
Abstract
Objectives:
The objective of this work was to study characteristics and clinical treatment patterns of bipolar disorder (BD) patients admitted to hospital and treated with quetiapine (immediate-release [IR] or extended-release [XR] formulations).
Methods:
BD patients admitted to hospital and prescribed quetiapine IR were followed by linking two Swedish nationwide registries; the hospitalization and drug dispense registries [ClinicalTrials.gov identifier: NCT01455961]. The study period was from 1 January 2008, to end of 31 December 2011. Data was primarily analysed using descriptive methods.
Results:
Quetiapine IR was used in 1761 patients of whom 1303 subsequently switched to XR (switch XR) and 458 remained on IR (continuous IR). At baseline, Switch XR patients were younger (−3.3 years), more frequently employed (+7.1%), had higher prevalence of single depressive episodes (+6.7%) and anxiety disorders (+5.8%), lower mean daily IR dose (−19.3%) and fewer medications for somatic disorders (−7.5%) than continuous IR patients. During follow up, the number of concomitant psychiatric medications was lower in switch XR patients (−6%) and higher in continuous IR patients (+6%). Mean daily quetiapine dose was 21% higher in switch XR versus continuous IR patients. Prescriptions of lower quetiapine dosages calculated below 50 mg per day in the XR switch and IR continuous groups were seen in 8% versus 10% of the patients, respectively.
Conclusions:
Differential use of quetiapine XR and IR in bipolar disorder patients with different and important characteristics was demonstrated. Patients who were switched to quetiapine XR had a higher psychiatric disease burden, were younger and had a higher degree of employment. These differences demonstrate the heterogeneity among bipolar disorder patients and indicate the need in clinical practice for individualized treatment to reduce the risk for both patient and society related losses.
Keywords
Introduction
Bipolar disorder (BD) is a complex, chronic, psychiatric disease characterized by one or more episodes of mania/hypomania that alternate with recurring, major depressive episodes [Lloyd et al. 2011; Price and Marzani-Nissen, 2012]. It represents a huge burden to the healthcare system with an estimated prevalence of 1–2.4% [Fajutrao et al. 2009; Merikangas et al. 2011]. In Sweden the annual prevalence of BD has been reported to have risen sharply during 1991–2010 [Carlborg et al. 2014], adding more concern to the epidemiological development of this disease.
BD has a poor prognosis associated with significant functional impairment caused by severe, chronic depression and consequently an increased risk of suicide [Fajutrao et al. 2009; Kupka et al. 2007; Lloyd et al. 2011; Merikangas et al. 2011; Price and Marzani-Nissen, 2012]. Comorbidity, including substance abuse and cardiovascular morbidity, is also found to be more prevalent in BD patients, thereby lowering their life expectancy more than that of the general population [Angst et al. 2002; Fajutrao et al. 2009; Laursen et al. 2007, 2013; Wahlbeck et al. 2011; Weiner et al. 2011; Westman et al. 2013]. Finally the management of BD patients is complicated by their lack of adherence to treatment [Berger et al. 2012; Gibson et al. 2013; Montes et al. 2013]. This combination of factors has a considerable impact on the disease burden and prognosis of BD [Gibson et al. 2013; Prince et al. 2007; Montes et al. 2013], the magnitude of which may have been underestimated previously [Fajutrao et al. 2009].
The heterogeneity of patient characteristics make individualized drug treatment crucial for treatment success as regards side effects, adherence challenges and patient preferences [Altamura et al. 2008; Montes et al. 2013; Parks et al. 2009]. In order to tailor drug treatment for BD patients, mood stabilizers, antidepressants and/or a combination of the two drug classes usually are used [Jeong et al. 2013; Haeberle et al. 2012]. Recent guidelines however advocate the use of mood stabilizers, as well as the use of monotherapy with atypical antipsychotics (AAPs) [Goodwin, 2009; Hirschfeld et al. 2002; Mahli et al. 2010; Spjut, 2003; Yatham et al. 2013], which may simplify treatment and increase the likelihood of treatment adherence.
Among the AAPs quetiapine is an established, first-line, oral treatment for BD [Cristancho and Thase, 2010] and exists in two formulations, extended release (XR) and immediate release (IR) [Kapur et al. 2000; Figueroa et al. 2009; Nord et al. 2011]. Quetiapine XR is characterized by sustained drug exposure with once-daily dosing, a faster dose titration and improved pharmacodynamic and tolerability profiles compared with quetiapine IR [Figueroa et al. 2009; Peuskens et al. 2007; Nemeroff et al. 2002]. The latter requires a longer dose titration period and is administered twice daily for manic episodes and as prophylaxis. Sedation, being the most common side effect with quetiapine IR treatment, may be less observed with quetiapine XR [Datto et al. 2009; Riesenberg et al. 2011].
