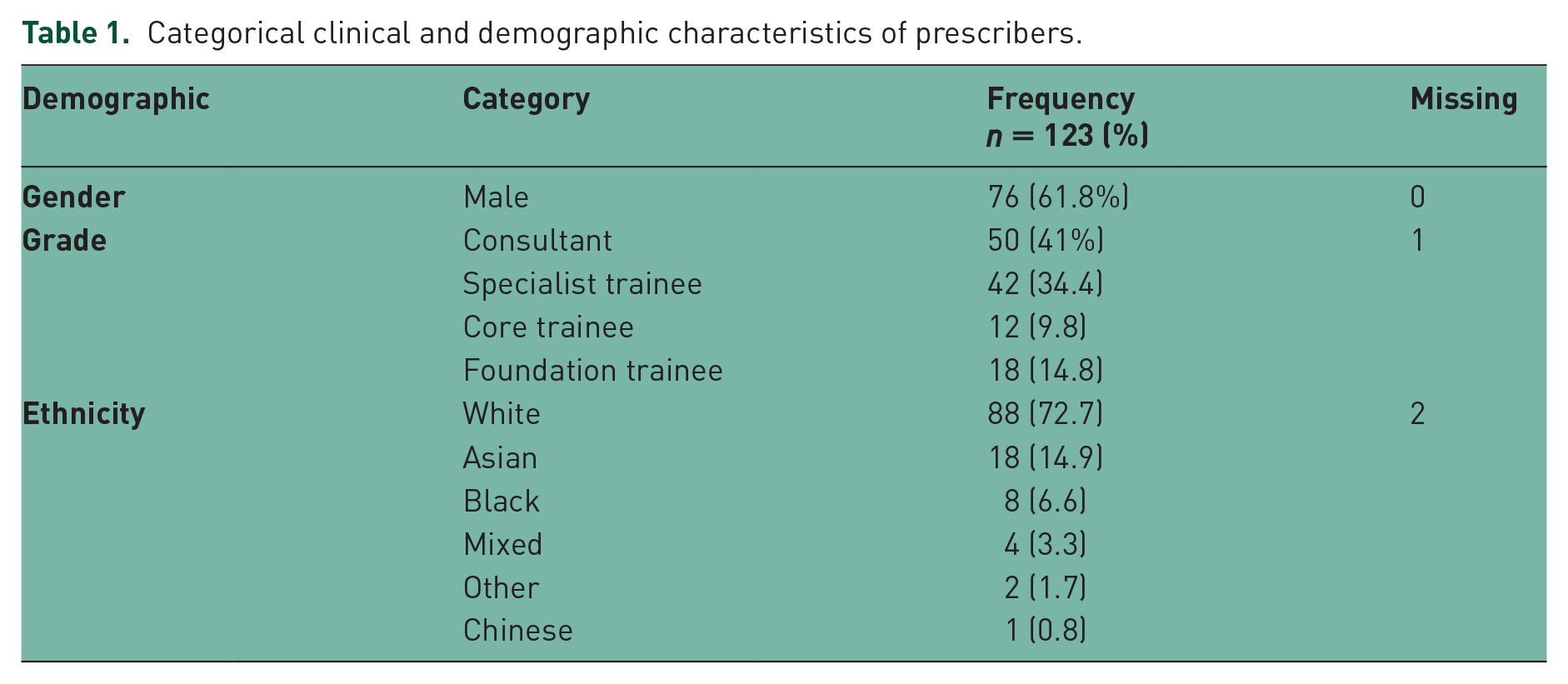
We sent 784 case vignettes and demographic data forms to prescribers. Of these, 123 (15.7%) were completed and returned. Clinical and demographic characteristics of prescribers are detailed in Table 1. The mean age of the prescribers (n = 115) was 39.1 years (range 25–63). A total of 63 (51.2%) of the returned case vignettes were those where the patient was described as white.
Categorical clinical and demographic characteristics of prescribers.
Outcomes
Descriptive data for each of the categorical outcomes (high dose, type, polypharmacy and route) are listed in Table 2.
Categorical outcomes of case vignette.
