
Abstract
Introduction
Prolongation of Q-Tc interval is commonly accepted as a surrogate marker for the ability of a drug to cause torsade de pointes. In the present study, safety of olanzapine versus risperidone was compared among a group of patients with schizophrenia to see the frequency of the electrocardiographic alterations induced by those atypical antipsychotics.
Method
Two hundred and sixty-eight female inpatients with schizophrenia entered in one of the two parallel groups to participate in an open study for random assignment to olanzapine (n = 148) or risperidone (n = 120). Standard 12-lead surface electrocardiogram (ECG) was taken from each patient at baseline, before initiation of treatment, and then at the end of management, just before discharge. The parameters that were assessed included heart rate (HR), P-R interval, QRS interval, Q-T interval (corrected = Q-Tc), ventricular activation time (VAT), ST segment, T wave, axis of QRS, and finally, interventricular conduction process.
Results
A total of 37.83% of cases in the olanzapine group and 30% in the risperidone group showed some Q-Tc changes; 13.51% and 24.32% of the patients in the olanzapine group showed prolongation and shortening of the Q-Tc, respectively, while changes in the risperidone group were restricted to only prolongation of Q-Tc. Comparison of means showed a significant increment in Q-Tc by risperidone (p = 0.02). Also, comparison of proportions in the olanzapine group showed significantly more cases with shortening of Q-Tc versus its prolongation (p = 0.01). No significant alterations with respect to other variables were evident.
Conclusion
Olanzapine and risperidone had comparable potentiality for induction of Q-Tc changes, while production of further miscellaneous alterations in ECG was more observable in the olanzapine group compared with the risperidone group. Also shortening of Q-Tc was specific to olanzapine.
Introduction
The risk of sudden cardiac death for individuals receiving antipsychotic drugs is about 2.4 times greater than that for nonusers [Agelink, 2002]. Prolongation of Q-Tc interval is commonly accepted as a surrogate marker for the ability of a drug to cause torsade de pointes (TdP). Although an absolute Q-Tc interval of more than 500 ms or an increase of 60 ms from baseline is regarded as indicating an increased risk of TdP, TdP can also occur with lower Q-Tc values or changes [Agelink, 2002; Sana et al. 2003]. Generally, the normal Q-Tc should not exceed 0.42 s in men and 0.43 s in women [Goldman, 1982]. According to Reilly, 8% of the psychotropic drug users had Q-Tc interval measurements two standard deviations greater than the mean for normal comparison subjects, which rose to 15% among subjects taking both tricyclic antidepressants and antipsychotic drugs (especially thioridazine) [Reilly et al. 2000]. Also, an increased risk of mortality (1.6–1.7 times greater), possibly due to heart failure or sudden death, has been reported with the use of olanzapine in the treatment of older patients with dementia, and so it has not been approved by the US Food and Drug Administration for use in the treatment of such patients [Kales et al. 2007].
However, a number of drugs, like digitalis, lamotrigine, rufinamide, mallotoxin, levcromakalim and nicorandil, have been found to actually shorten the action potential duration and QT interval, as well as being profibrillatory [Shah, 2010]. At first, this effect observed in nonclinical studies was treated as an idiosyncrasy of questionable clinical significance and generally received little further attention. However, recent clinical description of congenital forms of short QT interval syndrome (SQTS) and the arrhythmias associated with these syndromes have begun to raise concerns regarding the potential proarrhythmic consequences of drugs that may shorten QT interval in humans [Shah, 2010]. Congenital SQTS is associated with high incidence of syncope, sudden death (possibly due to malignant ventricular tachyarrhythmias) or atrial fibrillation, and these events can occur at any age, including in infants and young adolescents [Shah, 2010].
In the present study, the safety of olanzapine versus risperidone was compared among a group of female patients with schizophrenia to see the frequency of electrocardiographic changes induced by those atypical antipsychotics.
