
Abstract
Introduction:
Patient support programmes are assuming greater importance in the UK in many therapeutic areas, mostly with the aim of improving adherence to medication and many being provided by the pharmaceutical industry. Atomoxetine is a noradrenaline reuptake inhibitor for the treatment of attention deficit hyperactivity disorder that has recently demonstrated incremental efficacy for at least 12 weeks. Issues of adherence may be predicted over this initial period particularly if adverse events are reported. The Strattera Support Service was initiated in 2006 ( funded by Eli Lilly) to provide advice, initially through telephone contact, by trained nurses during the first 12 weeks of atomoxetine therapy and is offered to carers of patients diagnosed with ADHD after atomoxetine has been prescribed. The aim of this pilot service evaluation is to assess discontinuation rates and compare them with historical control data.
Methods:
Data from patients in the service who initiated atomoxetine between 1 January 2009 and 31 March 2010 were analysed to provide a pilot service evaluation. Continuation rates of patients in the service who were taking atomoxetine at week 12 were assessed and compared with historical control data.
Results:
Between 1 January 2009 and 31 March 2010, 346 patients (300 male patients) enrolled in the programme and commenced treatment with atomoxetine. The mean age of patients was 10.5 years. At 12 weeks, 33 (9.5%) patients had discontinued treatment; continuation rates were similar regardless of age and sex. Discontinuation rates of 39% are reported from historical control data.
Conclusions:
Preliminary data from a 12-week atomoxetine patient support programme are supportive that discontinuation rates may be lower than historically expected. Further service evaluations of this programme may be required.
Introduction
Atomoxetine is a nonstimulant medication for attention deficit hyperactivity disorder (ADHD) that has been licensed for use in children and adolescents since 2004 in Europe [Savill and Bushe, 2012]. ADHD is a common neurodevelopmental disorder which is being increasingly recognized, diagnosed and treated, and data from the UK General Practice Research Database demonstrated that the prevalence of prescriptions for methylphenidate, atomoxetine and dexamfetamine in a sample of 1636 patients increased 6.23 fold between 1999 and 2006 [McCarthy et al. 2009] There are seven currently licensed and available medications in the UK to treat ADHD: atomoxetine (Strattera®, Eli Lilly & Company Ltd, Basingstoke, UK), dexamfetamine, two short-acting preparations of methylphenidate (Ritalin®, Novartis Pharmaceuticals Ltd, Camberley, UK, Medikinet®, Flynn Pharma Ltd, Dublin, Ireland) and three long-acting preparations of methylphenidate (Concerta XL®, Janssen-Cilag Ltd, High Wycombe, UK, Equasym XL®, Shire Pharmaceuticals Ltd, Basingstoke, UK and Medikinet XL®, Flynn Pharma Ltd, Dublin, Ireland). Atomoxetine and methylphenidate are the commonest of these prescribed medications in ADHD, with clinical trials demonstrating differential response rates. Newcorn and colleagues, for example, showed that in 44% of patients their ADHD responded to either medication, whereas in 43% their condition responded to atomoxetine having failed to respond to methylphenidate, and in 42% it responded to methylphenidate having failed to respond to atomoxetine [Newcorn et al. 2009]. In a noninferiority meta-analysis of comparative clinical trials of at least 6 weeks’ duration, atomoxetine and methylphenidate were both associated with similar responder rates (>40% reduction in ADHD Rating Scale) of 53.6% and 54.4%, respectively, with atomoxetine demonstrating noninferiority to methylphenidate [absolute difference −0.9%, 95% confidence interval (CI) −9.2% –7.5%] [Hazell et al. 2010]. A recent systematic review of atomoxetine data between 2009 and 2011 conducted by two of the named authors also concluded that clinical parity exists in clinical trials comparing atomoxetine and methylphenidate when confounders are addressed [Bushe and Savill, 2011].
Despite atomoxetine having an onset of action on core ADHD symptoms that commences within the first few weeks, there is increasing evidence that the maximal efficacy may not be seen for 10–12 weeks, and there is some evidence from pooled analyses showing a 96% probability of robust improvement at 52 weeks [Dickson et al. 2011; Montoya et al. 2009; Svanborg et al. 2009].
