
Abstract
Introduction:
Asenapine is a novel, recently introduced antipsychotic drug. It has a unique receptor profile and it is licensed in the UK for the treatment of bipolar-affective disorder. However, there is some evidence for its effectiveness in schizophrenia and it is licensed for schizophrenia treatment in a number of countries. Significant numbers of patients within the high-secure hospital setting suffer from treatment-resistant schizophrenia. Many patients fail to respond to adequate antipsychotic trials, and require trials of augmentation with other medications.
Methods:
We report on our experience of using asenapine for augmentation of other antipsychotic medications in two male patients with treatment-resistant schizophrenia and histories of interpersonal violence. The patients provided informed consent to participate in this case series. Data were collected from the patients’ clinical records, incident reports and hospital medical centre records. These records were used to derive primary and secondary outcome measures. These included time spent in seclusion, verbal and physical aggression, numbers of incidents and metabolic parameters. Symptoms were rated pre- and postaugmentation using the Positive and Negative Syndrome Scale (PANSS) and Clinical Global Impression rating scales.
Results:
Both patients showed an improvement after the addition of asenapine. These improvements were characterized by a reduction in global PANSS scores, in the PANSS excitability component, a reduction in scores of violence, overall incidents and reduction in seclusion hours.
Conclusions:
We found asenapine to be an effective augmentation agent with other antipsychotics in both patients. Clinical improvement was noted within weeks. The case-series nature and small sample size limited our ability to draw firm conclusions from our data. However, retrospective analysis has allowed us to take a naturalistic approach that this augmentation strategy may be advantageous on an individual patient basis in a high-secure hospital setting.
Keywords
Introduction
Asenapine is an atypical antipsychotic drug that is in development for the treatment of bipolar-affective disorder and schizophrenia. It has been licensed in the European Union for treatment of moderate-to-severe manic episodes associated with bipolar I disorder. In the USA, asenapine is licensed for use in both schizophrenia and bipolar-affective disorder [Kane et al. 2011].
Asenapine has shown over 65% occupancy of D2 receptors in patients given 6 mg asenapine/day on positron emission tomography studies [Potkin et al. 2007]. Asenapine shows relatively high-binding affinity at serotonin 5-HT2A, 5-HT2B, 5HT2C, 5HT6 and 5HT7 receptors, in addition to dopamine D1, D3 and D4 receptors, and alpha-adrenergic and histaminic receptors. Of note, asenapine has very little affinity for muscarinic receptors, resulting in decreased likelihood of anticholinergic side effects seen with other atypical antipsychotics such as olanzapine or clozapine [Potkin et al. 2007].
The effectiveness of asenapine treatment in acute schizophrenia and longer-term management of schizophrenia has shown promise, particularly in regard to its treatment of negative symptoms of schizophrenia as well as positive reports on the drug’s safety and tolerability [Kane et al. 2011; Potkin et al. 2007].
Broadmoor Hospital is one of three high-secure hospitals in England and Wales. It has a total of 210 beds. Significant numbers of patients within the high-secure hospital setting suffer from complex treatment-resistant schizophrenia. Many patients fail to respond to adequate antipsychotic trials and require augmentation with other medication.
Patients who require short-term management for posing a significant risk to themselves or others are treated in seclusion. If patients present a persistent risk to themselves or others over a lengthy period and do not respond to short periods of seclusion, management with long-term segregation is utilized.
Only three out of a total of approximately 200 patients at Broadmoor Hospital were prescribed asenapine at the time of this report. We chose to focus on only two out of the three patients prescribed asenapine as the final patient on asenapine only was concordant with the medication for a number of days. The same patient stopped all of his oral medications and had a marked deterioration in mental state.
The two patients discussed had failed to respond to previous trials with antipsychotic medication. We wished to examine the efficacy of asenapine as an adjunct treatment for these patients with treatment-resistant schizophrenia and histories of violence in the high-secure hospital setting.
Case reports
Mr X is a mixed-race (white and black British) man in his 40s with a diagnosis of treatment-resistant schizophrenia. He first came into contact with mental-health services at age 24 years and had been treated at a high-secure hospital for the last 2.5 years. At the time of asenapine agumentation, Mr X was treated with clozapine. Mr X had been treated with amisulpride, haloperidol and zuclopenthixol depot in the past. He has a history of substance misuse, with a marked deterioration in mental state reported with cannabis and cocaine. Due to multiple episodes of aggressive behaviour and large amounts of time spent in seclusion, Mr X was transferred from a low-secure hospital, then to a medium-secure hospital and finally to Broadmoor high-secure hospital.