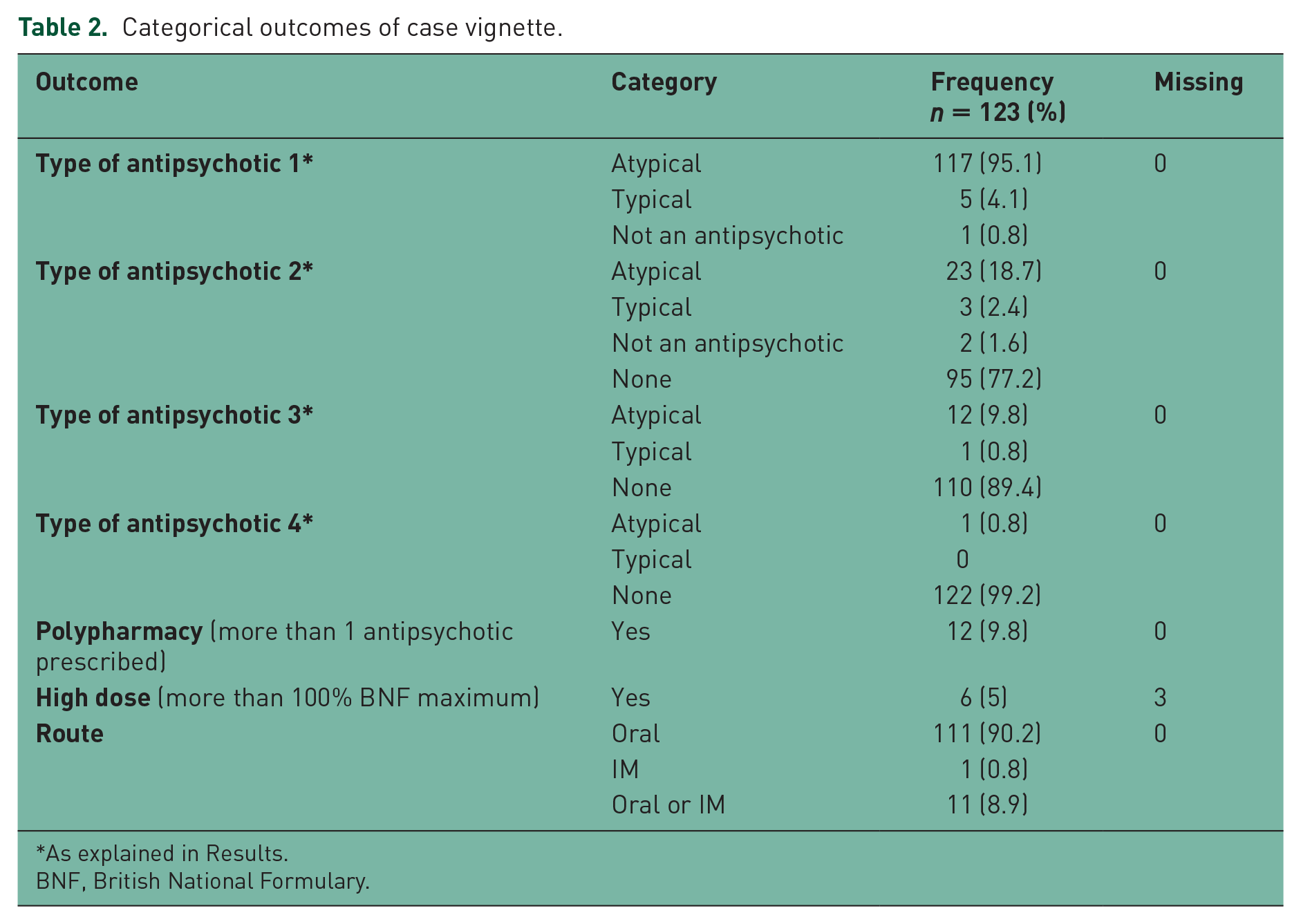
As explained in Results.
BNF, British National Formulary.
Total dose (percentage maximum dose)
There was no significant difference in total dose of antipsychotic by case ethnicity (p = 0.567) (see Table 3). The mean total doses for black and white patients were 47.7% and 50.9%, respectively (Figure 1).
Total dose and case ethnicity.