Although both formulations of quetiapine are used to treat BD [Cristancho and Thase, 2010; Suppes et al. 2010], their different properties may influence their actual clinical usage in a real-life clinical setting. This was recently documented for patients with schizophrenia, where differential use of the two formulations were demonstrated in real-life clinical practice [Eriksson et al. 2012; Emborg et al. 2012].
Little, however, is known about the relative use of quetiapine XR/IR in real-life treatment of patients with BD, although a recent naturalistic study showed differential use of the two formulations in a small subgroup of patients with BD [Hallinen et al. 2012]. The aim of this epidemiological registry study in Sweden was to ascertain whether there were also differences in clinical practice as regards treatment patterns and patient characteristics for BD patients treated with quetiapine IR continuously compared with those who were switched to quetiapine XR.
Methods
Patient population
All patients with a diagnosis of BD (International Statistical Classification of Diseases [ICD]; ICD9: 296.0, 296.4–296.8, 296A, 296C–296E, 296W; and/or ICD10: F30, F31), hospitalized at least once since 1987 and prescribed quetiapine XR and/or quetiapine IR, were identified in the mandatory Swedish National Patient Register (NPR), and linked to data from the Prescribed Drug Register, the Cause of Death Register and socioeconomic data (Statistics Sweden). The linkage of data was performed by the Swedish National Board of Health and Welfare. The personal identification number used to identify patients was replaced by a study identification number prior to subsequent data processing. Validation of diagnoses from the NPR has been assessed previously [Ludvigsson et al. 2009].
BD was defined as the most recent diagnosis of patients in connection with their in- or out-patient visits. The study groups of interest were patients treated either with quetiapine IR (initial prescription dispensed before 1 January 2008 and with at least one consecutive prescription dispensed after 1 January 2009) or patients switched to quetiapine XR treatment from previously prescribed quetiapine IR. Exclusion criteria were diagnoses of schizophrenia prior to or after inclusion, initial prescription of quetiapine XR, and initial prescription with quetiapine IR as monotherapy after 1 January 2008.
The index date (baseline) was defined as the first prescription of either quetiapine XR or quetiapine IR dispensed after 1 January 2009. The end of observation was 31 December 2011 and patients with index date after 31 January 2010 were excluded to allow at least 1-year follow up.
Study objectives
The primary objective was to determine the detailed clinical treatment of BD patients treated either with quetiapine IR or who were switched to quetiapine XR. Secondary objectives included the determination of patient demographics, comorbidities, concomitant medications and socioeconomic factors.
Statistical analyses
Data for both the primary and secondary objectives were primarily analyzed using descriptive methods. The mean and standard deviations are presented for continuous variables, and the frequencies and percentages are presented for categorical variables. In addition, the groups were compared using Students t-test for continuous variables and chi-square test for dichotomous variables. A p-value below 0.05 was considered as significant.
Baseline drug treatments were collected by registration of dispenses within 1 year before index. Socioeconomic data was assessed in the year before the year of index date, due to governmental annual register updates in the national registries. Registration of comorbidities was searched for at all available data prior to the index date.
Drug dosage was calculated to indirectly estimate the burden of disease. For dispensed prescriptions with a valid dose text (i.e. a text with information about the number of tablets per day or daily dose), the daily dose was estimated as [number of tablets per day * strength]. For subjects without the dose information text, the dose was estimated as [total number of tablets at dispense * strength/14]. Dispensed prescriptions with a dose text that lacked any valid information were not included in the dose calculations.
Study ethics
The study protocol was reviewed and approved by the regional ethics committee in Stockholm, Sweden (2011/1170-31/3) and registered at ClinicalTrials.gov [ClinicalTrials.gov identifier: NCT01455961]. The study was conducted in accordance with the principles stated in the Declaration of Helsinki, ICH GCPs and the applicable legislations on Non-Interventional Studies.
Results
Patient population
We identified a total of 5219 BD patients who were prescribed quetiapine XR or IR during the study period. Of these, 34% (1761 patients) fulfilled the inclusion criteria and were included in this study. Among excluded patients 2133 (41%) started XR without prior treatment with IR and 1325 (25%) patients started IR after 1 January 2008 and did not switch to XR. The majority of included patients were switched to quetiapine XR (74.0%; 1303 patients) and the remaining patients (26%; 458 patients) continued on IR.