Method
A total of 268 female inpatients with schizophrenia, according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders (APA, 2000, 4th edition, text revision), were entered in either of the two parallel groups to participate in an open study for random assignment to olanzapine (n = 148, 5−25 mg/day) or risperidone (n = 120, 4–8 mg/day). After complete description of the study to the subjects, written informed consent was obtained from either the participant or a legal guardian or representative. The patients were free to stop the medication if they wished. In addition, the whole of the procedure was approved by the related ethical committee of the university. Any patient with any diagnosed medical (such as severe renal or liver disease) or cardiovascular problem ( such as tachycardia, bradycardia, interventricular conduction defect, ischemic heart disease, myocardial or pericardial disease, congestive heart failure), electrolyte disturbances (hypocalcemia, hypercalcemia, hypomagnesemia, hypokalemia, hyperkalemia), cerebral or subarachnoid injury, and also patients who were utilizing other concomitant drugs (such as digitalis that shortens Q-Tc, or quinidine, procainamide or amiodarone that increase Q-Tc, or utilization of mood stabilizers, antidepressants or depot antipsychotics) or patients over 40 years old were excluded from the trial.
The aim of the study was to determine electrocardiographic changes in healthy patients with schizophrenia who were previously on a variety of typical antipsychotics. So, after a minimum 7-day washout period, both of these drugs were prescribed according to practice guidelines and standard titration protocols [Van Kammen and Marder, 2005] and in accordance with the following regimen: 1 mg/day risperidone or 5 mg/day olanzapine at baseline, up to 2 mg/day risperidone and 10 mg/day olanzapine at the end of the first week; and weekly interval increments of 2 mg for risperidone and 5 mg for olanzapine, individually and according to the clinical situation, up to a maximum of 8 mg and 25 mg for risperidone and olanzapine respectively at week 5. The fifth week dosage remained constant up to the end of the study.
Standard 12-lead surface electrocardiogram (ECG) was taken from each patient at baseline, before initiation of the antipsychotic and then again at the end of the treatment, just before discharge (at sunrise, before initiation of daily prescription). No other psychotropic drug was permitted during the assessment. The parameters that were assessed included heart rate (HR), P-R interval, QRS interval, Q-T interval (corrected = Q-Tc), ventricular activation time (VAT), ST segment, T wave, axis of QRS, and finally, interventricular conduction process. Although it is standard practice to measure the QT interval from the beginning of the QRS complex to the end of the T wave, the actual methods of measurement have not been standardized yet and dissimilar opinions exist regarding the most useful method for correction of the Q-T interval for HR (such as Bazett formula, Fridericia cube-root correction or Framingham linear regression equation) [Sana et al. 2003]. In this experiment, measurement of the Q-T interval was based on ‘expert opinion guidelines for measuring the QT interval’ [Sana et al. 2003]. Also, calculation of HR was based on the ‘modified table of Ashman R & Hull E’. Correction of the observed Q-T interval, based on the R-R interval, was done according to the ‘Kissin’s nomogram’ for rate correction of Q-T interval [Goldman, 1982]. Moreover, since the purpose of the current assessment involved detection of various alterations of ECG, caused by the abovementioned drugs, no definite criterion was set for a clinically meaningful alteration in Q-Tc or other related parameters.
Statistical analysis
Patients were compared on baseline characteristics by ‘χ2 tests’ for categorical variables and ‘t tests’ for continuous variables. Also, the results were analyzed by t test or ‘compression of two proportions’ for intra-group and between-group analysis. Statistical significance was defined as a two-sided p value less than or equal to 0.05. MedCalc, version 9.4.1.0, was used as the statistical software tool for analysis.