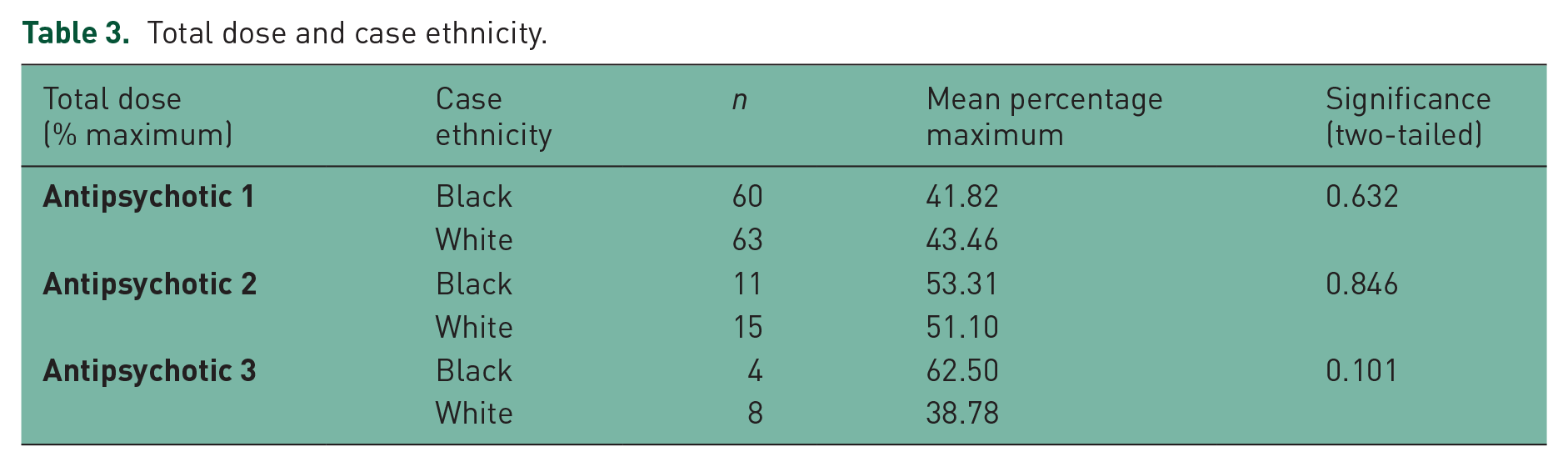

Total dose (percentage maximum) by case ethnicity.#
Type of antipsychotic
Aripiprazole then olanzapine were the most frequently chosen antipsychotics accounting for 82.1% of choices (Figure 2). Prescribers often gave several possible treatment options in reply to the case vignette questions, for example, olanzapine or aripiprazole or quetiapine or risperidone. These were labelled in the order written as antipsychotic 1 or antipsychotic 2 or antipsychotic 3 or antipsychotic 4. There was no difference by case vignette ethnicity in type (typical or atypical) of antipsychotic 1 (Figure 3), antipsychotic 2, antipsychotic 3 or antipsychotic 4.
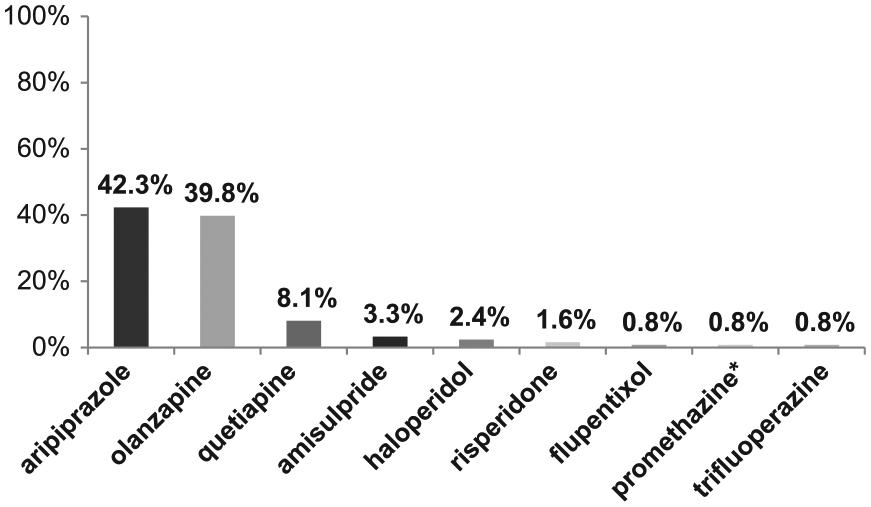
Choice of antipsychotic by case ethnicity.