Patient demographics
BD patients in the XR switch group were approximately 3 years younger and had a 2-year shorter disease history before index than BD patients in the IR continuous group (Table 1). Although the employment level for both groups tended to be low, it was 7.1% higher in the XR switch group compared with the IR continuous group. Similar healthcare utilization in both groups was reflected by the comparable number of hospital outpatient visits and hospitalizations 3 years before the index date (Table 1).
Patient population demographics at index date.

Chi-square test for categorical variables, t-test for numeric variables.
Patient characteristics prior to the index date
Patients in the XR switch group were diagnosed 6.7% more often with single depressive episodes and 5.8% more often with anxiety disorders compared with the IR continuous group (Figure 1).

The psychiatric comorbidity burden in patients with bipolar disorder who switched from quetiapine IR to XR (XR switch group) and those who continued IR treatment (IR continuous group) prior to index date.
Concomitant treatment with antipsychotic medication (AP) was more frequently used in the XR switch than the IR continuous group. The use of lithium was numerically higher in the XR switch group (Figure 2). Patients in the XR Switch group were prescribed a lower mean daily dose of quetiapine IR (218 versus 270 mg/day) and fewer were receiving medications for somatic diseases (39.0 versus 46.5%) than those in the continuous IR group (data not shown). The frequency of patients on lower dosages calculated below 50 mg of quetiapine per day in the XR switch and IR continuous groups were 8% versus 10%.
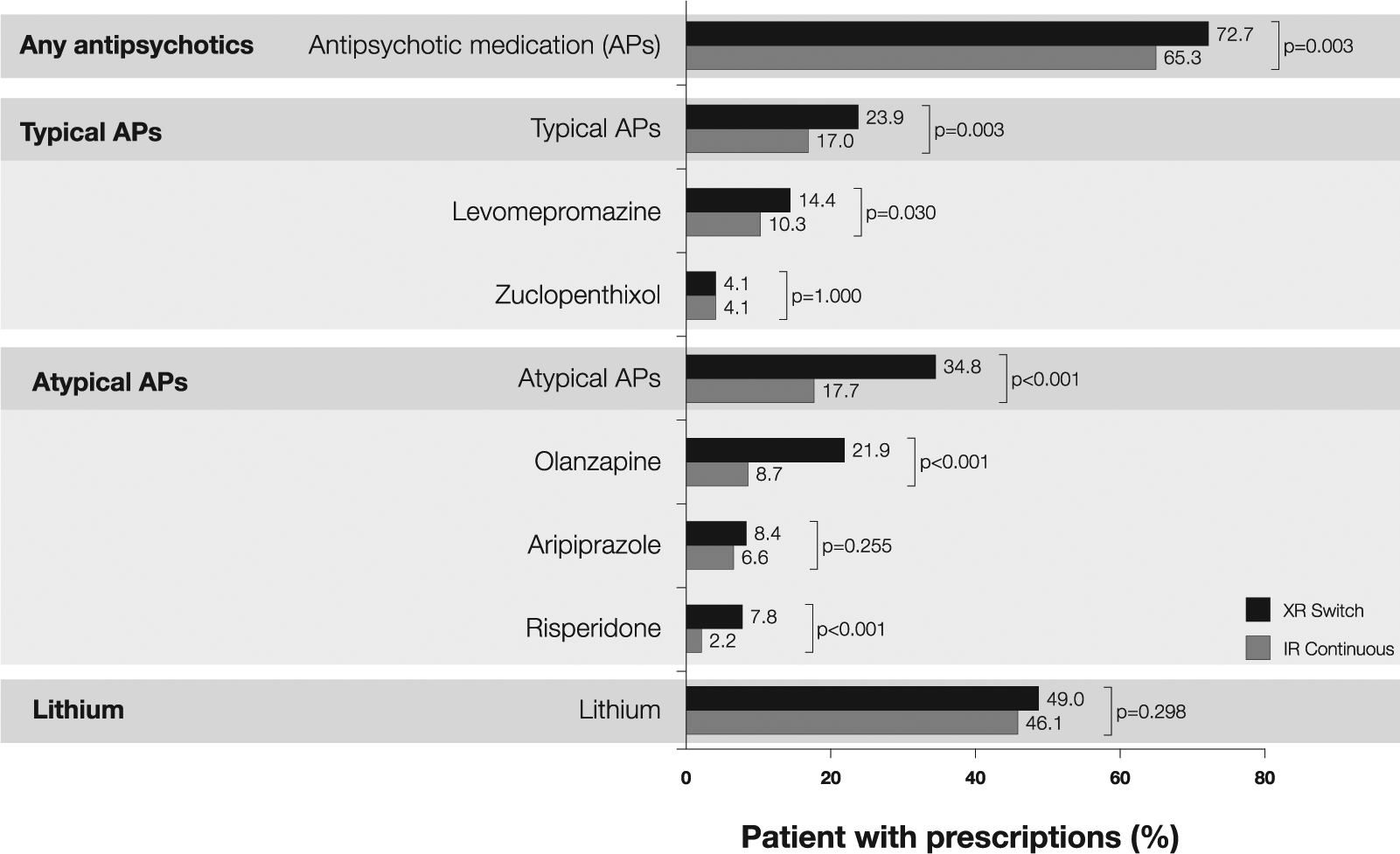
Concomitant medications, prior to index date, in quetiapine XR switch versus IR continuous patients with bipolar disorder.