Results
Groups were initially comparable and demographic and diagnostic variables were analogous (Table 1). A total of 37.83% (n = 56) of cases in the olanzapine group and 30% (n = 36) in the risperidone group showed some Q-Tc changes (comparing baseline with post-treatment stage). In addition, 13.51% (n = 20) and 24.32% (n = 36) of the patients in the olanzapine group showed prolongation (0.01−0.04 s, mean = 0.02 ± 0.01 s) and shortening (0.01−0.04 s, mean = 0.02 ± 0.01 s) of the Q-Tc interval respectively. This reduction in Q-Tc was equivalent to 0.04 s in at least 5.40% (n = 8) of the patients. The abovementioned changes in the risperidone group were restricted to prolongation of only Q-Tc (0.01−0.02 s, mean = 0.016 ± 0.005 s) (Figure 1). A comparison of proportions between olanzapione and risperidone regarding total number of cases in the related groups with Q-Tc change was nonsignificant [z = 1.34, p = 0.17, 95% confidence interval (CI) = −0.03 to 0.19]. Besides, in the olanzapine group, comparisons of means between baseline Q-Tc and its post-treatment measurement, and also between post-treatment Q-Tc in the olanzapine group and the comparable variable in the risperidone group were nonsignificant. But a comparison of means between a baseline Q-Tc of the risperidone group versus its post-treatment measurement showed a significant increment (p = 0.02) (Table 2). In addition, a comparison of proportions in the olanzapine group showed that the quantity of cases with shortening of Q-Tc was significantly more than the number of patients with Q-Tc prolongation (z = −2.37, p = 0.01, 95% CI = −0.19 to −0.01). Moreover, 5.40% (n = 8) of patients in the olanzapine group showed alteration of the P-R interval. Four of these patients showed prolongation (0.02 s) and the others shortening (0.02 s). However, at the end, such an alteration was nonsignificant in comparison with baseline in the related group (p = 0.15) (Tables 2 and 3). In addition, in the olanzapine group, two had synchronized increment of Q-Tc and P-R interval. It should be mentioned that there was no P-R alteration in the risperidone group.
Baseline demographic and electrocardiographic characteristics of the participants.
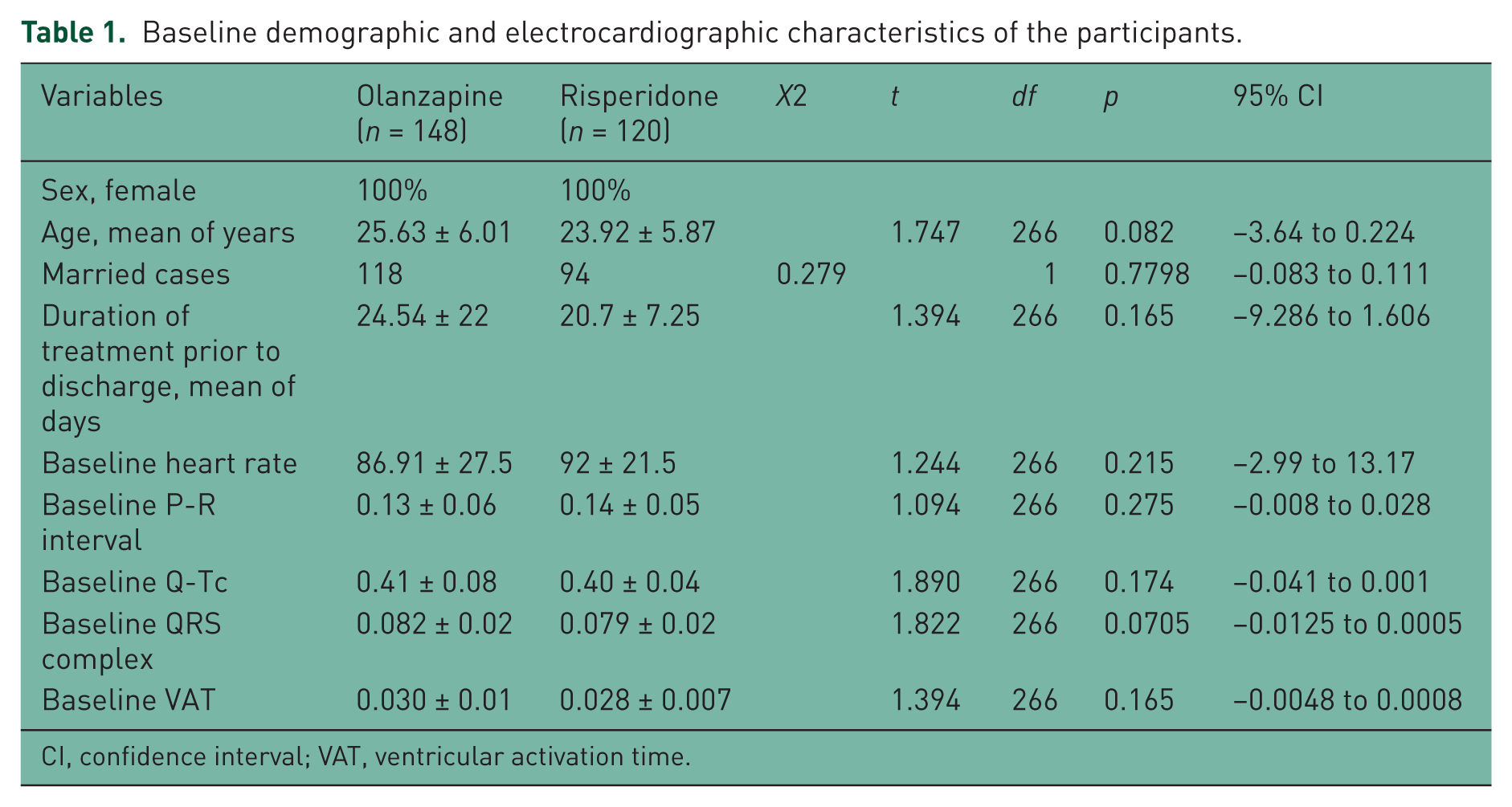
CI, confidence interval; VAT, ventricular activation time.