In clinical usage this may mean that adverse effects are reported earlier than improvement can be measured and consequently treatment could potentially be discontinued early either due to apparent lack of efficacy or adverse events. Adverse events are common in atomoxetine- and placebo-treated cohorts. For example, in a 12-week placebo-controlled trial in a treatment-naïve population, decreased appetite was reported in 27% of patients on atomoxetine and 7.8% of those on placebo [Montoya et al. 2009] (Table 1). Total treatment-related adverse events were reported in this study in 65% of patients on atomoxetine and 37.3% of those on placebo, with the most common adverse events being decreased appetite and somnolence. To address the issue of possible early cessation of treatment with atomoxetine, the Strattera Support Service (SSS) was set up in 2006 in the UK to support carers of child and adolescent patients with ADHD for 12 weeks after initiation of treatment with atomoxetine, with the aim of reducing discontinuations from therapy [Lenox-Smith et al. 2011b]. This nurse-led service assists in the management of adverse effects of treatment and helps manage expectations appropriately in the initial phase of treatment.
Incidence of treatment-related adverse events [data from Montoya et al. 2009].

Patient support programmes (PSPs) are usually initiated by pharmaceutical companies with the aim of optimizing treatment and improving outcomes and are becoming increasingly used. Patient safety is a critical component of such programmes. Adverse events are not surprisingly reported more often in programmes with telephone support and there are strict protocols for adverse event reporting which enables pharmacovigilance requirements to be adhered to. That potential adverse events may be reported has been demonstrated in a trial of duloxetine alone compared with duloxetine plus telephone intervention. While there was no statistically significant difference between groups on the primary outcome measure of remission, more adverse events were reported in patients receiving the telephone support service [Perahia et al. 2008].
Guidance notes on PSPs have been developed by the Association of British Pharmaceutical Industry (ABPI) Pharmacovigilance Expert Network (PEN) and shared with the Medicines and Healthcare Products Regulatory Agency (MHRA). Within the guidance provided, a patient support programme is defined as a service for direct patient or patient–carer interaction/engagement designed to help manage medication and/or disease outcomes such as adherence, awareness and education, or to provide healthcare professionals with support for their patients [ABPI, 2011].
There are three main types of patient support programmes: compliance programmes, when the consenting patient is contacted on an agreed basis to provide them with support; call centre programmes, when the patient makes contact requiring advice or information; and nurse educator programmes, when nurses are employed by the company, often via a third party, to directly interact with patients to aid adherence and other aspects of treatment. The SSS is an example of both the first and third type of programme combined, when trained nurses offer support around the medication prescribed, in this case, atomoxetine. The provision of patient support services to aid adherence to medications or provide aspects of care such as physical health programmes in severe mental illness have been increasing over the past decade. Examples include an osteoporosis patient support programme provided by Servier Laboratories Ltd intended to improve adherence and prevent unnecessary early treatment discontinuation through an interactive service with nursing support [Servier, 2010]. Other models differ with online provision of information and treatment diaries. Pharmacists may also be involved in the provision of patient support programmes designed to improve adherence to medications [http://www.lpc-online.org.uk/bkpage/files/178/whitepaper/az__mmm_programme_sunderland_110908.pdf (accessed 16 October 2012)]. Over the past decade, there have been several examples of successful interventions using such programmes. Some of these programmes have led to the publication of data evaluating the service providing longer-term outcome data. The Well Being Support service provided a physical health intervention to almost 1000 patients with all forms of severe mental illness in the UK, provided weight management clinics and demonstrated significant reductions in both weight and cardiovascular risk factors [Smith et al. 2007].
The SSS is described below and preliminary pilot data are presented on medication discontinuation rates over 12 weeks during this programme [Lenox-Smith et al. 2011b].
The Strattera Support Service
This is a national post-prescription support service for carers of children and adolescents who have been prescribed atomoxetine to treat ADHD. Any enrolled clinician can offer this service after the decision to prescribe atomoxetine has been made. Nurse advisers, employed by Quintiles UK on behalf of Lilly, provide an ongoing service consisting of telephone calls throughout the initial 12 weeks of treatment. The contact frequency is agreed with the carers on initial contact following a baseline assessment.
The service is split into five distinct phases.
Phase 1: clinician sign up.
In this phase the clinician signs a service authorization document which enables the two SSS nurses to work with the carers of the clinician’s patients. This document acts as a contract between Quintiles and the clinician and clarifies the scope of the service.