Patient characteristics after the index date
During the follow-up after switch to quetiapine XR, the number of concomitant AAP and antidepressant medications in patients was decreased, while it increased in the IR Continuous group (Figure 3). In general, the most commonly coprescribed AAPs were olanzapine, aripiprazole and risperidone, whilst the most commonly, coprescribed antidepressants were the selective serotonin reuptake inhibitors, nonselective monoamine reuptake inhibitors and other antidepressants (Figure 3, detailed data not shown).

Concomitant treatment with atypical antipsychotic medications (AAPs) and antidepressants for quetiapine extended release (XR) switch and immediate release (IR) continuous patients before versus after index date.
The mean daily dose of quetiapine prescribed to patients who switched from IR to XR treatment was higher than in those who continued treatment with quetiapine IR, i.e. 305 versus 252 mg/day, respectively (data not shown).
Discussion
In this study, 15% of all BD patients in Sweden were initiated on quetiapine IR at some point, and the majority of these patients (72%) were subsequently switched to the quetiapine XR formulation. Patients who were switched showed a higher degree of depressive disorders, anxiety disorders, and other mental and behavioral disorders than patients continuing on quetiapine IR. The higher psychiatric disease burden was further stressed by the more frequent use of concomitant AAPs and various classes of antidepressants, reflecting a common use of mood stabilizers, antidepressants and/or a combination of the two drug classes to treat both the anxiety and depressive phase of BD [Jeong et al. 2013; Haeberle et al. 2012].
Following their switch to quetiapine XR, the number of concomitant AAP and antidepressant medications prescribed to these patients was slightly less, while it was higher in patients who remained on quetiapine IR. The observed use of higher daily quetiapine dosages is supported by previous reports and suggests more psychiatrically burdened patients. For example, recent findings in patients with schizophrenia and BD showed that quetiapine XR was more often used as monotherapy and in significantly higher doses than quetiapine IR [Hallinen et al. 2012]. Similar findings have been suggested in other studies in patients with schizophrenia, where quetiapine IR was used at lower doses as as-needed medication for its sedative and/or anxiolytic effects, whilst quetiapine XR was used at higher doses for its antipsychotic effect [Emborg et al. 2012; Eriksson et al. 2012].
Both this study and that of Eriksson and colleagues suggest that more severely affected patients are treated with quetiapine XR. The switch behavior may indicate a need for an alternative treatment for patients with a high psychiatric burden who have difficulties in complying with twice-daily quetiapine IR and require higher doses of quetiapine XR [Jeong et al. 2013; Hirschfeld et al. 2006; Suppes et al. 2010; Thase et al. 2006; Vieta et al. 2007; Weisler et al. 2008].
In this psychiatrically burdened group, higher doses of quetiapine XR also increase the likelihood of effectively treating BD symptoms with less sedative effect than quetiapine IR [Cristancho and Thase, 2010; Figueroa et al. 2009; Peuskens et al. 2007; Nemeroff et al. 2002; Reisenberg et al. 2011].
The patients in our study had symptoms and high levels of comorbidities characteristic of the general BD population [Angst et al. 2002; Laursen et al. 2007, 2013; Wahlbeck et al. 2011; Weiner et al. 2011; Westman et al. 2013] and comparable treatment patterns [Berger et al. 2012; Haeberle et al. 2012; Post et al. 2010]. This complexity of comorbidity seen in BD [Merikangas et al. 2007; Price and Marzani-Nissen, 2012] results in polypharmacy [Berger et al. 2012; Haeberle et al. 2012; Post et al. 2010], which may lead to treatment nonadherence [Berger et al. 2012; Gibson et al. 2013; Montes et al. 2013]. Better adherence to treatment is clinically important and might also translate into a reduced burden on the national economy since BD is associated with very high societal costs per patient [Ekman et al. 2013]. Interestingly, Locklear and colleagues recently suggested that mental-health-related hospitalizations and costs are reduced in BD patients after initiation with quetiapine XR compared with patients initiated on quetiapine IR [Locklear et al. 2013].