Percentage of prolongation and shortening of Q-Tc in the olanzapine and risperidone groups.
Intragroup analysis of different parameters, between baseline and final stage of the assessment.

CI, confidence interval; HR, heart rate; VAT, ventricular activation time.
Major finding of the current study.

Intragroup analysis in both groups did not show any significant difference in HR, VAT and QRS complex between baseline and closing stage of the treatment (Table 2). Moreover, no shifting in the S-T segment (depression or elevation) or T-wave alteration was evident among those cases. In the olanzapine group, two patients showed left anterior hemi-block in addition to mild shortening of Q-Tc (0.01 s). No serious adverse effect, like TdP, Brugada syndrome, ventricular tachyarrhythmia, ventricular fibrillation (VF) or sudden death, occurred throughout this experiment. The mean modal dose of olanzapine during the present assessment was 19.49 ± 5.51 mg/day. The most common dosages of olanzapine were 20 mg/day (n = 98, 66.21%), 25 mg/day (n = 26, 17.56%) and 15 mg/day (n = 24, 16.21%). The mean modal dose of risperidone throughout the experiment was 5.14 ± 2.86 mg. The most common doses were 6 mg/day (n = 58, 48.33%), 8 mg/day (n = 48, 40%) and 4 mg/day (n = 16, 13.33%). Also during the study, 26.66% (N = 32) of the cases in the risperidone group and 9.45% (N = 14) in the olanzapine group showed extra-pyramidal side effects. Increase in weight was significantly greater in the patients treated with olanzapine (n = 34, 22.97%) than in those treated with risperidone (n = 10, 8.33%). The mean weight gain in the olanzapine and risperidone groups was about 2.2 ± 0.91 kg and 0.6 ± 0.75 kg respectively. Post hoc power analysis demonstrated an acceptable power of 0.88 [n1 = 148, n2 = 120, α = 0.05, critical t (266) =1.65] for this trial.
Discussion
The main purpose of this study was to compare the effects of olanzapine and risperidone on the ECG of healthy female patients with schizophrenia. According to the findings, there were more significant alterations in the post-treatment ECG of patients in the olanzapine group versus the risperidone group. These alterations included mostly Q-Tc shortening or prolongation, and left anterior hemi-block and P-R interval shortening or prolongation. Moreover in the olanzapine group, there were significantly more cases of Q-Tc shortening in comparison to prolongation. Conversely, a significant increment of mean Q-Tc was induced only by risperidone in the present study, while numerically there was no significant difference between the two groups regarding Q-Tc changes. In spite of all these alterations, fortunately there was no serious cardiac event or increase in Q-Tc in any sample of more than 0.06 s in comparison with baseline, or more than 0. 5 s throughout the appraisal.
