
Abstract
Introduction:
Around 40–60% of the patients with obsessive–compulsive disorder (OCD) remain unimproved by serotonin reuptake inhibitors (SRIs). Goal of this study was to compare the efficiency and safety of aripiprazole versus quetiapine, in patients with OCD, who did not respond effectively to fluvoxamine.
Method:
A total of 44 female inpatients with OCD, who did not respond successfully to fluvoxamine at maximum dose (300 mg/day) and duration (12 weeks), were assigned randomly, in a double-blind trial, to receive aripiprazole (n = 22) or quetiapine (n = 22), in addition to their SRI, for 12 weeks. Treatment response was assessed by the Yale–Brown Obsessive–Compulsive Scale (YBOCS), as primary outcome measure, and Clinical Global Impressions-Severity Scale (CGI-S), as a secondary outcome measure.
Results:
A total of 27.27% of the cases in the aripiprazole group (n = 6) and 54.54% of them in the quetiapine cluster (n = 12) responded moderately to the aforesaid augmentation. The mean ± SD baseline YBOCS score of 33.27 ± 3.90 dropped to a mean of 30.72 ± 4.67 (p = 0.06) in the aripiprazole group, and from 31.18 ± 4.93 to 27.97 ± 3.71 (p = 0.01) in the quetiapine group, at the end of the evaluation. There was no significant change with respect to CGI-S in either of the aforesaid groups.
Conclusion:
This study shows that treatment-resistant OCD patients may benefit more from addition of quetiapine in comparison with aripiprazole, to their ongoing SRI therapy.
Introduction
Obsessive–compulsive disorder (OCD) is a psychiatric disorder that affects 2–3.5% of people during their lifetimes [Sasson et al. 1997]. Poor response occurs in 40–60% of people that are prescribed first-line pharmaceutical treatments such as selective serotonin reuptake inhibitors (SSRIs), and moreover 20–40% do not respond adequately even after several prescriptions [Expert Consensus Panel for Obsessive–Compulsive Disorder, 1997; Catapano et al. 2006].
Therapeutic strategies in these resistant cases usually consist of augmentation therapies with a range of adjunctive drugs, including antipsychotics. Treatment with second-generation antipsychotics (SGAs) that show fewer extrapyramidal symptoms, in comparison with typical antipsychotics, may be a useful alternative for treatment-refractory OCD patients. The broader range of effective treatment with the addition of atypical antipsychotics may be due to D2 blockade or a combined serotonergic–dopaminergic blockade, particularly a 5-HT2A and D2 antagonism [Komossa et al. 2010]. However, according to Bloch and colleagues [Bloch et al. 2006], only one-third of treatment-refractory OCD patients show a meaningful treatment response to antipsychotic augmentation, along with sufficient evidence that demonstrates the efficacy of haloperidol and risperidone, and inconclusive data regarding quetiapine and olanzapine. In addition, patients with comorbid tics are likely to have a differential benefit to antipsychotic augmentation [Dold et al. 2011]. This group also, according to a meta-analysis, declared risperidone more efficacious than other SGAs in treatment-resistant OCD [Dold et al. 2011]. In addition, with respect to newer SGAs, there are a number of clinical trials in the literature with different outcomes as regards the effectiveness of quetiapine [Kordon et al. 2008; Carey et al. 2005; Denys et al. 2004; Fineberg et al. 2006] and aripiprazole [Pessina et al. 2009; Muscatello et al. 2011; Delle Chiaie et al. 2011; Ak et al. 2011]. In this study, the efficacy and safety of aripiprazole has been compared with quetiapine in a group of patients suffering from treatment-resistant OCD.
Method
This study was approved by University’s Medical Ethics Committee. A total of 44 female in-patients, as accessible sample in the chronic ward of the hospital, after full explanation of the procedure for them and obtaining signed informed consent, were entered into a 12-week parallel group, double-blind study for random assignment to adjunctive aripiprazole (n = 22 patients) or quetiapine (n = 22 patients), plus their regular prescription. Patients were diagnosed with OCD according to the criteria of Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision [APA, 2000].