Mr Y is a black British man of West African origin in his 50s, who first came into contact with mental-health services in his early 30s. He was subsequently diagnosed with treatment-resistant schizophrenia. At the time of writing this report, Mr Y had been at Broadmoor Hospital for 9 years. He had not responded to high doses of haloperidol and continued to have grandiose and paranoid delusions. Co-morbidities of impaired renal function and type 2 diabetes limited medication options. Prior to being treated with haloperidol, Mr Y had been prescribed aripiprazole and risperidone. He was transferred from prison to the high-secure hospital setting due to deteriorating mental state. His index offence was rape. Following transfer to the high-secure hospital, Mr Y had carried out a physical assault on his former responsible clinician. Shortly before starting asenapine, Mr Y required transfer from a rehabilitation ward to a high-dependency ward due to an increase in hostile behaviour towards staff and deterioration in mental state, namely increasing severity of persecutory delusions.
The two patients were informed about the case series. Informed consent was sought from the patients. Following interview, patients signed a consent form. The third patient prescribed asenapine at Broadmoor Hospital at the time of this case series was not concordant with asenapine and took the medication for less than 1 week. He was therefore excluded from this report.
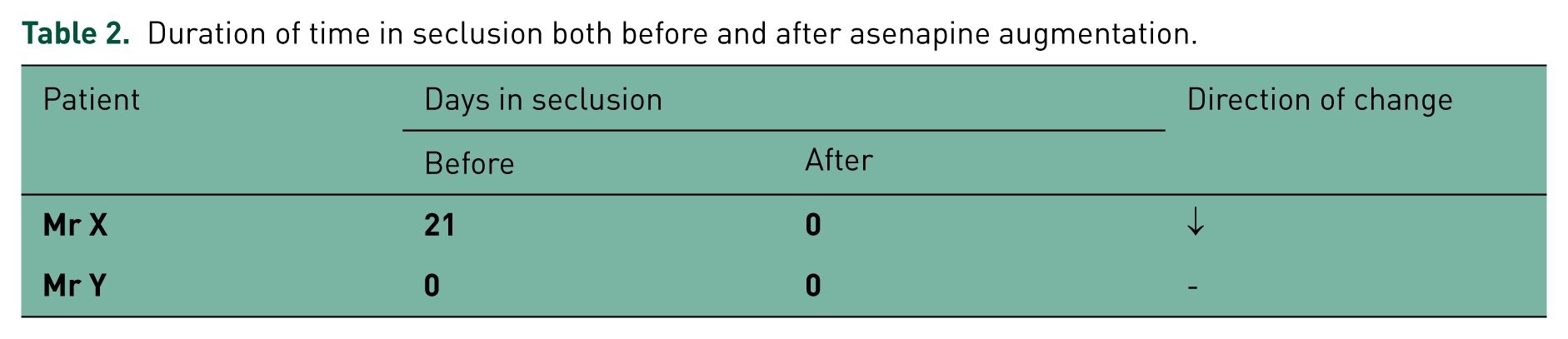
Data were collected from the patients’ clinical records, incident reports and hospital medical centre records. This information has been summarized in Tables 1–3 below. Areas of interest were the amount of time spent in seclusion (Table 2), number and type of incidents recorded (see Figure 1) as well as metabolic parameters (Table 3). Symptoms were rated both before and after asenapine augmentation using the Positive and Negative Syndrome Scale (PANSS) and Clinical Global Impression (CGI) rating scales. Symptoms were rated at 90 days prior to starting asenapine augmentation and 90 days after asenapine augmentation.
Treatment details and results.

BD, twice daily; G, general psychopathology scale; N, negative scale; OD, once daily; P, positive scale.
Duration of time in seclusion both before and after asenapine augmentation.
Metabolic parameters.