Phase 2: clinician engagement.
In this phase the nurse sits down with the clinician and looks at the practicalities of how the service is going to work. This will include everything from the referral process to communication between the nurse and the clinician to formalizing processes covering untoward incidents that may occur during the service.
Phase 3: carer referral.
The service is intended to be an integral part of the Strattera package. When an enrolled clinician prescribes atomoxetine they may also consider, in conjunction with the patient and their carer, whether the support service is an appropriate option. If considered useful, the support service is discussed with the patient and their carer and consent is obtained to refer the carer into the service.
Phase 4: service delivery.
When a referral is received into the support service a welcome pack is sent out to the carer advising what can be expected from the service. A nurse is allocated to and makes contact with the carer to welcome them into the programme and to determine the agreed level of support to be offered throughout the 12-week programme. The support service at the time of the collection of the data described here was restricted to phone calls but has since been expanded to include newsletters and motivational and reminder text messages which can be opted out of at any time.
During the current 12-week programme the carer will on average receive six calls of approximately 15 min duration, six newsletters, two motivational texts per week and two reminder texts per appointment. The calls, newsletters and texts mirror the themes of the first 12 weeks on atomoxetine and will include topics such as side effects, efficacy and daily routine.
At the end of the 12 weeks the carer completes a satisfaction survey to provide feedback on the service.
Phase 5: clinician feedback.
The final phase occurs when the nurse ensures that the clinician has received feedback on the carers referred into the service. If atomoxetine has been stopped the clinician receives a discontinuation letter advising how long the carer was in the service and the reason for discontinuation. If the carer completes the 12-week service the clinician receives a discharge summary advising how the carer progressed through the 12 weeks, any issues that had been discussed and the outcomes achieved. During this final phase the clinician also feeds back on their experience of using the service.
The Lilly Global Patient Safety team trains the SSS nurses annually on the capturing and reporting of all adverse events which are raised through the interactions with the carers.
The following sections describe outcomes from the service offered at the time when newsletters and text messages had not been introduced.
Methods
Data are presented descriptively without formal statistics and represent a service evaluation and not any form of clinical research. Data from all patients who initiated atomoxetine in the service between 1 January 2009 and 31 March 2010 were available for analysis. Patients who were enrolled in the service but did not start atomoxetine were not included in the analysis. Continuation rates were assessed at week 12 and were defined as the number of patients in the service who were taking atomoxetine at that stage.
Patients were considered adherent if they reported taking atomoxetine at week 12 regardless of whether treatment had been interrupted prior to week 12. Continuation rates from the service were then compared with historical market research data provided by the market research company Cegedim. From the 450 practices in Primary Care using InPS Vision clinical software, Cegedim selected 150 of the practices most representative of UK regional populations. Data from these practices include duration of therapy. Cegedim considers a patient to be adherent if they return for repeat prescriptions within 1.5 times the expected duration of their previous prescription [Lenox-Smith et al. 2011a]. This historical data set was then compared with data from the SSS.
Results
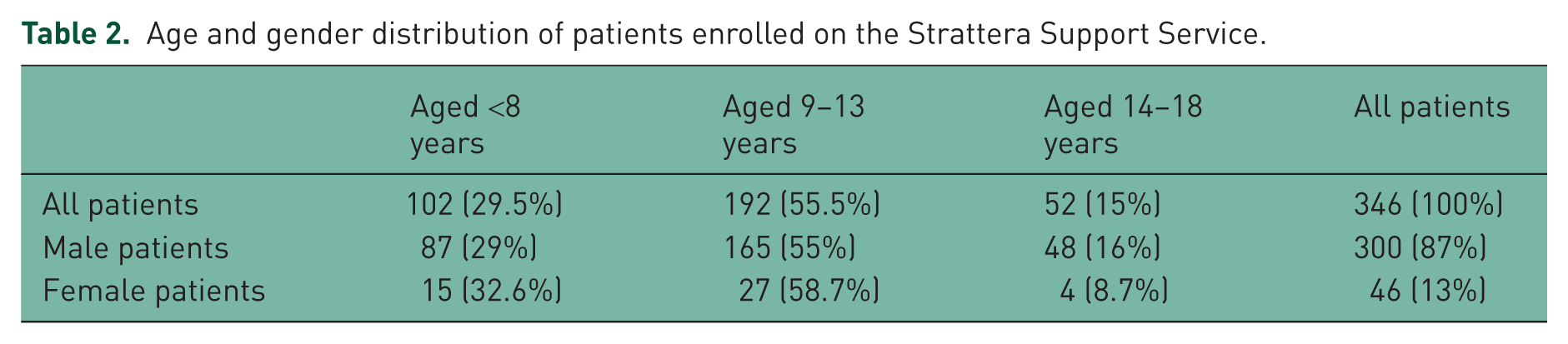
Between 1 January 2009 and 31 March 2010, 346 patients (300 male/46 female) starting atomoxetine were enrolled by their carers into the service. Table 2 shows the breakdown of enrolled patients by age and sex. Continuation rates by age are presented in Figure 1 [Lenox-Smith et al. 2011a]. At 12 weeks, 33 (9.5%) patients had discontinued atomoxetine, giving a noncontinuous compliance rate of 90.5% with continuation rates similar regardless of age and sex. Naturalistic data collected by Cegedim in July 2009 demonstrated a 12-week compliance rate for atomoxetine of 61% [Lenox-Smith et al. 2011b].