Cases with identified comorbidity, such as substance misuse, mood, medical and neurological problems, had been excluded from the trial. Inclusion criteria in this study were as follows.
OCD symptoms resistant to fluvoxamine at maximum dose (300 mg/day) and long enough duration (12 weeks).
A score on the YBOCS of at least 18. During the trial, whereas the patients, staff and assessor were unaware of the prescribed augmentation that were packed into identical capsules, all patients continued to take their current SRI (fluvoxamine) at the maximum dose (300 mg/day) during assessment. Aripiprazole addition was initiated at a dose of 2.5 mg/day and then increased by 2.5 mg increments in weekly meetings, to a maximum of 10 mg by week 4 and then this dose was held constant to the end of the study. Quetiapine (immediate-release formulation) as well was started by 25 mg bid, and then increased by 75 mg in weekly meetings, to maximum of 300 mg by week 4 and that dose was held constant to the end of the study. No other psychotropic drug or psychosocial intervention, during the trial, was administrated for them.
The primary outcome measure was YBOCS [Goodman et al. 1998]. Clinical Global Impressions-Severity Scale (CGI-S) also was used as the secondary outcome [Guy, 1976]. Full response to treatment was defined of at least 50% decrease in YBOCS score and partial response as between 25% and <50% decrease in that score in comparison with the baseline. The study duration was 12 weeks, and the patients were assessed by means of YBOCS at baseline (week 0), and weeks 2, 4, 8, and 12. CGI-S was scored at the baseline and at the end of the assessment. Adverse events were assessed at each visit by means of patients’ spontaneous reports and clinical examination by psychiatrist.
Statistical analysis
Patients were compared on baseline characteristics by means of t tests. Treatment efficacy also was analyzed by t test and repeated-measures analysis of variance (ANOVA) comparing both groups over 12 weeks. Statistical significance was defined as a two-sided p value ≤0.05. MedCalc, version 9.4.1.0, was used as statistical software tool for analysis.
Results
Analysis for efficacy was based on data from an equal number of patients in both groups, which were initially comparable, and demographic and diagnostic variables were analogous (Table 1). According to the findings, there was no full response in any of the cases in either group. A total of 6 patients (27.72%) in the aripiprazole group and 12 patients in the quetiapine group (54.54%) showed partial response, with a decrease from 33.17 ± 3.90 to 30.72 ± 4.67 and 31.18 ± 4.93 to 27.97 ± 3.71 by aripiprazole and quetiapine, respectively (Tables 2 and 3).
Demographic characteristics of patients participating in the quetiapine and aripiprazole groups.

Abbreviations: YBOCS, Yale–Brown Obsessive–Compulsive Scale; CGI-S, Clinical Global Impressions-Severity Scale; SD, standard deviation; SE, standard error.
Percentage of positive response on the YBOCS, in the aripiprazole and quetiapine groups.

Between-group analysis of primary outcome measure at baseline (week 0) and weeks 2, 4, 8 and 12.

Abbreviations: YBOCS, Yale–Brown Obsessive–Compulsive Scale; OCD, obsessive–compulsive disorder; SD, standard deviation; SE, standard error.
Within-group analysis showed that although this improvement was significant in the quetiapine group (t = 1.88, p = 0.01) at the end of the trial, but it was not so with aripiprazole (t = 2.44, p = 0.06); see Table 3.
In addition, repeated-measures ANOVA regarding YBOCS, did not show any significant improvement by aripiprazole [F(4,84) = 0.636, p < 0.63, SS = 1058.00, MSe = 416.07], whereas a remarkable improvement was evident by quetiapine [F(4,84) = 10.8, p < 0.04, SS = 286.64, MSe = 8.45] at the end of the assessment, and also in comparison with aripiprazole [F(1,105) = 3.71, p < 0.05, SS = 4.09, MSe = 1.10], in a split-plot (mixed) design ANOVA. In addition, while head-to-head analysis could not illustrate any important difference between quetiapine and aripiprazole in weeks 2, 4 and 8, it was significant in week 12 (Table 3 and Figure 1).