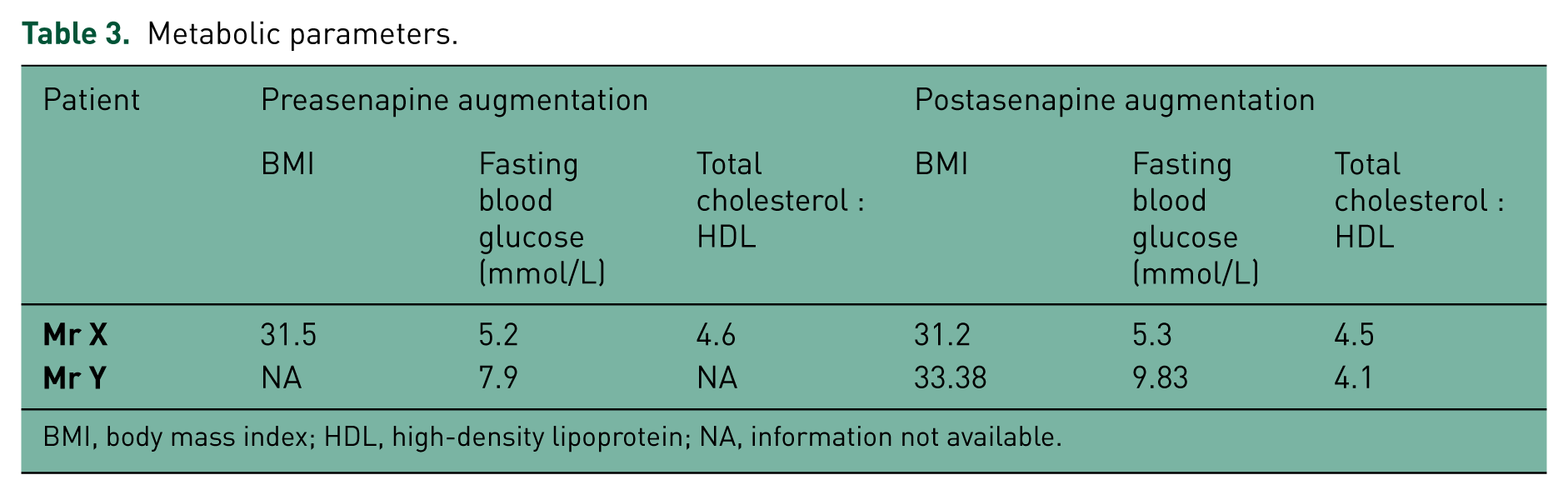
BMI, body mass index; HDL, high-density lipoprotein; NA, information not available.

Number of incidents recorded 90 days before and after asenapine augmentation.
Discussion
We found that augmentation with asenapine was followed within weeks by an improvement in both patients’ PANSS scores in all three domains (positive, negative and global psychopathology scales). A decrease in incident reports of physical aggression was noted for both patients. Verbal aggression incidents decreased in just one of the patients. Both patients’ overall level of dependency appeared to decrease. Mr X’s management in long-term segregation was ended while Mr Y was referred from a high-dependency ward to a rehabilitation ward. (Mr Y remained on a high-dependency ward at the time of writing this report.)
Asenapine did not appear to have a significant impact on either patient’s physical health. Mr X did not have any evidence of weight gain. There was also no significant change in his fasting glucose or cholesterol. Unfortunately not enough information was available to comment on the same parameters for Mr Y. A change in fasting blood glucose was seen in Mr Y from 7.9 mmol/L to 9.83 mmol/L. Mr Y has long-standing type 2 diabetes. The significance of this finding is uncertain. Asenapine appeared to be well tolerated by both patients. Unfortunately, no data were collected on objective measures of extrapyramidal side effects.
With respect to the number of days spent in seclusion, it appeared that Mr X had a decrease in time spent in seclusion (21 days before asenapine augmentation and 0 days after asenapine). However, Mr X’s management changed from seclusion to long-term segregation and thus days spent in seclusion were not counted. This is therefore not a complete picture. However, Mr X did stop being managed in long-term segregation after 89 days of asenapine treatment. These findings are open to researcher bias.
Doses of concurrent psychotropic medications in both patients remained the same throughout the 180 days of this report.
Conclusion
It is not possible to establish a causal link between asenapine augmentation and the clinical improvements we observed in our small sample size of patients. This case series was not compared with patients with similar presentations on first-line treatments. Conducting such a case series may be helpful in gaining more certainty on the efficacy of asenapine augmentation.
Our observations only took place over a period of 180 days (half prior and half following asenapine augmentation). This is a relatively short period of time considering the duration of both patients’ hospital stays.
We conclude that asenapine augmentation may be advantageous on an individual patient basis in a high-secure hospital setting.
Footnotes
Acknowledgements
The authors would like to state that some of the information contained in this article submission was presented on an educational poster at the Faculty of Forensic Psychiatry Annual Conference in Belfast (5th-7th March 2014). This article has not been published in another journal, is not in press and has not been submitted to another journal or elsewhere.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.