Type of antipsychotic by case ethnicity.
Antipsychotic polypharmacy, high dose, route of ad-ministration outcomes
There were no differences in antipsychotic polypharmacy (p = 0.365, Figure 4), high dose prescribing (p = 0.680, Figure 5) and route of administration (p = 0.531, Figure 6) by case ethnicity.

Polypharmacy (more than one antipsychotic prescribed) by case ethnicity.

High-dose antipsychotic (more than 100% BNF maximum dose) by case ethnicity.

Route of antipsychotic by case ethnicity.
Prescriber variables and outcomes
Each prescriber variable (age, gender, grade of staff and ethnicity) was examined to determine whether associated with our outcomes (total dose, high dose, polypharmacy, type and route).
Total dose
Age was not normally distributed but three discreet categories were evident. These three categories were: 32 years old or less, 33–44 years old and 45 years old or more. Mid-aged (33–44 year olds) prescribers were more likely to use higher doses (p = 0.01). Gender, grade of staff and prescriber ethnicity were not significantly associated with total dose.
High dose
As with total dose, mid-aged prescribers were more likely to prescribe high doses (p = 0.04). Gender, grade and prescriber ethnicity were not significantly associated with high dose.
Polypharmacy
Mid-aged prescribers were more likely to prescribe more than one antipsychotic concurrently (p = 0.001). Gender, grade and prescriber ethnicity were not significantly associated with polypharmacy.
Type and route
We found no association between any prescriber variables for type and route outcomes.
Discussion
Main findings
We found no difference in antipsychotic prescribing by ethnicity when examined using a case vignette method. This included analysis of total dose, high dose, polypharmacy, type and route of antipsychotics chosen. In addition prescriber variables, with one exception, were not associated with any of our outcomes.
Comparison with previous studies
A similar method to that used in this study has been used previously to test differences by race in the treatment of patients with mental health problems. The study of British psychiatrists [Lewis et al. 1990] used a case vignette, differing by race (black or white) and gender, to determine effects of these variables on treatment. Inter-estingly they found that psychiatrists rated white patients as significantly more likely than black to need ‘neuroleptic treatment’. In addition to this they also found no differences by race in ‘antidepressant treatment not indicated’ and ‘unlikely to comply’. This study was revisited in 2001 by Minnis and colleagues [Minnis et al. 2001]. Again they used a case vignette but also attached a photograph of a white or black man. Similarly, these later authors also found that white patients were more likely than black to have ‘neuroleptic drug treatment indicated’. Thus, as in this study, prior case-based questionnaires did not find black patients were more likely to receive antipsychotics.
Limitations
We had a poor questionnaire return rate compared with previous studies. This may be because the vignettes were emailed and so could be easily ignored as prescribers receive large volumes of unsolicited email. A reminder was sent out, again by email, and did improve response rates.
Poor return rates may also have been because prescribers guessed the reasons for our study. Other studies [Lewis et al. 1990; Minnis et al. 2001] did not ask for prescribers’ ethnicity directly as we did. This was because they were concerned that this would unmask their studies. Instead they collected indirect indicators of ethnicity, i.e. medical school of graduation; however, some of their respondents still guessed correctly. We cannot be sure if any of our prescribers knew, or whether or not some were suspicious. No prescribers we spoke to guessed correctly the purpose of the study, but many were concerned that the case vignette was for a ‘prescribing test’ set by our Trust and that there were ‘correct answers’.
Conclusion
Our original conclusions about antipsychotic prescribing quality and ethnicity are supported by the results of this study. Prescribing for UK black and white patients is broadly similar when tested in clinical and theoretical studies. In this and previous studies we have found no adverse bias in prescribing practice related to ethnicity.
Footnotes
Appendix 1
Acknowledgements
The authors of this article wish to thank Olubanke Dzahini for her statistical support and advice.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.