While our results were more or less in harmony with the findings of Ravin and Levenson, and Yerrabolu and colleagues as regards the effect of risperidone on Q-T interval [Ravin and Levenson, 1997; Yerrabolu et al. 2000], they go against those of Czekalla and colleagues who stated that ‘risperidone can be used safely in elderly patients, who are often taking several medications, without risk of increased Q-T dispersion’ [Czekalla et al. 2001]. Also, with respect to olanzapine, while our results were not in agreement with Janion and colleagues, who stated that ‘olanzapine is relatively safe and does not contribute significantly to a Q-Tc prolongation that could result in potentially fatal ventricular arrhythmias’ [Janion et al. 2006], they are relatively in accord with Desai and colleagues regarding potentiality of olanzapine for induction of Q-T interval prolongation and VF [Desai et al. 2003].
In spite of the absence of cardiac events in the present assessment, it must be taken into view that TdP may also occur with lower Q-Tc values or changes; a Q-Tc change as little as 10 ms could be a ‘signal’ that a drug may carry an arrhythmic liability. Essentially there is no established threshold below which prolongation of the Q-T interval is considered free of proarrhythmic danger [Agelink, 2002; Sana et al. 2003]. However, shortening of Q-Tc by olanzapine had not been previously reported in the literature. In essence, little information is known about the issue of drug-induced QT/QTc shortening [Shah, 2010; Holbrook et al. 2009]. Although the variants of SQTS have been expressed as SQT1–SQT5, the number of patients studied with these syndromes is relatively much smaller than the number studied with long QT interval syndrome (LQTS). Therefore, the genotype–phenotype correlations of congenital SQTS are at present not as well characterized as they are for congenital LQTS. This is further aggravated by a lack of currently accepted definitions of what constitutes a short QT interval [Shah, 2010]. However, on the basis of the available data, 360 ms is probably a reasonable value for the lower limit of a normal Q-Tc interval. Studies show that the prevalence of SQTS in the population at large is very low but the risk of VF in those who have a short Q-Tc interval is much higher than normal. In addition, patients with idiopathic VF were found to have shorter Q-T interval at slower HRs, a finding suggestive of arrhythmogenicity [Shah, 2010].
As with QT/QTc prolongation, there are genetic syndromes and pharmaceutical agents which may cause shortening of QT/QTc. Although the potential safety issue of QT/QTc shortening and its suitability as a biomarker of drug-induced cardiac arrhythmias are indistinguishable, the type of arrhythmia associated with prolongation and shortening seems to differ. Prolongation is associated with TdP, whereas it is suggested that shortening of QT/QTc is mainly associated with VF. Current clinical epidemiological evidence suggests that excessive shortening of QT/QTc may facilitate induction of VF [Shah, 2010; Holbrook et al. 2009]. Acquired QT/QTc shortening has been reported to be caused by hypercalcemia, hyperkalemia, hyperthermia, thyrotoxicosis, chronic fatigue syndrome, and myocardial ischemia, which had been totally ruled out in the exclusion criteria. However, variables like sinus arrhythmia and the independent effect of HR on Q-T interval [Ahnve and Vallin, 1982], beat-to-beat variability as a result of modulation of the autonomic nervous system [Mine et al. 2008], or the independent regulatory action of the sympathetic and parasympathetic tone [Harada et al. 2005] must be considered as important factors that steadily influence the Q-T interval. Especially in this regard, both sympathetic and parasympathetic tone appear to contribute to HR-independent changes in QT duration. In the basal state parasympathetic more than sympathetic tone influences the relation QT–HR. Major increases in sympathetic nervous system activity may change the relation QT–HR. Thus, in case of abrupt autonomic changes, any proposed formula for HR correction of QT may be inappropriate, also in the normal range of HR [Cuomo et al. 1997]. The short duration of the study (limited to the period of acute treatment), sex-based sampling, which limits its generalization, lack of a placebo arm, which may have had a significant impact on the assay sensitivity of the study, and a small sample size were among the prominent weaknesses of this trial. Further analogous trials in the future may improve our knowledge of this vital subject.
Conclusion
Olanzapine and risperidone had comparable potentiality for induction of Q-Tc changes, while production of further miscellaneous alterations in ECG was more observable in the olanzapine group. In addition, shortening of Q-Tc was specific to olanzapine.
Footnotes
Acknowledgements
The authors gratefully acknowledge their dear colleagues, H. Kaviani, MD and S. Akbari, MD, and the Department of Research for their practical and financial support of this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.