Age and gender distribution of patients enrolled on the Strattera Support Service.

Patient compliance at week 12 by age and sex.

Patient compliance at week 12 on the Strattera Support Service (SSS) compared with naturalistic data.
Discussion
Medication adherence is a well recognized issue with most treated disorders and types of medication. When the key behaviours of a disorder include disorganization, forgetfulness, distractibility and lack of attention, it may potentially be more of an issue. The use of a patient support programme offered through the initial stages of treatment may assist in addressing issues of nonadherence. Patients enrolled into the SSS reported higher rates of noncontinuous compliance during the first 12 weeks of therapy than comparative rates reported in naturalistic, retrospective data. The authors are unaware of any additional data that can be cited on discontinuation rates at 12 weeks in naturalistic cohorts.
A feature of the SSS which may be of particular benefit to carers and patients is the employment of qualified dual-trained nurses (registered general nurse/registered mental nurse), trained in both mental illness and the use of psychological techniques to deliver ongoing support.
Adherence to medication should lead to improved outcomes for those patients. Our service evaluation data are both descriptive and preliminary; further research may be necessary to evaluate the degree to which the SSS is associated with low discontinuation rates and subsequent improvement in clinical outcome. Research into the efficacy of patient support programmes is now becoming feasible [A’Campo et al. 2011].
There are several limitations of this analysis that need to be factored into any interpretation. There was no randomization and the two compared populations are likely to be different. No further information is available on the Cegedim population. This analysis measured adherence as the number of patients in the SSS who were taking atomoxetine at week 12. However, patients may have stopped and restarted their medication prior to week 12 and these data are unknown. There was no assessment of the correlation between frequency of contact and continuation, thus it is not possible to factor in the importance of frequency of contact and how this may relate to differing continuation rates. There may have been some bias in patient selection. Healthcare professionals may either preferentially select patients for the service who were more likely to comply with medication and a patient support service or alternatively offer the service to those in whom the perceived risk of poor adherence may be highest. Either way, such patient selection could have influenced the outcomes. Further study is thus needed to understand the independent variables which may impact on the outcomes of this patient support programme.
What is certain, however, is that patient support programmes are likely to grow in importance, may be initiated outside of the pharmaceutical industry and new types of programmes may be trialled. The development of all types of patient support programmes along with initiatives such as Telehealth and Telecare technology, which provide healthcare to patients with long-term health conditions, should enhance the care and support offered to patients with health needs, and hopefully improve individual outcomes.
Conclusion
The SSS is a nurse-led patient support programme which appears to reduce discontinuation rates from atomoxetine by offering support and advice to carers of patients with ADHD during the initial 12 weeks of treatment.
Footnotes
Acknowledgements
The authors would like to acknowledge Sabine Dahlen and Yvonne Parkinson (Quintiles UK) for their ongoing contribution to the running of the Strattera Support Service.
Funding and Conflict of interest statement
NS, ALS and CB are employees and shareholders of Eli Lilly who is the marketing authorization holder and manufacturer of atomoxetine in the UK and has financed this manuscript. JP is the nurse manager employed by Quintiles UK who manages the Strattera Support Service on behalf of Lilly.