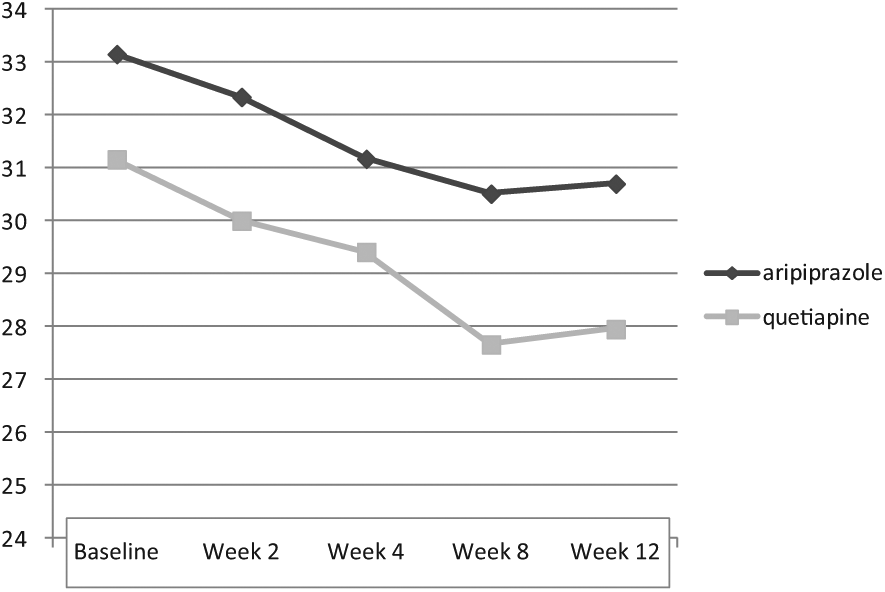
Changes of mean YBOCS between week 0 (baseline) and 12.
Also, with respect to CGI-S, no significant change was evident by aripiprazole (3.29 ± 0.33 to 3.17 ± 1.02; t = 0.52, p = 0. 60) or quetiapine (3.38 ± 0.08 to 3.32 ± 0.14; t = 1.74, p = 0.08), though perhaps a better response was noticeable with the latter one.
As the sample size was small, the effect size (ES) was analyzed for changes on the YBOCS and CGI-S at the end of the assessment. Outcome indicated a medium improvement of YBOCS by both quetiapine (d = 0.7, r = 0.3) and aripiprazole (d = 0.5, r = 0.2). Also, there was small and medium improvements of CGI-S by aripiprazole (d = 0.15, r = 0.07) and quetiapine (d = 0.5, r = 0.2), respectively.
Post hoc analysis showed power = 0.49 on behalf of this trial, which turned to power = 0.79 in compromise power analysis. The most common adverse effects of aripiprazole and quetiapine in our samples, during the trial, were somnolence (27.77% and 45.55%, respectively), dizziness (18.18% and 54.54%, respectively) and weight gain (27.27% in the quetiapine group only, with a mean increase of 0.36 ± 0.11 kg) and inner unrest (18.18% in the aripiprazole group). Since the side effects were mild and well tolerated, then no one dropped out owing to medication intolerance.
Discussion
According to the result of this study, the addition of aripiprazole and quetiapine to ongoing SRI treatment may be efficacious for treatment-refractory OCD patients, a finding that was significant only in the quetiapine group. Perhaps a longer duration of trial or higher dosage could result in significant outcomes in the aripiprazole group and better results in the quetiapine cluster. In this regard, although the baselines were generally comparable, the severity of the primary outcome measure in the aripiprazole group was greater than the secondary. This may have influenced the end result of our appraisal. The same issue is also applicable to the doses of these drugs, which only could be roughly considered as comparable. It is mentionable that in a somewhat similar approach, Selvi and colleagues, in a single-blind, randomized study, had also found risperidone more effective than aripiprazole for improvement of YBOCS [Selvi et al. 2011].