The substantial clinical burden of BD on the healthcare system and significantly higher levels of comorbidity in BD patients compared to the general population are well documented [Angst et al. 2002; Fajutrao et al. 2009; Laursen et al. 2007, 2013; Wahlbeck et al. 2011; Weiner et al. 2011; Westman et al. 2013]. A recently reported study in schizophrenia found that significantly more patients treated with quetiapine XR had somatic diseases than quetiapine IR-treated patients [Eriksson et al. 2012]. In this study, quetiapine XR-treated patients were both younger and had higher levels of employment than quetiapine IR-treated patients, suggesting a more fragile and complex patient group in need of optimized treatment, but with greater potential to achieve fewer sick leave days. Further investigations are required to determine whether or not these patients also have the high burden of somatic disease typical of BD since they received fewer medications for somatic diseases. It may be that the higher psychiatric disease burden in these patients dominates their general clinical assessment and treatment of somatic disease is overshadowed by psychiatric prioritizations.
The strength of this nationwide registry study was the large number of patients included without patient selection due to comorbidities commonly present in randomized clinical trials, need for informed consent, and the similar patient demographics in the compared groups. The impact of regional differences in treatment guidelines was minimized by using nationwide and mandatory registers.
However, as with all retrospective, observational studies, the present study may have limitations. Quetiapine IR is known to be prescribed in low dosages to address sleeping disorders, information which is lacking in the present data set. However, the similar frequency of lower calculated quetiapine dosages (<50 mg/day) in both groups support prescription for the BD indication. Validation of the clinical diagnosis is a general problem with registry-based studies and also applies here. It is also unclear, given the ICD classification used, whether the diagnoses of BD refer to type I or type II and if the individual treatment prescription is used for manic/depressive episodes or prophylaxis. Furthermore, as the study was performed in Sweden only, the results may not be fully representative of other countries.
Overall, we found that BD patients in Sweden were treated according to guidelines advocating the use of AAP monotherapy [Goodwin, 2009; Hirschfeld et al. 2002; Mahli et al. 2010; Spjut, 2003; Yatham et al. 2013]. Both quetiapine XR and IR are commonly used to treat BD, but their actual clinical use differs. In our study, the majority of patients initiated on quetiapine IR were switched to XR, and represented a more psychiatrically burdened group compared to patients who did not switch from quetiapine IR. The high frequency of switches and differential use of quetiapine have been reported previously [Berger et al. 2012; Dell’Osso et al. 2012; Haeberle et al. 2012] and support a role for both quetiapine IR and XR in the treatment of BD.
In conclusion, 15% of all BD patients in Sweden are, at some point, initiated on quetiapine treatment. Despite being the same drug, but with two different formulations, quetiapine IR and XR are used in patients with different characteristics. Quetiapine XR was used in BD patients with a greater burden of psychiatric comorbidity before switch, compared to patients treated continuously with quetiapine IR. Although there was a higher disease burden in the quetiapine XR group, patients were younger and had a higher degree of employment than those of the IR group. Following switch to quetiapine XR, patients received a higher, mean daily quetiapine dose compared with those in the continuous IR group and decreased their use of concomitant psychiatric drugs. This study shows the extensive use of both XR and IR formulations in patients with BD, with quetiapine XR being used more often in more fragile patients with a higher potential to reduce sick leave, and thus indicates a need for both formulations in clinical practice. Switching does occur between the two formulations but more studies are required to investigate reasons for the switch.
Footnotes
Author’s note
This manuscript was prepared in line with guidelines established by the International Committee of Medical Journal Editors (ICMJE) and published in its Uniform Requirements of Manuscripts Submitted to Biomedical Journals.
Funding
This study was sponsored by AstraZeneca. AstraZeneca employees were members of the study committee that had overall responsibility for the concept, design and data analyses. Dr Grażyna Söderbom from Klipspringer AB provided medical writing support funded by AstraZeneca.
Conflict of interest statement
Andreas Carlborg has acted as a consultant to and participated in clinical trials by AstraZeneca Nordic, and has lectured for and received grants from AstraZeneca and Wyeth. Marcus Thuresson is a full-time employee at Statisticon AB. Johan Bodegard is a full-time employee at AstraZeneca. Lena Ferntoft was a full-time employee at AstraZeneca at the time of this study.