In general and with respect to quetiapine, in contrast to Kordon and colleagues [Kordon et al. 2008] and Carey and colleagues [Carey et al. 2005], the result of our study was comparable with the findings of Denys and colleagues [Denys et al. 2004] and Fineberg and colleagues [Fineberg et al. 2006], while in connection with aripiprazole, it was not in concord with Pessina and colleagues [Pessina et al. 2009], Muscatello and colleagues [Muscatello et al. 2011], Delle Chiaie and colleagues [Delle Chiaie et al. 2011] and Ak and colleagues [Ak et al. 2011]. The primary outcome measure of all of the above trials was YBOCS, except than the last two, who used YBOCS plus CGI-S.
Nonetheless this diversity could be the outcome of dissimilarities between intervening factors, such as the kind of prescribed SRI, duration of study, patient’s gender, and, in particular, the criteria of response. The main problem here is that there is some inconsistency in the definition of treatment refractoriness and there is not yet any universal agreement on the definition of responsiveness or resistance in the realm of OCD. Therefore, first of all, clear criteria for no response need to be agreed upon because frequently the standards for response rates differ to a large extent. For example, Weiss and colleagues [Weiss et al. 1999] used a cutoff of 50% decrease in YBOCS score as responders, while Francobandiera [Francobandiera, 2001] chose a cutoff of 25%. On the other hand, McDougle and colleagues [McDougle et al. 2000] used a more restrictive criterion with a cutoff of 35% for YBOCS decrease and a final score of 16 on the YBOCS in combination with a final CGI-S rating of much improved or very much improved. Such differences invalidate the comparison of effect sizes between studies.
As regards quetiapine, Komossa and colleagues [Komossa et al. 2010] found that although quetiapine combined with antidepressants was no more efficacious than placebo combined with antidepressants in terms of response of patients with OCD to treatment, but it showed a significant superiority in comparison with olanzapine and risperidone in improvement of the mean YBOCS score. In addition, some beneficial effects of quetiapine, in terms of anxiety or depressive symptoms, were observable.
Alternatively and according to Denys and colleagues [Denys et al. 2004], not only quetiapine was superior to placebo regarding improvement of YBOCS in treatment-resistant OCD, but the best response was visible by means of its combination with clomipramine, fluoxetine, and fluvoxamine and with the lowest SRI doses.
Indeed, specific sociodemographic factors, including pharmacogenetic and clinical characteristics of the patients, and in addition, different treatments received by them in the past, could also have contributed to the modest responses in the current measurement.
Unlike other studies by olanzapine and risperidone, in this one, weight gain and extrapyramidal symptoms were not the most common side effects and also complaints such as somnolence, dizziness, and weight gain were mild to moderate and did not cause serious problems for the patients. Better tolerance and side-effect profiles, particularly in long term, may perhaps put quetiapine in a better position in comparison with the aforesaid SGAs. Small sample size, short duration of study, gender-based sampling and lack of placebo arm, which may have significant impact on the assay sensitivity of the study and artificially inflate results in an active comparator trial, were among the weak points of this trial. Surely, intermediary power of current assessment implies necessity of larger samples for verification of the outcome of this experiment.
Further analogous trials in future possibly will improve our knowledge in this regard.
Conclusion
This study shows that treatment-resistant OCD patients may benefit more from the addition of quetiapine, in comparison with aripiprazole, to their ongoing SRI therapy.
Footnotes
Acknowledgements
The authors gratefully acknowledge their dear colleagues, S. Akbari, MD and P. Sadeghi, MS, and the Department of Research for their practical and financial support of this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.